ABSTRACT
OBJECTIVES: to investigate the relation between age at menarche and gestational weight gain.
METHODS: cross-sectional study, with 2609 women from "Projeto VIVER: desfechos em saúde nos períodos perinatal e neonatal" (VIVER Project: "Health outcomes in the perinatal and neonatal periods). Outcome: gestational weight gain; independent variable: age at menarche. Descriptive analysis with prevalence presentation (CI95%). To test the association between weight gain and menarche, Poisson regression was applied.
RESULTS: early menarche (< 12 years) occurred in 21.9% of the sample (CI95%=20.3-23.4). In the group with early menarche, 43.7% presented pre-gestational overweight, 85.6% post-pregnancy overweight and 36.8% had excessive gestational weight gain. Early menarche increases the risk of excessive gestational weight gain by 33% (aPR= 1.33; CI95% = 1.05-1.69).
CONCLUSIONS: early menarche is related to excessive gestational weight gain. Educational actions to prevent overweight in prenatal consultations should be prioritized, especially among women with early menarche.
Keywords:
Menarche, Gestational weight gain, Body weight
RESUMO
OBJETIVOS: investigar a relação entre a idade da menarca com o ganho de peso gestacional.
MÉTODOS: estudo transversal com 2609 mulheres do Projeto VIVER “Desfechos em saúde nos períodos perinatal e neonatal”, tendo como desfecho o ganho de peso gestacional e como variável independente a idade da menarca. Análise descritiva com apresentação da prevalência (IC95%). Para testar a associação entre ganho de peso e menarca, aplicou-se regressão de Poisson.
RESULTADOS: menarca precoce (< 12 anos) ocorreu em 21,9% da amostra (IC95%= 20,3-23,4). No grupo com menarca precoce, 43,7% apresentaram sobrepeso pré-gestacional, 85,6% sobrepeso pós-gestacional e 36,8% tiveram ganho de peso gestacional excessivo. Menarca precoce aumentou o ganho de peso gestacional excessivo em 33% (RPa= 1,33; IC95%= 1,05-1,69).
CONCLUSÕES: menarca precoce está relacionada ao ganho de peso gestacional excessivo. Ações educativas de prevenção ao sobrepeso nas consultas de pré-natal devem ser priorizadas, principalmente entre mulheres com menarca precoce.
Palavras-chave:
Menarca, Ganho de peso na gestação, Peso corporal
IntroductionMenarche, the first menstrual period, is a factor of great importance, as it is related to a woman’s physiological development,
1 and is considered a marker of global importance.
2 In this sense, menarche functions as a milestone in female sexual maturation, which will be influenced by exposures throughout life, modulating future health events.
3 On average, menarche occurs around the age of 12, but a secular reduction in its age has been observed
4,5 one of the explanations is the increase in overweight children and adolescents.
5,6 Thus, early menarche (<12 years)
7 is positively related to overweight, which tends to persist into adulthood,
6,7 as well as being compatible with an increased risk of breast cancer,
8,9 ovarian cancer
10 and depression.
11In addition to the relation between the reduction in the age of menarche and overweight, at a global level, the trend in the Body Mass Index (BMI) shows an increase in weight values in relation to height.
12 The reasons for the occurrence of this event are mainly related to sedentary lifestyles and eating habits, such as increased consumption of food rich in salt, sugar and fat, as well as hormonal and genetic factors.
13Excess weight in the female population
14,15 can have an impact on women’s quality of life and on their reproductive health and that of their offspring.
13 Weight gain is quite common during pregnancy. However, there is an increase in overweight and obesity among pregnant women,
16-18 since pre-pregnancy overweight increases the risk of excessive weight gain during pregnancy.
19 Excessive gestational weight gain (GWG) can cause not only metabolic problems for the mother, but also an increased risk on hypertensive syndromes, gestational diabetes mellitus (GDM), as well as unfavorable perinatal outcomes, such as an increased risk of macrosomia, hyperbilirubinemia, hypoglycemia and childhood obesity.
20-22Thus, this study justifies the necessity to verify the relation between early menarche and excessive GWG, since discovering the relation, it can help develop strategies in pregnant women gain adequate weight, especially those with early menarche, thus contributing to a better quality of life for the mother-child binomial. With this in mind, we investigated the relation between age of menarche and GWG.
MethodsThis is a cross-sectional study from a prospective cohort, “
Projeto VIVER: desfechos em saúde nos períodos perinatal e neonatal”, (VIVER Project: Health outcomes in the perinatal and neonatal periods) which was a general objective to analyze the influence of early determinants on morbidity and mortality in the perinatal and neonatal periods in the Metropolitan (Maternities 1 and 3) and North (Maternity 2) health regions in the State of Espírito Santo, Brazil. The criteria for choosing the maternity hospitals in the original study were: were located in one of the health regions, carrying out a greater number of births and having a greater diversity of care (80 to 100% by the
Sistema Único de Saúde (SUS) (Public Health System) 100% private or by health plan).
23 The project began in August 2019 and ended in March 2020. It was monitored in three stages. In the maternity, visits were daily to identify women who had given birth during this period, with a questionnaire covering sociodemographic, maternal and family characteristics, reproductive history, preconception health, prenatal care, labor and birth care being applied; early and late neonatal follow-ups were carried out by telephone with mothers after completing seven and 27 days of birth, respectively. More information can be found in the research in the methodological article.
23This present study used only the data collected during the follow-up in the maternity, totaling 3,435 women. The inclusion criteria were all pregnant women who provided information about the age of menarche, pre-gestational weight, post-gestational weight and gestational weight gain, totaling 2,609. The exclusion criteria were: twins, prematurity and negative gestational weight gain.
BMI was calculated from the weight and height values, whose formula is [mass (Kg)/height (m)
2]. The classification used to assess BMI was the one recommended by the World Health Organization (WHO),
24 in which BMI < 18.5 kg/m
2 - thin or underweight; BMI 18.5-24.9 kg/m
2 - normal or eutrophic; BMI 25-29.9 kg/m
2 - overweight or pre-obese; BMI >30 kg/m
2 - obese. The calculation for GWG was: [(weight at last prenatal visit)-(weight at first prenatal visit)]. For the classification of GWG, the guideline used was the one recommended by the Institute of Medicine (US) and National Research Council (US) Committee to Reexamine IOM Pregnancy Weight Guidelines,
25 which recommends weight gain between 12.5-18.0 kg for mothers classified by pre-gestational BMI as underweight, 11.5-16.0 kg for those with eutrophic weight, 7-11.5 kg for overweight and 5.0-9.0 kg for obese mothers.
The statistical program Stata, version 12.1, was used to analyze the data. The variables were categorized as follows: age in complete years: ≤19, 20-34 and ≥35; self-reported skin color: mixed, white, black, yellow and indigenous; schooling in complete years of study: 1-8, 9-11 and ≥12; marital status with or without a partner; family income (Reais) in quintiles, where 1 represented the lowest income and 5 the highest income; age of menarche in years: <12, 12-14 and ≥15; smoking during pregnancy: yes/no; physical activity: yes/no; gestational diabetes: yes/no; start of prenatal consultations in trimester: 1
st, 2
nd and 3
rd; number of prenatal consultations: <7 and ≥7; gestational age: term (≥ 37 to < 42 weeks) and post-term (≥ 42 weeks); pre-gestational nutritional status classified by BMI; height in meters (m); pre- and post-gestational weight and GWG were adopted in kilograms (Kg).
For the variables height, pre- and post-gestational weight and GWG, the means and their respective confidence interval values (CI95%) were estimated. The association between the categories of age of menarche and the outcome was verified by Poisson regression, with the risk estimator being the prevalence ratio (PR). For pre- and post-gestational BMI, a comparison was made between the “increased” (BMI classified as overweight and obese) and “adequate” (BMI classified as eutrophic and underweight) groups. For GWG, the “inadequate” (weight gain above that recommended by the IOM),
25 and “adequate” groups were compared with age of menarche. The crude and adjusted PR values were estimated, and the variables used for adjustment were: age, reported skin color, mother’s schooling, living with a partner, income quintile, smoking and physical activity during pregnancy and pre-gestational diabetes. Bivariate analysis was carried out to check for associations between the variables age at menarche (independent variable) with pre- and post-gestational weight and GWG (dependent variables), with a significance level set at 5%.
The study was approved by the Human Research Ethics Committee of
Universidade Vila Velha (CAAE no. 02503018.0.0000.5064) and by the Human Research Ethics Committees of the maternity hospitals involved.
ResultsThe final sample consisted of 2609 participants, after excluding preterm pregnancies (N=140), twin pregnancies (N=72) and pregnancies that had a negative GWG (N=39).
Most of the sample was made up of women aged between 20 and 34 (70.0%), with self-reported white skin color (51.6%), 12 or more years of schooling (61.4%), with a partner (87.4%) and income in the 2
nd quintile (30.6%). Early menarche occurred for 21.9% of the women, with an average of 12.7 years (data not shown). Regarding information on lifestyle habits and pregnancy, 94.1% said they had not smoked during pregnancy, 79.7% said they did not practice physical activity, 89% did not have gestational diabetes, 70.1% were in the first trimester of pregnancy when they began prenatal care, 80.2% had seven or more prenatal consultations, 99.6% had full-term gestational age. As for nutritional status, 54.4% of the women were eutrophic at the beginning of pregnancy. The average height of the mother, pre- and post-gestational weight and the GWG were respectively: 1.62 m; 65kg; 77.3kg; 12.3kg (Table 1).
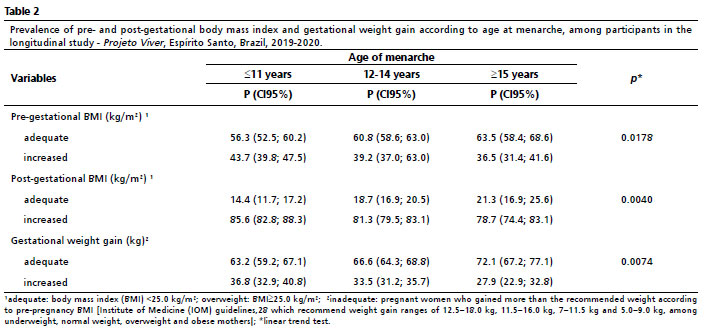
Among the group who had an early menarche (<12 years), 43.7% (CI95%) = 39.8-47.5) were pre-pregnancy overweight, 85.6% (CI95%) = 82.8-88.3) were post-pregnancy overweight and 36.8% (CI95%) = 32.9-40.8) had excessive GWG (Table 2).
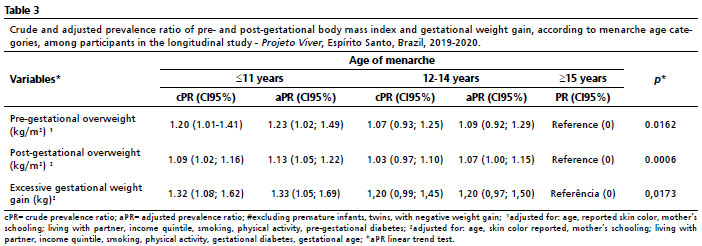
There was practically no variation, indicating that the adjustment variables did not interfere with the relation. Women with early menarche (<12 years) had a 23% (CI95% = 1.02-1.49) higher risk of pre-pregnancy overweight, 13% (CI95% = 1.05-1.22) of post-pregnancy overweight and 33% (CI95% = 1.05-1.69) of excessive GWG, compared to those with late menarche (≥15 years) (Table 3).
DiscussionThe main finding of the study was that women with early menarche (<12 years) had a higher risk of having excessive GWG, pre- and post-gestational overweight, compared to the group with late menarche (≥ 15 years), even adjusting for factors that could interfere with this relation.
These results corroborate to the findings of a prospective cohort study with a dynamic sample, from 2005 to 2007, carried out in a Basic Health Unit in Ilha do Governador, Rio de Janeiro, Brazil, which analyzed the relationship between various factors, including reproductive factors, and changes in weight during pregnancy
26. The participants’ characteristics were similar to this study, with a mean age of 25.7 years and a mean age of menarche at 12.6 years. However, the pre-gestational BMI was lower, as 33.4% were overweight (BMI ≥25 kg/m
2). Although the age of menarche in the study in Rio de Janeiro was assessed linearly, there was an increase in GWG as the age of menarche decreased (β: -2.4).
26 With regard to GWG, a retrospective cohort on mothers and daughters in California, USA, showed that excessive GWG can be harmful to the women’s offspring. The study assessed the impact of GWG on offspring, which found a relation between the daughters’ time of sexual maturation and the mothers’ GWG. The daughters of mothers whose GWG was excessive had an 80% higher risk of having early telarche, compared to the daughters of mothers who had an adequate GWG.
27In relation to the age of early menarche (<12 years), the study obtained similar results to others carried out in Brazil.
5,6,13 The reduction in the age of menarche is a trend observed in Brazil and other countries. One study systematically mapped the trend in the age of menarche in cohorts from 27 low- and middle-income countries, using 16 global fertility surveys, 28 demographic surveys
1 and health surveys, and found that the average age of menarche in cohorts from 1932 was 14.7 years, while in cohorts from 2002, the average was 12.9 years.
1 Colombia, one of the countries evaluated and located in South America, showed a reduction in the age of menarche, from 13.5 years in 1976 to 12.8 years in 2015.
1Although genetic and environmental factors play an important role in determining girls’ sexual maturation, nutritional quality plays a key role in this process. A meta-analysis
28 published in 2020 identified the relation between nutritional standards and the age of menarche. A higher risk of early menarche (<12 years) was associated with a diet rich in 232% carbohydrates, 215% animal protein, 20% iron and 25% polyunsaturated acids. Eating 1g/day of animal protein at childhood brought the age of menarche forward by approximately two months (β: -0.13).
This study also observed that pre-gestational BMI classified as overweight was higher in the group of women with early menarche (<12 years) when compared to the group with late menarche (≥15 years). On birth cohort in 1982 in Pelotas, RS,
6 early menarche (<12 years) was positively associated with fat mass index (2.33 kg/m
2), but in the cohort in 1993, when the researchers adjusted the variables for BMI at 11 years of age, the association with fat mass index was reduced from 2.2 kg/m
2 to 0.26. The researchers concluded that overweight in childhood is related to early menarche and that such overweight tends to accompany women into adulthood.
6 In this sense, the overweight acquired influences the cardiovascular health on these women, increasing the risk of diseases such as hypertension, diabetes and abdominal fat (15% to 30%). Another study carried out at
Hospital Israelita Albert Einstein assessed pre-gestational BMI, GWG, and associated maternal and fetal complications in the population of pregnant women attended at the
Programa Gestação Saudável.
20 (Healthy Pregnancy Program). The participants were an average of 30.2 years old, with an average pre-gestational BMI of 25.3 and an average GWG of 11.4 kg. The researchers found that having an early menarche increased the risk of gestational diabetes mellitus to 7.5 times.
This study analyzed the relation between the age of menarche and GWG. The results showed that the group with early menarche was more likely to be overweight before and after pregnancy and to have excessive GWG. In view of this, it can be assumed that the onset of the early reproductive cycle, marked by menarche before the age of 12, may be triggered by reproductive hormones and this event may lead to the accumulation of body fat, especially in the gluteal femoral region.
29 This assumption deserves attention, since the secular age of menarche shows a downward trend in different populations worldwide
1,7 and obesity is on the rise and is considered a global public health problem.
12,13,16-18Regarding to the limitations of the study, the age of menarche was collected using the recall method, based on the participant’s memory. However, the bias presented by this method is small, as it is a very important moment in a woman’s life. In addition, a study carried out with women belonging to the Newton Girls Study obtained a strong correlation between recalling the age of menarche (r = 0.79;
p<0.001) even 30 years after the event.
30As for early menarche being associated with overweight, the study has a reverse causality bias, as it was not possible to verify whether overweight occurred before or after early menarche, making it difficult to establish the temporal sequence between the supposed cause and effect. Another limitation was the availability of information on the necessary variables for the study: some women did not provide information on their pre-gestational weight, age of menarche, others had a negative GWG, preterm and twin pregnancies; for this reason, they were excluded from the sample, leaving only those participants who provided valid data for the study to take place; however, this situation did not lead to low representativeness in the final study sample. However, the study maintained a high sample size and the baseline characteristics showed no differences between the age of menarche groups compared. Except for age, since those who menstruated before the age of 12 had a higher prevalence of age under 20 than the other menarche age categories (12-14; >15).This reinforces the secular downward trend in the age of menarche, in which younger women menstruate earlier and tend to have greater adiposity.
Finally, it can be concluded that the occurrence of menarche at the age of 12 or earlier is related to overweight. In addition, this group is at greater risk of excessive GWG during pregnancy, the consequences of which extend to the mother-child binomial. Despite the evidence from this and other studies and the large sample for such an analysis, this finding should be interpreted with caution, since the study was carried out in maternities and may not represent the randomness found in population studies. This information could help to promote improvement in the care provided for pregnant women during prenatal care, favoring better planning to achieve favorable outcomes.
References1. Leone T, Brown LJ. Timing and determinants of age at menarche in low-income and middle-income countries. BMJ Global Health. 2020 Dec; 5 (12): e003689.
2. Sommer M, Sutherland C, Chandra-Mouli V. Putting menarche and girls into the global population health agenda. Reprod Health. 2015 Mar; 12 (1): 24.
3. Deardorff J, Berry-Millett R, Rehkopf D, Luecke E, Lahiff M, Abrams B. Maternal Pre-pregnancy BMI, Gestational Weight Gain, and Age at Menarche in Daughters. Matern Child Health J. 2012 Oct; 17 (8): 1391-8.
4. Pathak PK, Tripathi N, Subramanian SV. (Secular Trends in Menarcheal Age in India-Evidence from the Indian Human Development Survey. PLOS ONE. 2014; 9 (11): e111027.
5. Barros BS, Kuschnir MCMC, Bloch KV, Silva TLN. ERICA: age at menarche and its association with nutritional status. J Pediatr. 2019 Jan; 95 (1): 106-11.
6. Bubach S, Menezes AMB, Barros FC, Wehrmeister FC, Gonçalves H, Assunção MCF,
et al. Impact of the age at menarche on body composition in adulthood: results from two birth cohort studies. BMC Public Health. 2016 Sep 22; 16 (1).
7. Lee HS. Why should we be concerned about early menarche? Clin Exper Pediatr. 2021; 64 (1): 26-7.
8. Admoun C, Mayrovitz HN. The Etiology of Breast Cancer. In: Mayrovitz HN, editor. Breast Cancer. Brisbane (AU): Exon Publications; 2022. p.21-30. [
Internet]. [acesso em 2022 Sep 28]. Disponível em:
https://exonpublications.com/index.php/exon/article/view/breast-cancer-etiology9. Song SS, Kang S, Park S. Association of Estrogen-Related Polygenetic Risk Scores with Breast Cancer and Interactions with Alcohol Intake, Early Menarche, and Nulligravida. Asian Pacific J Cancer Prev. 2022 Jan; 23 (1): 13-24.
10. Nash R, Johnson CE, Harris HR, Peres LC, Joslin CE, Bethea TN,
et al. Race Differences in the Associations between Menstrual Cycle Characteristics and Epithelial Ovarian Cancer. Cancer Epidemiol Biomarkers Prev. 2022 Jun; 31 (8): 1610-20.
11. Hirtz R, Libuda L, Hinney A, Föcker M, Bühlmeier J, Holterhus P-M,
et al. Age at menarche relates to depression in adolescent girls: Comparing a clinical sample to the general pediatric population. J Affect Dis. 2022 Dec; 318: 103-12.
12. Silva LES, Oliveira MM, Stopa SR, Gouvea ECDP, Ferreira KRD, Santos RO,
et al. Tendência temporal da prevalência do excesso de peso e obesidade na população adulta brasileira, segundo características sociodemográficas, 2006-2019. Epidemiol Serv Saúde. 2021; 30 (1).
13. Gonçalves DF, Teixeira MTB, Silva GA, Duque KCD, Machado MLSM, Ribeiro LC. Fatores reprodutivos associados ao excesso de peso em mulheres adultas atendidas pela Estratégia Saúde da Família. Ciênc Saúde Colet. 2020 Aug; 25 (8): 3009-16.
14. Kanter R, Caballero B. Global gender disparities in obesity: a review. Adv Nutr. 2012 Jul; 3 (4): 491-8.
15. Silva AG, Andrade FMD, Ribeiro EG, Malta DC. Temporal trends of morbidities, and risk and protective factors for noncommunicable diseases in elderly residents in Brazilian capitals. Rev Bras Epidemiol. 2023; 26: e230009.
16. Flannery C, Mtshede MN, McHugh S, Anaba AE, Clifford E, O’Riordan M,
et al. Dietary behaviours and weight management: A thematic analysis of pregnant women’s perceptions. Matern Child Nutr. 2020 Apr 30; 16 (4).
17. Monteschio LVC, Marcon SS, Arruda GO, Teston EF, Nass EMA, Costa JR,
et al. Ganho de peso gestacional excessivo no Sistema Único de Saúde. Acta Paul Enferm. 2021 Nov; 34: eAPE001105.
18. Horta BL, Barros FC, Lima NP, Assunção MCF, Santos IS, Domingues MR,
et al. Maternal anthropometry: trends and inequalities in four population-based birth cohorts in Pelotas, Brazil, 1982-2015. Int J Epidemiol. 2019 Apr; 48 (Suppl. 1): i26–36.
19. McDowell M, Cain MA, Brumley J. Excessive Gestational Weight Gain. J Midwifery Womens Health. 2019 Jan; 64 (1): 46-54.
20. Ferreira LAP, Piccinato CA, Cordioli E, Zlotnik E. Pregestational body mass index, weight gain during pregnancy and perinatal outcome: a retrospective descriptive study. Einstein (São Paulo). 2019 Oct 28; 18.
21. Sun Y, Shen Z, Zhan Y, Wang Y, Ma S, Zhang S,
et al. Effects of pre-pregnancy body mass index and gestational weight gain on maternal and infant complications. BMC Pregnancy Childbirth. 2020; 20 (1): 390.
22. Santos SFM, Costa ACC, Araújo RGPS, Silva LAT, Gama SGN, Fonseca VM. Fatores associados à adequação do ganho de peso gestacional de adolescentes brasileiras. Ciênc Saúde Colet. 2022; 27 (7): 2629-42.
23. Poton WL, Santos AS, Bubach S, Cypreste AMZ, Oliveira CG, Oliveira AC,
et al. Aspectos metodológicos do Projeto VIVER: um estudo longitudinal no Espírito Santo (Brasil). Cad Saúde Colet. 2024.
(No prelo).
24. WHO Expert Committee on Physical Status: the Use and Interpretation of Anthropometry. Physical status: the use of and interpretation of anthropometry, report of a WHO expert committee. [
Internet] Geneva: WHO; 1995. [access in 2019 Nov 24]. Available from:
https://apps.who.int/iris/handle/10665/3700325. Rasmussen KM, Yaktine AL, Institute of Medicine (US) and National Research Council (US) Committee to Reexamine IOM Pregnancy Weight Guidelines, eds.
Weight Gain During Pregnancy: Reexamining the Guidelines. Washington (DC): National Academies Press (US); 2009. [access in 2019 Nov 24]. Available from:
https://pubmed.ncbi.nlm.nih.gov/20669500/26. Rodrigues PL, Lacerda EMA, Schlüssel MM, Spyrides MHC, Kac G. Determinants of weight gain in pregnant women attending a public prenatal care facility in Rio de Janeiro, Brazil: a prospective study, 2005-2007. Cad Saúde Pública. 2008; 24: s272-84.
27. Aghaee S, Laurent CA, Deardorff J, Ferrara A, Greenspan LC, Quesenberry CP,
et al. Associations of Maternal Gestational Weight Gain and Obesity With the Timing of Pubertal Onset in Daughters. Am J Epidemiol. 2019 Mar; 188 (7): 1262-9.
28. Nguyen NTK, Fan H-Y, Tsai M-C, Tung T-H, Huynh QTV, Huang S-Y,
et al. Nutrient Intake through Childhood and Early Menarche Onset in Girls: Systematic Review and Meta-Analysis. Nutrients. 2020 Sep; 12 (9): 2544.
29. Nieuwenhuis D, Pujol‐Gualdo N, Arnoldussen IAC, Kiliaan AJ. Adipokines: A gear shift in puberty. Obes Rev. 2020 Jan 30; 21 (6).
30. Must A. Recall of Early Menstrual History and Menarcheal Body Size: After 30 Years, How Well Do Women Remember? Am J Epidemiol. 2002 Apr; 155 (7): 672-9.
Authors’ contributionPoton WL, Bubach S and Santos AS: conception, study design and analysis of the manuscript. Cassiano DR and Bubach S: interpretation of the results, writing and critical review of the manuscript’s content. All the authors have approved the final version of the manuscript and declare no conflicts of interest.
Received on March 21, 2023
Final version presented on August 19, 2024
Approved on August 26, 2024
Associated Editor: Aurélio Costa


 ; Susana Bubach 2
; Susana Bubach 2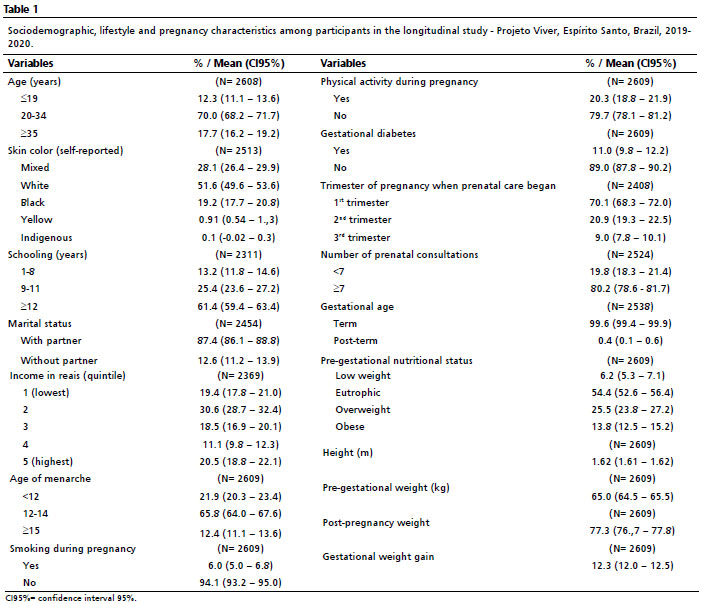






 Ler em português
Ler em português