ABSTRACT
OBJECTIVES: to determine the association between vertical childbirth posture and grade II or higher perineal tears in women attended under a humanized model.
METHODS: 715 clinical records of humanized deliveries attended between 2016 and 2022 in Viña del Mar, Chile, were studied using bivariate analysis and binary logistic regression.
RESULTS: 64.1% of the women presented perineal lesions, mainly low grade (51.2%). Second degree tears or more represented 12.2% (mostly grade II), with very few grade III tears (0.7%) and zero grade IV tears. Vertical postures, compared to horizontal ones, were significantly associated with the presence of grade II tears or more (p=0.02), even after adjusting for maternal and neonatal variables (OR=2.31, CI95%=1.11-4.81). Of the latter, parity and size of the newborn were the factors most associated with this type of injury.
CONCLUSION: humanized childbirths in general present less frequency and severity of perineal injuries than what is reported in traditional care; however, upright postures, compared to horizontal ones, were significantly associated with the presence of grade II or higher tears.
Keywords:
Humanizing delivery, Home childbirth, Posture, Pelvic floor
RESUMO
OBJETIVOS: determinar la asociación entre postura de parto vertical y desgarros perineales grado II o más en mujeres atendidas bajo el modelo humanizado.
MÉTODOS: se estudiaron 715 registros clínicos de partos humanizados atendidos entre 2016 y 2022 en Viña del Mar, Chile, mediante análisis bivariado y regresión logística binaria.
RESULTADOS: el 64.1% de las mujeres presentó lesiones perineales, principalmente de bajo grado (51.2%). Los desgarros de segundo grado o más representaron un 12.2% (mayoritariamente grado II), siendo muy escasos los desgarros grado III (0.7%) y nulos los desgarros grado IV. Las posturas verticales, en comparación a las horizontales, se asociaron significativamente a la presencia de desgarros grado II o más (p=0.02), incluso luego de ajustar por variables maternas y neonatales (OR=2.31, IC95%=1.11-4.81). De estas últimas, la paridad y la talla del recién nacido fueron los factores que más se asociaron con este tipo de lesiones.
CONCLUSIÓN: los partos humanizados en general presentan una menor frecuencia y gravedad de lesiones perineales que lo reportado en atenciones tradicionales, no obstante, las posturas verticales, en comparación a las horizontales, se asociaron significativamente a la presencia de desgarros grado II o más.
Palavras-chave:
Parto humanizado, Parto domiciliario, Postura, Piso pélvico
IntroductionComparing to the rest of Latin American and Caribbean countries, Chile has low maternal and infant mortality rates.
1-3 However, maternal morbidity associated with childbirth care is high, with 91% of induced deliveries, 55% with continuous fetal monitoring, 56% with episiotomies and 80% assisted in lithotomy position.
4 In addition, a study conducted in 2018,
5 indicated that women felt poorly informed and listened to, and, even, mistreated during care. For this reason, the World Health Organization (WHO) has guidelines in favor of humanized childbirth, for example, accompanied, respectful and informed childbirths, which favor the spontaneity of the process for greater maternal-fetal well-being.
6,7During the last decade, the number of births attended at a Chilean private health sector increased from 21% to 32%,
2 which could be related to the increase in home births. If in 2003 there were 20 assistances per year, in 2017 there were more than 30 per month, with low rates of maternal or neonatal complications (2%), episiotomies (2.3%) and perineal tears (32.2%), which, for the most part, were mild or first degree (99.4%).
8Numerous factors influence the development of perineal injuries during labor, including stressed urinary incontinence, home delivery, forceps use, prolonged expulsive period of labor, type of pushing, routine episiotomy, family history of pelvic floor dysfunction, induction of labor, vacuum extraction and fetal head circumference equal to or greater than 35cm.
9-11 Therefore, childbirth in the correct position benefits the mother and the newborn,
12-14 with fewer interventions and postpartum care.
15,16Upright, or flexible sacral posture during the second stage of labor enhances uterine labor by gravity and pelvic expansion,
15 decreasing compression of the maternal aorta.
16,17 Among the benefits following an upright delivery, shorter length of labor and reduced rates of episiotomy and assisted delivery have been reported. However, when compared to horizontal postures, there is a greater risk of stage II tears and blood loss of more than 500 ml.
2,8,11,18 Despite this, studies with Chilean women have shown that these injuries are less frequent in humanized childbirths than in traditional care.
2Humanized childbirth care is a growing trend, due to its benefits in labor and the reduction of maternal and neonatal risks.
2,6,7 However, the vertical posture, frequent in this type of care, could favor pelvic floor muscle injuries,
15 although the evidence is contradictory.
2,8 Therefore, the objective of this study was to determine the association between the type of posture adopted during labor and the occurrence of stage II or higher perineal injuries in humanized care.
MethodsAnalytical cross-sectional study that included the records of all humanized childbirth care at the OBSNATURA Center in Viña del Mar, Chile, between January 2016 and March 2022 (789 childbirths). OBSNATURA is a health center created by midwives, which was created to provide prenatal education and currently focuses on humanized and multidisciplinary care of natural childbirth, in water, at home and in private health institutions. Term deliveries (37 weeks or more) were included, excluding those in which episiotomy was performed (19 childbirths) and records with incomplete data (55 childbirths). Consequently, 715 deliveries were analyzed.
The response variable was second-degree tears or more during the second stage of labor. A binary indicator was constructed, assigning the value “1” in the case of grade II, III or IV tears, and “0” otherwise (grade I or lesser tears, such as mucosal or labial fissures, haematomas, including undamaged perineum).
To measure childbirth posture, defined as the position chosen by the patient during the second stage of labor (expulsive),
13 a two-level categorical variable was created: (a) vertical or flexible sacral posture, including sedentary positions (in labor chair, on stretcher, on the bed, on the toilet, in a car, in a tub with water), fowler position, standing, leaning or hanging from the neck, kneeling, and four-lying or squatting (on a stretcher, a bed, the floor or in water); b) horizontal or reduced sacral mobility postures, including lithotomy, Mc Robert, supine in bed, lying in bed (stretcher or floor), and right or left lateral decubitus (lateral SIMS).
To reduce possible confounding biases, maternal and newborn variables were included for control or adjustment, including: duration of the second stage of labor (in minutes); use of neuroaxial anesthesia during labor and childbirth; type of delivery (spontaneous or pharmacologically intervened); the newborn’s weight (in grams), head circumference (in centimeters) and height (in centimeters); mother’s age (in years), number of previous children and occupation (student, technician, professional or housewife).
Descriptive statistics included measures for categorical variables (percentages) and numerical variables (mean and standard deviation). Bivariate association was performed using Pearson’s chi-square and Student’s t-test. Finally, multivariate analysis was performed by binary logistic regression, reporting crude and adjusted odds ratios (OR) with 95% confidence intervals. All analyses were performed at a significance level of 5% (
p<0.05), using STATA 16.0 statistical software.
The research protocol was approved by the Scientific Ethical Committee of the
Universidad Mayor de Santiago de Chile (approval act 0253 on May 11, 2022), which granted a waiver of informed consent for the use of clinical records.
ResultsPerineal injuries were present in 64.1% of the women who received humanized childbirth care; however, most of them corresponded to grade I tears (51.2%). Grade II or greater tears accounted for 12.2%, being mainly type II. The frequency of major tears was very low, with only 0.7% of grade III tears, with no findings of grade IV tears.
The participants’ average age was 31±4.8 years, most of whom were professionals or technicians. Humanized care was mainly performed in private clinics. Table 1 presents the general description of the study population together with the bivariate analysis between the sociodemographic and clinical variables of the participants and the presence of perineal tear grade II or higher.
Seventy-nine.9% (571) of the deliveries were attended in upright postures. When associating to childbirth posture with the presence of pelviperineal muscle injury, there were significant statistical differences (
p=0.02) between the proportion of grade II or greater tears in women attended in upright positions (13.7%), in comparison to the horizontal postures (8.5%).
No significant differences were observed between the frequencies of perineal tears type II or more according to the mother’s age, occupation or place of delivery (private institution or home). However, all maternal clinical variables were significantly associated with this type of perineal injuries, among them, number of children and parity (
p<0.01), expulsion time (
p=0.02), use of neuroaxial anesthesia (
p=0.02) and type of delivery (
p=0.02). In relation to the clinical variables of the newborn, significant differences were only present the height in centimeters (
p=0.05).
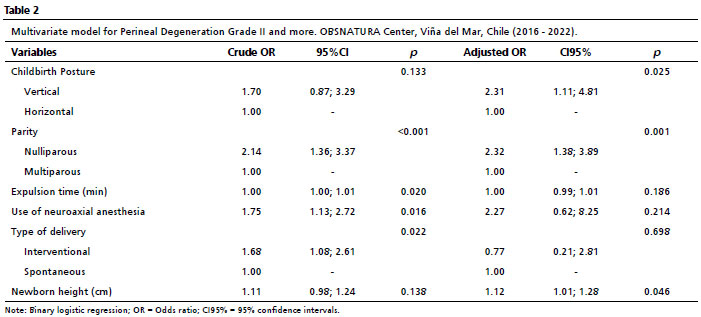
From the significant findings of the bivariate analysis, a multivariate analysis was performed by binary logistic regression (Table 2) reporting crude and adjusted odds ratios (OR) and 95% confidence intervals. Vertical postures during the second stage of labor, compared to horizontal postures, after adjusting for maternal and newborn variables, were significantly associated with the presence of perineal tears type II or more, increasing the probability of occurrence of this type of injury (OR=2.31, CI95%=1.11-4.81). In regards to the adjustment variables, nulliparous women had a higher chance of suffering this type of injury compared to women who had at least one child before the present delivery (OR=2.32, CI95%=1.38-3.89). In turn, for each additional centimeter of height of the newborn, the probability of occurrence of this type of tears increased 2% (OR=1.12, CI95%=1.01-1.28).
DiscussionThe findings of the present study show that vertical posture during the second stage of labor in humanized care, compared to horizontal posture, is significantly associated with the presence of grade II or more tears; however, these injuries have a lower frequency and severity than those reported in deliveries attended under the traditional model.
The overall frequency of perineal injuries was considerably low, being mainly grade I injuries. Muscle injuries (grade II or III tears) represented only 12.9%, with no cases of grade IV tears (rupture of the anal sphincter muscles with tearing of the anal mucosa). Regarding to parity, primiparas presented a higher frequency of injuries (8.6%) than multiparas (4.4%), which is in line with the higher risk reported in that group.
19 Consequently, when comparing our results, we can observe that humanized delivery had a lower prevalence and severity of perineal injuries, which coincides with a decreasing trend reported by recent scientific literature.
20,21A study
22 conducted in a maternity hospital in Brazil reported the frequency of perineal injuries in spontaneous vaginal deliveries without episiotomy. The prevalence of grade I tears was 47%, grade II lesions reached 31% and third degree lesions only 1.8%, with no type IV tears. Although the order of the frequencies coincides with the findings of the present study, the magnitude observed in the humanized deliveries analyzed was considerably lower, mainly in grade II and III tears with 12.2% and 0.7%, respectively. Therefore, it can be pointed out that the frequency of tears occurring in humanized deliveries, compared to spontaneous vaginal deliveries attended under the traditional model, is lower and distributed more towards less severe injuries.
Binfa
et al.
4 studied the frequency of grade III tears in humanized childbirth in Chile, and found a prevalence of 0.7%. In the present study, the frequency of this type of tearing coincided exactly with what was reported. It should be noted that, both in that study and in the present one, no serious injuries (grade IV tears) were recorded, which is a very relevant fact to ratify the importance of humanized care for the prevention of serious pelvic floor dysfunctions in the postpartum period, such as persistent pain,
23 postpartum depression,
24 fecal incontinence,
25 among others.
26The available evidence on the relation between birth posture and perineal indemnity is inconclusive. Steen
et al.,
27 note that lateral (horizontal) position increases rates of intact perineum and that upright, four-lying (not squatting) position reduces the risk of perineal trauma. De Jonge
et al.
28 on the other hand, describe that grade II perineal tears increase when in a sitting position is adopted, comparing to a reclining position, a finding that coincides with our study where the highest frequency of perineal injuries occurred in upright postures, without breaking down in details whether the upright posture is sitting, upright, kneeling or squatting. Markus
et al.
29 reinforce the above, indicating that maternal childbirth positions with reduced sacral flexibility significantly decrease the risk of second-degree perineal tearing. These findings coincide with the results obtained in this study, where the risk of type II or greater muscle tearing was significantly higher in women in the vertical delivery position than in those in horizontal positions, after adjusting for maternal and newborn variables.
Regarding adjustment variables, the use of neuroaxial anesthesia was not associated with the presence of grade II or greater perineal tears (OR=2.29, CI95%=0.64-8.14), which is not consistent with other primary and secondary research that has reported that the use of anesthesia is more of a protective factor that tends to decrease perineal tears.
13,25Meanwhile, maternal age was not a determining factor for the presence of postpartum perineal dysfunction, which is inconsistent with evidence supporting this direct association.
25,29 Nulliparity was significantly associated with the presence of type II or more perineal tears, which is consistent with other researches.
22,29,30 In our investigation, newborn weight was not associated with the presence of type II or greater tears; however, height showed positive association, which partially coincides with evidence reporting this type of lesions when newborn weight exceeds 4,000 grams.
25,29,31 Although a variable called macrosomia was included in the analysis, there were no significant results to report.
One of the limitations of this study is that the data on perineal injuries correspond to clinical reports, so future research is recommended with other quantitative measurements to objectively compare tissue discontinuity, for example, imaging technologies such as ultrasound.
31 Another limitation is that we do not report the frequency of tearing for each subvariety of, vertical or horizontal posture, so we suggest determining this type of injury separately, especially in squatting position, which has been attributed to a higher risk of pelvic floor injury relative to other standing postures.
27Perineal tears could be related to the presence of symptoms of pelviperineal dysfunctions, so we recommend developing longitudinal studies that evaluate the state of pelvic floor functionality in postpartum humanized care and the factors that could influence the occurrence of dysfunctions.
The strengths of this study in contributing to the knowledge on humanized childbirth care, providing valuable information regarding the effect of the postures on the pelvic floor adopted in this type of delivery. On the other hand, the size of the database used, with a large number of clinical records, makes the present investigation one of the largest Chilean studies on humanized multidisciplinary care of natural childbirth.
In conclusion, the findings of the present study show that women in labor attended under the humanized model have a lower frequency and severity of perineal tears compared to those reported at childbirth attended under the traditional model.Vertical positions during the second stage of labor, compared to horizontal positions, are significantly associated with the presence of grade II or higher tears, as are other factors, including nulliparity, length of labor, and size of the newborn.
References1. Centro Latinoamericano y Caribeño de Demografía (CELADE). América Latina y el Caribe: Estimaciones y proyecciones de población. División de Población de la Comisión Económica para América Latina y el Caribe (CEPAL). 2022. [access in 2023 Jan 15]. Available from:
https://www.cepal.org/es/subtemas/proyecciones-demograficas/america-latina-caribe-estimaciones-proyecciones-poblacion2. Ministerio de Salud de Chile. Departamento de Estadísticas e Información en Salud (DEIS). Indicadores Básicos de Salud de Chile 2016. 2018. [access in 2023 Jan 15]. Available from:
http://www.deis.cl/wp-content/uploads/2018/12/IBS-2016.pdf3. Sadler M, Leiva G. Nacer en el Chile del Siglo XXI: el sistema de salud como un determinante social crítico en la atención del nacimiento. In: Cabieses B, Bernales M, Obach A, et al. (eds) Vulnerabilidad social y su efecto en salud en Chile. Universidad del Desarrollo, Santiago; 2016. p. 61-77.
4. Binfa L, Pantoja L, Ortiz J, Gurovich M, Cavada G, Foster J. Assessment of the implementation of the model of integrated and humanised midwifery health services in Chile. Midwifery. 2016; 35: 53-61.
5. Observatorio de Violencia Obstétrica de Chile (OVO Chile). Resultados Primera Encuesta sobre el Nacimiento en Chile. Santiago; 2018.
6. World Health Organization (WHO). WHO recommendations on intrapartum care for a positive childbirth experience. Geneva: WHO; 2018. [access in 2023 Jan 15]. Available from:
https://www.who.int/publications/i/item/97892415502157. Masoumi SZ, Kazemi F, Oshvandi K, Jalali M, Esmaeili-Vardanjani A, Rafiei H. Effect of training preparation for childbirth on fear of normal vaginal delivery and choosing the type of delivery among pregnant women in Hamadan, Iran: A randomized controlled trial. J Family Reprod Health. 2016; 10 (3): 115-21.
8. Reischmann P, Risi C, Serrano N. Evaluación de la atención del parto en casa planificado con asistencia profesional, durante los años 2003–2014. Seminario para optar al grado de Licenciado en Obstetricia y Puericultura. Universidad de Santiago de Chile; 2015.
9. Barasinski C, Vendittelli F. Effect of the type of maternal pushing during the second stage of labour on obstetric and neonatal outcome: a multicentre randomised trial-the EOLE study protocol. BMJ Open. 2016; 6 (12): e012290.
10. Jiang H, Qian X, Carroli G, Garner P. Selective versus routine use of episiotomy for vaginal birth. Cochrane Database Syst Rev 2017 Feb; 2 (2): CD000081.
11. Jansson MH, Franzén K, Hiyoshi A, Tegerstedt G, Dahlgren H, Nilsson K. Risk factors for perineal and vaginal tears in primiparous women – the prospective POPRACT-cohort study. BMC Pregnancy Childbirth 2020; 20 (1): 749.
12. Mao Y-J, Zheng Z-J, Xu J-H, Xu J, Zhang X-L. Pelvic floor biometry in asymptomatic primiparous women compared with nulliparous women: a single-center study in Southern China. J Int Med Res. 2020 Apr; 48 (4): 030006052092039.
13. Masenga GG, Shayo BC, Msuya S, Rasch V. Urinary incontinence and its relation to delivery circumstances: A population-based study from rural Kilimanjaro, Tanzania. PLoS One. 2019 Jan; 14 (1): e0208733.
14. Gizzo S, Di Gangi S, Noventa M, Bacile V, Zambon A, Nardelli GB. Women’s choice of positions during labour: return to the past or a modern way to give birth? A cohort study in Italy. Biomed Res Int. 2014; 2014: 638093.
15. Berta M, Lindgren H, Christensson K, Mekonnen S, Adefris M. Effect of maternal birth positions on duration of second stage of labor: systematic review and meta-analysis. BMC Pregnancy Childbirth. 2019; 19 (1): 466.
16. Lawrence A, Lewis L, Hofmeyr GJ, Styles C. Maternal positions and mobility during first stage labour. En: Lawrence A, editor. Cochrane Database of Systematic Reviews. Chichester, UK: John Wiley & Sons, Ltd; 2013.
17. Satone PD, Tayade SA. Alternative birthing positions compared to the conventional position in the second stage of labor: a review. Cureus. 2023 Apr; 15 (4): e37943.
18. Gupta JK, Sood A, Hofmeyr GJ, Vogel JP. Position in the second stage of labour for women without epidural anaesthesia. Cochrane Libr. 2017; 2017 (5).
19. Kim KW, Lee S. Childbirth outcomes and perineal damage in women with natural childbirth in Korea: a retrospective chart review. Korean J Women Health Nurs. 2021 Dec; 27 (4): 379-87. [Korean].
20. Tavakoli A, Panchal VR, Mazza GR, Mandelbaum RS, Ouzounian JG, Matsuo K. The association of maternal obesity and obstetric anal sphincter injuries at time of vaginal delivery. AJOG Glob Rep. 2023 Oct; 3 (4): 100272.
21. Laurita Longo V, Odjidja EN, Zanfini BA, Catarci S, Carducci B, Draisci G, et al. Risk factors associated with severe perineal lacerations during vaginal delivery: a 10-year propensity score-matched observational study. AJOG Glob Rep. 2023 Mar; 3 (2): 100174.
22. Lins VML, Katz L, Vasconcelos FBL, Coutinho I, Amorim MM. Factors associated with spontaneous perineal lacerations in deliveries without episiotomy in a university maternity hospital in the city of Recife, Brazil: a cohort study. J Matern Fetal Neonatal Med. 2019; 32 (18): 3062-7.
23. Komatsu R, Ando K, Flood P. Factors associated with persistent pain after childbirth: a narrative review. Brit J Anaesth. 2020 Mar; 124 (3): e117-30.
24. Mohammad Redzuan SA, Suntharalingam P, Palaniyappan T, Ganasan V, Megat Abu Bakar PN, Kaur P, et al. Prevalence and risk factors of postpartum depression, general depressive symptoms, anxiety and stress (PODSAS) among mothers during their 4-week postnatal follow-up in five public health clinics in Perak: A study protocol for a cross-sectional study. BMJ Open. 2020; 10 (6): e034458.
25. Thubert T, Cardaillac C, Fritel X, Winer N, Dochez V. Définitions, épidémiologie et facteurs de risque des lésions périnéales du 3e et 4e degrés. RPC Prévention et protection périnéale en obstétrique CNGOF. Gynecol Obstet Fertil Senol. 2018; 46 (12): 913-21.
26. Ferreira CWS, Atan IK, Martin A, Shek KL, Dietz HP. Pelvic organ support several years after a first birth. Int Urogynecol J. 2017; 28 (10): 1499-505.
27. Steen M, Diaz M. Perineal trauma: a women´s health and wellbeing issue. Br J Midwifery. 2018; 26 (9): 574-84.
28. De Jonge A, Rijnders M, Van Diem M, Scheepers PLH, Lagro Janssen ALM. Birthing positions during second stage of labor and long-term psychological outcomes in low-risk women. Int J Childbirth. 2011; 1 (4): 242-53.
29. Aasheim V, Nilsen ABV, Reinar LM, Lukasse M. Perineal techniques during the second stage of labour for reducing perineal trauma. Cochrane Libr. 2017; 2018 (6).
30. Wilson AN, Homer CSE. Third- and fourth-degree tears: A review of the current evidence for prevention and management. Aust N Z J Obstet Gynaecol. 2020 Apr; 60 (2): 175-82.
31. Cassadó J, Simó M, Rodríguez N, Porta O, Huguet E, Mora I, et al. Prevalence of levator ani avulsion in a multicenter study (PAMELA study). Arch Gynecol Obstet. 2020; 302 (1): 273-80.
Authors’ contributionCavallari-Drey YE and Ortiz-Llorens M: formulation of the research idea, study design, data collection, and analysis and interpretation of the results. Drafting of the article. The authors have approved the final version of the article and declared they have no conflicts of interest.
Received on August 2, 2023
Final version presented on June 16, 2024
Approved on July 1, 2024
Associated Editor: Melânia Amorim


 ; Manuel Ortiz-Llorens 2
; Manuel Ortiz-Llorens 2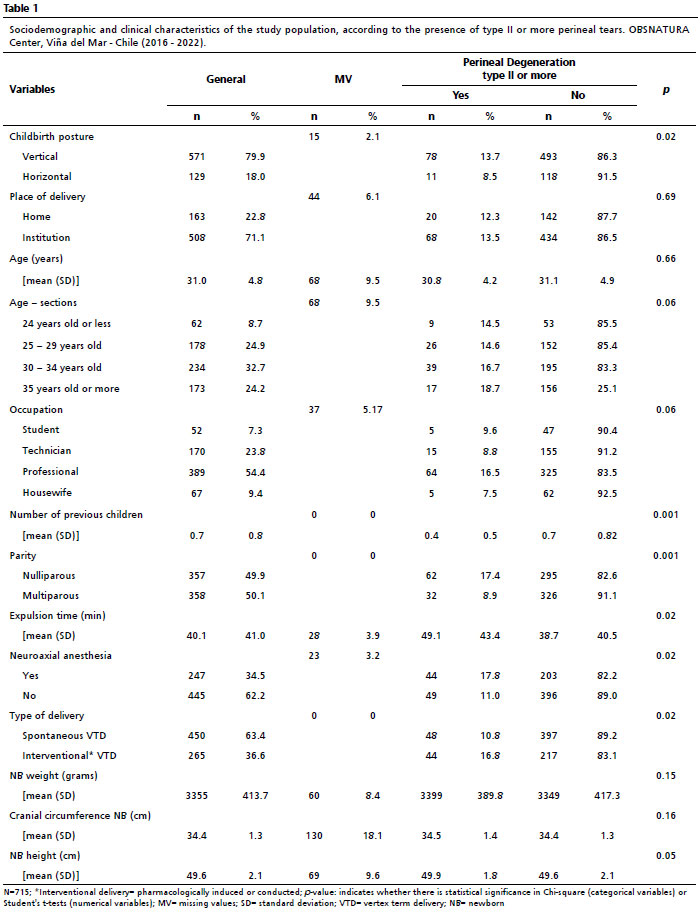






 Ler em português
Ler em português