ABSTRACT
OBJECTIVES: to analyze the choice and continuation rate of contraceptive methods in women with sickle cell disease (SCD).
METHODS: an exploratory prospective study was conducted at a hospital enrolling 44 women with SCD aged 15-40 years old. After contraceptive counseling, the women selected one of the available contraceptive methods and separated into two groups, and were followed up at one, three, six, and 12 months. To analyze the continuation rate of contraceptive use, the two groups were: group (G1) using progestin-only contraceptives, through any route of administration and group (G2) using other contraceptive methods (combined hormonal and non-hormonal contraceptives). The continuation rate was analyzed using Kaplan-Meier survival analysis, considering a p<0.05.
RESULTS: after contraceptive counseling, most women opted for any progestin-only methods: injectable contraceptives (n=18; 40.9%), oral contraceptives (n=7; 15.9%), or intrauterine devices (n=3; 6.8%). The continuation rate decreased in both groups during the 12-months follow-up period. In the G1, the continuation rate was 60.7% (CI95%=40.4-76.0), while that in the G2 was 68.7% (CI95%= 40.5-85.6) with no significant difference between the groups (p=0.641).
CONCLUSIONS: the overall continuation rates in both groups were satisfactory. No significant difference in the continuation rate of contraceptive methods was observed between the groups, although most women preferred progestin-only methods.
Keywords:
Sickle cell disease, Anemia sickle cell, Contraception, Patient compliance, Medication adherence
RESUMO
OBJETIVOS: analisar a escolha e a taxa de continuação do uso de métodos contraceptivos em mulheres com doença falciforme (DF).
MÉTODOS: foi realizado um estudo prospectivo exploratório em um hospital, no qual foram incluídas 44 mulheres com DF com idade entre 15 e 40 anos. Após aconselhamento contraceptivo, as mulheres selecionaram um dos métodos contraceptivos disponíveis e foram separadas em dois grupos, sendo acompanhadas por um, três, seis e 12 meses. Para analisar a taxa de continuação do uso de métodos contraceptivos, os dois grupos foram: grupo (G1) que utilizou apenas contraceptivos de progestágeno, por qualquer via de administração e grupo (G2) que utilizou outros métodos contraceptivos (contraceptivos hormonais combinados e não hormonais). A taxa de continuação foi analisada pela análise de sobrevida de Kaplan-Meier, considerando um p<0,05.
RESULTADOS: após aconselhamento contraceptivo, a maioria das mulheres optou por algum dos métodos contendo apenas progestágeno: contraceptivos injetáveis (n=18; 40,9%), contraceptivos orais (n=7; 15,9%) ou dispositivos intrauterinos (n=3; 6,8%). A taxa de continuação diminuiu em ambos os grupos durante o período de acompanhamento de 12 meses. No G1, a taxa de continuação foi de 60,7% (IC95%= 40,4-76,0), enquanto no G2 foi de 68,7% (IC95%= 40,5-85,6) sem diferença significativa entre os grupos (p=0,641).
CONCLUSÕES: as taxas gerais de continuação em ambos os grupos foram satisfatórias. Não foi observada diferença significativa na taxa de continuação dos métodos contraceptivos entre os grupos, embora a maioria das mulheres tenha preferido métodos somente com progestágeno.
Palavras-chave:
Doença falciforme, Anemia falciforme, Contracepção, Adesão do paciente, Adesão à medicação
IntroductionSickle cell disease (SCD) is a common genetic and inherited disease affecting hemoglobin development.
1 In Brazil with heterogeneous ethnicity and population distribution, it is estimated that approximately 60,000 to 100,000 people have SCD.
2 Hemolysis and chronic inflammation are responsible for pain and multisystemic involvement.
1,2 Over the past decades, thanks to improved screening and advances in complication and disease control management, reproductive-age women with SCD are beginning to face fertility control and pregnancy challenges.
3,4 Pregnant women with SCD have a higher frequency of unfavorable maternal and fetal outcomes, including pain crisis, miscarriages, stillbirths, preterm deliveries, preeclampsia, and perinatal and maternal mortalities.
5,6Effective contraception is a complex task and involves many steps beyond simply providing education and counseling, and there may still be many barriers in preventing unwanted pregnancy and its consequences.
7 However, counseling on effective contraception is considered an important strategy to reduce unplanned pregnancies. Once women are informed of the risks and benefits of different contraceptive methods, they can plan when and how many children they would like to have.
8-11 In addition to promoting universal access to reproductive planning in women with SCD, adequate clinical follow-up, correct method of contraceptive use, and continuation rates should be monitored.
10-12Many factors may influence the continued use of contraceptive methods, including sociocultural characteristics, forms of administration, patient or provider’s motivation, provider’s beliefs, clinical condition, disease severity, patient’s perception of the benefit of medication use, and access to health services.
11,13-15The use of progestin-only contraceptives has increased over the past decade among women with SCD because of their positive health benefits, and they are classified as CDC (Centers for Disease Control) and World Health Organization (WHO) category 1 (no restrictions on their use).
16,17 However, women with SCD lack knowledge of contraceptive efficacy and make limited use of reversible contraception when compared to the general population.
15,18 Since contraceptive preferences and continuation rates may vary due to many factors, it is important to investigate whether women with SCD may be more likely to select a progestin-only contraceptive methods and consequently use it for longer period compared to other methods; this study aimed to analyze the choice and continuation use rate of contraceptive methods in such women.
MethodsThis exploratory observational study was conducted at a reference hospital for women’s healthcare in Recife, Pernambuco, Brazil, from January 2018 to August 2020.
The study sample had 44 women with SCD aged 15-40 years old, with a sexually active lifestyle and a desire for contraception. We excluded women who were not using contraceptive methods due to the desire of getting pregnant.
The women participating in the study were recruited in the waiting room of the outpatient gynecologic clinic while waiting for the service; those who agreed to participate were interviewed for the collection of socio-demographic, clinical, and reproductive data. They received contraceptive counseling and then they selected one of the contraceptive methods available at the service: combined oral contraceptive, combined injectable, progestin-only pill, progestin-only injectable, copper intrauterine device, levonorgestrel intrauterine device, female sterilization, and male condom. Contraceptive implants, hormonal patch, and vaginal ring were not included as an option for our patients because they were not available in the public health service.
Individualized contraceptive counseling was provided by two specialists (nurse and gynecologist) trained in reproductive planning. The counseling adhered to the WHO and CDC eligibility criteria.
15,16 Counseling included information on each available method, efficacy, mechanism of action, use, contraindications, and possible side effects. After the women selected their preferred contraceptive method, the instructions for use were reinforced with verification of the woman’s understanding. All the women received the selected method to begin on the first day of the next period or were instructed to return for intrauterine device (IUD) insertion, when this was the selected method.
The women were instructed to return to the clinic after one, three, six, and 12 months. At each follow-up, appropriate use, continuation rate, desire to change methods, clinical or gynecological complaints, and occurrence of pregnancy were assessed. Women who did not return were contacted by phone to reschedule the visit.
To analyze the continuation rate of contraceptive use, the women were divided into two groups: one group (G1) used progestin-only methods (progestin-only pill, progestin-only injectable or levonorgestrel intrauterine device) and another group (G2) used other contraceptive methods as combined hormonal and non-hormonal (combined oral contraceptive, combined monthly injectable, copper intrauterine device, female sterilization, and male condom). The self-reported continuation rate was considered, and at each return, the women were asked whether they were using the method as prescribed and did not stop using their selected contraceptives for ≥4 weeks.
Data analysis was performed using the STATA 12.1 software. The women’s data are presented in the tables. The continuation rate was analyzed using Kaplan–Meier survival analysis (long-rank test), considering a 95% confidence interval. Significance was set at
p<0.05.
The study was approved on October 25, 2017, by the Ethics Committee for Research Involving Human Beings where the study was carried out under the approval number 2.349.314 and CAAE number: 70666317.8.0000.5201.
ResultsOf the 54 women initially selected, ten were lost to follow-up, resulting in a sample of 44 women for the 12-months follow-up. It was not possible to know why the ten women did not return for follow-up. They did not respond to telephone calls (flowchart - Figure 1).
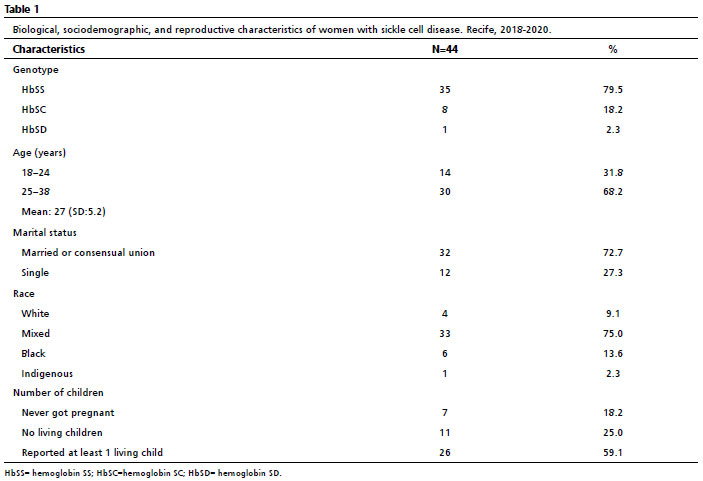
The genotype characteristics of the 44 study women were as follows: 35 women (79.5%) had HbSS (hemoglobin SS); 8 women (18.2%) had HbSC (hemoglobin SC) and only one woman (2.3%) had HbSD (hemoglobin SD). Their age ranged from 18 to 38 years old, with a mean age of 27 (SD: 5.2) years. Mixed race was predominant (n=33; 75%), and most were married or had a partner (n=32; 72.7%). Among the 37 women who had been pregnant, 11 (25%) had no living children. The most frequently reported clinical complication was pain crisis (n=18; 40.9%) (Table 1).
All 44 women (100%) reported having at least one episode of pain crisis, although 10 (22.7%) reported no pain crisis in the past 2 years. Six (13,6%) women reported a past thromboembolic event, while headache occurred in 34 women (77.3%)
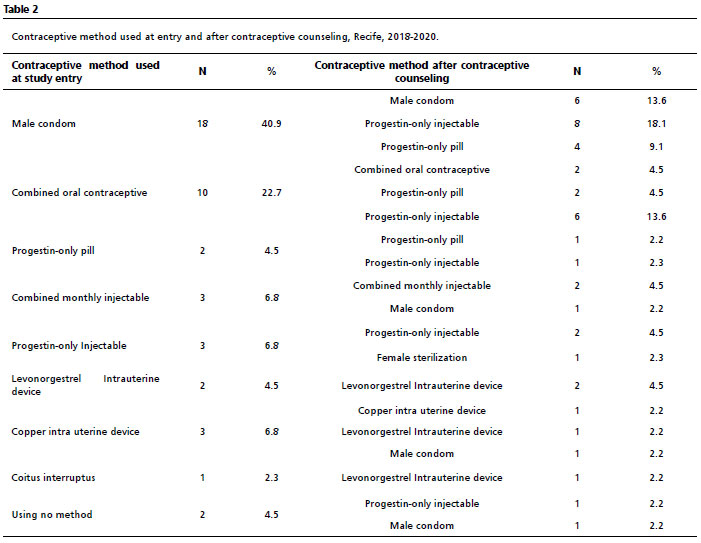
Among the contraceptive methods used prior to counseling, male condoms (n=18; 40.9%) and combined oral contraceptive (n=10; 22.7%) were predominant. After contraceptive counseling, the majority (63.6%) opted for progestin-only methods: Progestin-only injectable (n=18; 40.9%), progestin-only pill (n=7; 15.9%), or levonorgestrel intrauterine devices (n=3; 6.8%). The other choices were male condoms (n=9; 20.4%), combined oral contraceptive (n=4; 9.1%), copper IUDs (n=2, 4.5%), and one (2.3%) opted for female sterilization (Table 2).
During the study, five women discontinued the use of their selected method with the intention of getting pregnant; of these, two became pregnant during the study, resulting in a pregnancy rate of 4.5% (CI95%=0.6-15.5). The two women who became pregnant during the study had discontinued the use of the contraceptive method due to the desire of getting pregnant, and there were no reports of maternal or fetal complications in these two cases.
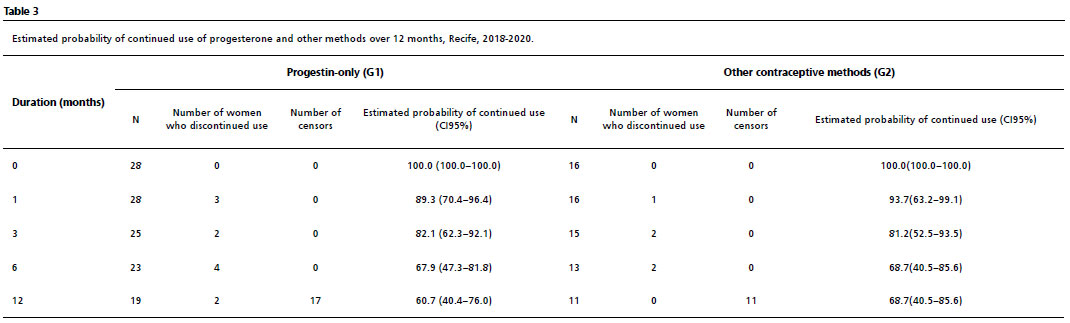
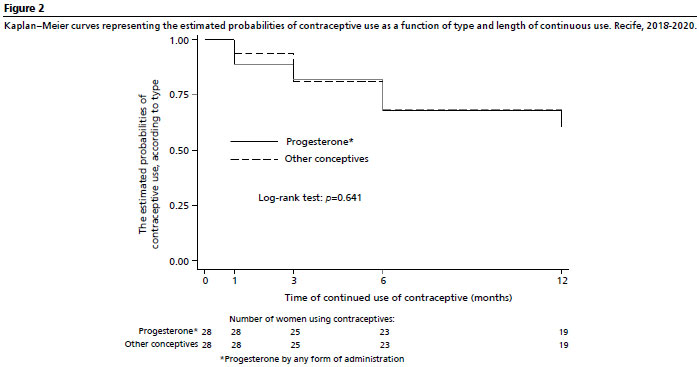
The continuation rate of contraceptive use decreased in both groups during the 12-months follow-up period. Among those using progestin-only methods, the continuation rate was 60.7% (CI95%=40.4-76.0), while among those using the other methods was 68.7% (CI95%=40.5-85.6) (Table 3), with no significant difference between the groups (
p=0.641; Figure 2).
DiscussionThere are few studies on contraception choice in women with SCD in Brazil and comparing the results of our study with a study conducted in São Paulo, Brazil and published in 2017, we observed that our results were comparable, in which >80% of women with SCD reported using contraception, with most of them using the combined hormonal contraceptive.
8 In our study, almost all women reported using some contraceptive method when entering the study, but almost 50% of them reported using an unreliable method such as condoms. On the other hand, after counseling most of them chose more reliable methods. The high women’s preference for progesterone-only methods may have been influenced by the counseling itself, which exposed the risks and benefits of each method. The health organizations
16,17 do not contraindicate any method for women with SCD, although some health conditions in addition to SCD may be limiting the choice. Some studies
10,13,14,19 have suggested health benefits for women with SCD using progestin-only methods, such as a decrease in the frequency of pain crises, although more studies are still needed to confirm this hypothesis. Nevertheless, among progesterone-only methods, levonorgestrel intrauterine devices have been recommended because they are considered a long-acting reversible contraception (LARC), do not depend on the woman’s memory and have less risk of contraceptive failure.
17,20Combined oral contraceptives, although culturally accepted by most of women in Brazil, and this was observed in a study in São Paulo among women with SCD
8, were not the first choice among women with SCD in our study. This could be a consequence of the hypothetical association of the combined hormonal contraceptive with an increased risk of venous thromboembolism in a group of women with a predisposing clinical condition.
15,21 No overlap of risks of combined hormonal contraceptive use with the pathophysiology of SCD has been documented in a well-designed study.
15,19,22Considering that women with SCD can use any contraceptive method if it is adequately monitored
7,17,23 and that SCD is a disease that can lead to unfavorable gestational outcomes for both the mother and the child,
5,6 we observed that the women in the present study understood the need to choose more effective methods and switched from less safe to safer methods. This reinforces the need to improve knowledge about contraceptive methods in women with SCD so that they can make more informed choices.
18,24 At the start of the study, before the counseling, almost half of the women had used male condoms as the only method. Male condoms also were the most common contraceptives used by Jamaican and American women diagnosed with SCD in previous studies.
25,26 The high rate of the barrier method may be due to fear or doubts in prescribing hormonal contraceptive methods to women with chronic conditions such as SCD.
27After counseling, progestin-only methods were the most selected ones. This change of methods may be related to the provision of personalized contraceptive counseling. The patient-centered counseling should also motivate the reproductive healthcare team to offer the best method to suit each patient’s needs while providing guidance on its correct use and possible adverse effects.
10,26 A study conducted in Uganda and Pakistan in women of childbearing age has revealed that high-quality family planning counseling, measured by information that contraceptive users received from providers, is associated with subsequent continuation of contraceptive use.
23 Regardless of the contraceptive method selected, studies on contraceptive use have demonstrated that women with SCD have low adherence.
13,18 Motivation and timing of reproductive life may interfere with both the choice and continuation of different methods.
25,27,28A Family Planning Survey carried out with young adults with SCD aged 18 to 30 years old, at a large academic hospital in Baltimore, United States, suggests an association of having an obstetrician/gynecologist care and contraception use.
11Reproductive health care often requires the physician to initiate the discussion, as patients may not voluntarily present their intimate healthcare concerns. Preferably, this discussion should begin from the beginning of reproductive life, even with the pediatrician, including the clinician, hematologist, and gynecologists.
11,15Moreover, method discontinuation may be related to the fear of side effects, the severity of the disease, lack of knowledge on fertility, and provider’s beliefs.
9,10,18,19,24The copper IUD
16,17 was selected by few women, although no current evidence towards limiting copper IUD use in women with SCD exists, except for women with anemia due to increased menstrual flow, in which case the risks and benefits of using the copper intrauterine device must be weighed.
16,17 Nevertheless, it has been reported as a safe option for most women of reproductive age with chronic conditions. Patients, also, may be fearful of the copper IUD because it is a foreign body placed in the uterus over a prolonged time,
10 or over estimate the chance of pregnancy associated with IUD use.
18The correct use of contraceptive methods is an important strategy to reduce the risk of unplanned pregnancy in women with SCD.
14 In this cohort, the pregnancy rate was low, even considering the small sample size, and it is important to highlight that those who got pregnant during the study stopped using contraceptives because they wanted the pregnancy.
Examining concerns related to pregnancy planning and contraceptive practices for women with SCD is worthwhile.
10 This was observed in a previous study in our service that highlighted the need for women with SCD to receive more attention in this counseling.
29In this sense, it is also possible to encourage women with SCD and others medical conditions to increase LARCs usage.
10,12,18 We cannot disregard the interference of the prescriber’s beliefs in the choice of contraceptive methods by women; however, this is difficult to measure.
29This study found a continuation rate of 60.7% for progestin-only methods in the first year of follow-up, and the progestin-only injectable being the most used among these. This was similar to the findings of a prospective cohort study that enrolled 5.087 women willing to start a new reversible contraceptive method in the United States and recorded an adherence rate of 57% to depot medroxyprogesterone acetate (DPMA), a progestin-only injectable, in the first year of use.
20The women in this present study were followed up for one year and although there was no difference in the continuation rate between the groups, the progestin-only methods were the most chosen, corroborating the literature recommendation that they are the most suitable for the group of women with SCD.
7,19,12,30Results from this study are limited due to the small sample size and was conducted at a single institution, although similar in size to other studies among SCD women.
11,26,27 Therefore, multicenter studies are needed, since SCD is not a very common condition.
We conclude that, the overall continuation rates of these methods were satisfactory. No significant difference in the continuation rate was observed when comparing the progestin-only methods group to the other contraceptive methods group, although women with SCD more often selected progestin-only methods.
This prospective research highlights the beneficial impact of contraceptive counseling in helping women with SCD to make an informed and effective contraceptive choice.
AcknowledgmentsWe would like to thank the Pernambuco Science and Technology Support Foundation (FACEPE) for the doctoral scholarship (Process number: IBPG-0860-4.01/16) granted to Evelyne Nascimento Pedrosa; the National Council for Scientific and Technological Development (CNPq) in Brazil for the productivity scholarship (Process number: 304094/2017-0) granted to Ariani Impieri Souza; and the support of the Coordination for the Improvement of Higher Education Personnel - Brazil (CAPES) through the Academic Excellence Program (PROEX).
References1. Steinberg MH. Sickle cell anemia, the first molecular disease: overview of molecular etiology, pathophysiology, and therapeutic approaches. Sci World J. 2008; 8: 1295-324.
2. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Secretaria de Ciência, Tecnologia e Insumos Estratégicos. Protocolo clínico e diretrizes terapêuticas da doença falciforme. [access in 2022 Nov 26]. Available from:
https://www.gov.br/saude/pt-br/assuntos/pcdt/arquivos/2018/doenca-falciforme-pcdt.pdf/view3. Lubeck D, Agodoa I, Bhakta N, Danese M, Pappu K, Howard R, et al. Estimated life expectancy and income of patients with sickle cell disease compared with those without sickle cell disease. JAMA Netw Open. 2019; 2 (11): e1915374.
4. Eissa AA, Tuck SM, Rantell K, Stott D. Trends in family planning and counselling for women with sickle cell disease in the UK over two decades. J Fam Plann Reprod Health Care. 2015; 41 (2):96-101.
5. Boafor TK, Olayemi E, Galadanci N, Hayfron-Benjamin C, Dei-Adomakoh Y, Segbefia C,
et al. Pregnancy outcomes in women with sickle-cell disease in low- and high-income countries: a systematic review and meta-analysis. BJOG. 2016; 123 (5): 691-8.
6. Silva FAC, Ferreira ALCG, Hazin-Costa MF, Dias MLG, Araújo AS, Souza AI. Adverse clinical and obstetric outcomes among pregnant women with different sickle cell disease genotypes. Int J Gynaecol Obstet. 2018; 143 (1): 89–93.
7. O’Brien SH, Klima J, Reed S, Chilsom D, Schwarz EB, Kelleher KJ. Hormonal contraception use and pregnancy in adolescents with sickle cell disease: analysis of Michigan Medicaid claims. Contraception. 2011; 83 (2): 134-7.
8. Carvalho NS, Braga JP, Barbieri M, Torloni MR, Figueiredo MS, Guazzelli CA. Contraceptive practices in women with sickle-cell disease. J Obstet Gynaecol. 2017; 37 (1): 74-7.
9. Moreira LR, Ewerling F, Barros AJD, Silveira MF. Reasons for nonuse of contraceptive methods by women with demand for contraception not satisfied: an assessment of low and middle-income countries using demographic and health surveys. Reprod Health. 2019; 16: 148.
10. Hunter-Greaves T, Medley-Singh N, Tate N, McDaniel A, Simms-Stewart D, Rattray C. Contraceptive practices in women with chronic medical conditions. J Obstet Gynaecol. 2021; 41 (4): 626-30.
11. Linton EA, Williams EC, Early ML, Prince E, Stewart RW, Lanzkron S,
et al. Family planning needs of young adults with sickle cell disease. EJHaem. 2023 Aug; 4 (3): 587-94.
12. Shankar D, Stanek CJ, Bangudi S, Liles SM, Colton ZA, Hart LC,
et al. Contraception, pregnancy, and STI counseling and care among transitioning young adults with sickle cell disease. [Letter]. Blood Adv. 2023; 7 (21): 6668-71.
13. De Sanctis V, Soliman AT, Daar S, Canatan D, Di Maio S, Kattamis C. Current issues and options for hormonal contraception in adolescents and young adult women with sickle cell disease: an update for health care professionals. Mediterr J Hematol Infect Dis. 2020; 12: e2020032.
14. Haddad LB, Curtis KM, Legardy-Williams JK, Cwiak C, Jamieson DJ. Contraception for individual with sickle cell disease: a systematic review of the literature. Contraception. 2012; 85 (6): 527-7.
15. Pecker LH, Kuo KHM. Go the Distance: Reproductive Health Care for People with Sickle Cell Disease. Hematol Oncol Clin North Am. 2022; 36 (6): 1255-70.
16. Nguyen AT, Curttis KM, Tepper NK, Kortsmit TK, Brittain AW, Snyder EM,
et al. U.S. Medical Eligibility Criteria for Contraceptive Use, 2024. MMWR Recomm Rep 2024 Aug; 73 (4): 1-126. [access in 2024 Aug 10]. Available from:
https://www.cdc.gov/mmwr/volumes/73/rr/rr7304a1.htm17. WHO (World Health Organization). Family Planning: A Global Handbook for Providers. Evidence-based guidance developed through worldwide collaboration. Updated 4
th edition 2022 [online]. [access in 2022 Dec 14]. Available from:
https://fphandbook.org/sites/default/files/WHO-JHU-FPHandbook-2022Ed-v221115a.pdf18. Pecker LH, Hussain S, Lanzkron S, Tao X, Thaler K, Burke AE,
et al. Women with sickle cell disease report low knowledge and use of long acting reversible contraception. J Natl Med Assoc. 2021; 113 (5): 552-9.
19. Bala NS, Stanek JR, Vesely SK, Cronin RM, Creary SE, Roe AH,
et al. Comparison of thromboembolism outcomes in patients with sickle cell disease prescribed hormonal contraception. Blood Adv. 2023; 7 (20): 6140-50.
20. Peipert JF, Zhao Q, Allsworth JE, Petrosky E, Madden T, Eisenberg D,
et al. Continuation and satisfaction of reversible contraception. Obstet Gynecol. 2011; 117 (5): 1105-13.
21. Franceschi LD, Cappellini MD, Olivieri O. Thrombosis and Sickle Cell Disease. Semin ThrombHemost. 2011; 37: 226-36.
22. Lizarralde-Iragorri MA, Shet S. Sickle Cell Disease: A Paradigm for Venous Thrombosis Pathophysiology. Int J Mol Sci. 2020; 21: 5279.
23. Chakraborty NM, Chang K, Bellows B, Grépin KA, Hameed W, Kalamar A,
et al. Association between the quality of contraceptive counseling and method continuation: findings from a prospective cohort study in Social Franchise Clinics in Pakistan And Uganda. Glob Health Sci Pract. 2019; 7 (1): 87-102.
24. Barden-O’Fallon J, Speizer IS, Calhoun LM, Corroon M. Women’s contraceptive discontinuation and switching behavior in urban Senegal, 2010-2015. BMC Women’s Health. 2018; 18: 35.
25. Knight-Madden J, Barton-Gooden A. Contraceptive usage among Jamaican women with sickle cell disease. Contraception. 2009; 80 (5): 474-8.
26. Roe AH, Lang B, McAllister A, Gaitors MC, Smith-Whitley K, Schreiber CA, et al. Contraceptive use and preferences among females with sickle cell disease. Contraception. 2022; 105: 42-5.
27. Khachikyan I, Speller-Brown B, Gomez-Lobo V, Trotman G, Darbari D. Reproductive health and knowledge among youth with sickle cell disease. J Nurse Pract. 2022; 18 (7): 726-9.
28. Pecker LH, Sharma D, Nero A, Paidas MJ, Ware RE, James AH, Smith-Whitley K. Knowledge gaps in reproductive and sexual health in girls and women with sickle cell disease. Br J Haematol. 2021; 194 (6): 970-9.
29. Pedrosa EN, Corrêa MSM, Ferreira, ALCG, Sousa CES, Silva RA, Souza AI. Contraception and reproductive planning from the perspective of women with sickle cell disease. Rev Gaúcha Enferm. 2021; 42: e20200109.
30. Baldwin MK, Bannow BS, Rosovsky RP, Nancy Sokkary N, Srivaths LV. Hormonal Therapies in females with blood disorders: thrombophilia, thrombosis, hemoglobinopathies, and anemias. Res Pract Thromb Haemost. 2023; 7 (4): e100161.
Authors’ contributionPedrosa EN: data design, collection and analysis, wrote the manuscript. Corrêa MSM: supervised the study. Silva FAC: design and data collection. Ferreira ALCG and Hazin-Costa MF: designed the study. Souza AI: designed and supervised the study, performed the data analysis and wrote the manuscript. All authors approved the final version of the article and have no conflicts of interest.
Received on June 12, 2023
Final version presented on August 3, 2024
Approved on August 6, 2024
Associated Editor: Leila Katz


 ; Maria Suely Medeiros Corrêa 2
; Maria Suely Medeiros Corrêa 2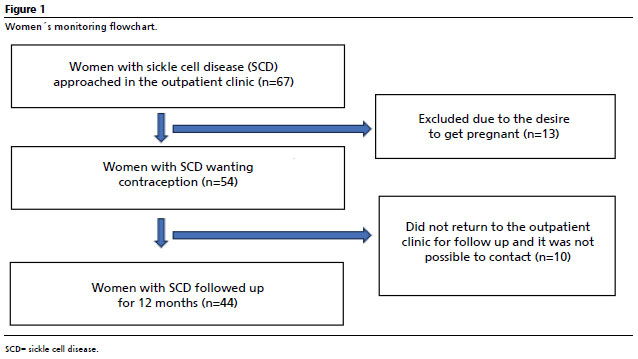






 Ler em português
Ler em português