ABSTRACT
INTRODUCTION: to report cases of women with acute kidney injury (AKI) in the pregnancy-puerperal cycle, admitted to a maternity teaching hospital in Recife, Pernambuco, Brazil.
DESCRIPTION: a case-series study reviewing the records of 100 patients with AKI admitted to the maternity hospital of the Institute of Integrative Medicine Professor Fernando Figueira (IMIP – Portuguese acronym).
DISCUSSION: the majority of patients (65.1%): were brown-skinned and the mean age was 25.5 years; were primiparas (65.1%) and had cesarean section (75.5%). The most common hypertensive disorder was preeclampsia (74.0%), followed by chronic arterial hypertension (11.0%) and eclampsia (6.0%). Hemorrhage occurred in 19% of women. The most common form of treatment was fluid therapy (70.0%) and oliguria was one of the most common AKI consequences (84.8%). Hemodialysis was necessary in 13% of cases and 4.0% died. Kidney function was restored prior to discharge from hospital in almost 70.0% of cases. The main causes of AKI were hypertensive disorders and hemorrhage/hemorrhagic shock.
Keywords:
Acute kidney injury, Pregnancy, Intensive care unit
RESUMO
INTRODUÇÃO: relato de casos de mulheres com lesão renal aguda (LRA) no ciclo grávido-puerperal internadas em uma maternidade escola do Recife-PE.
DESCRIÇÃO: realizou-se um estudo do tipo série de casos, por meio da análise dos prontuários de 100 pacientes que cursaram com LRA na maternidade do Instituto de Medicina Integral Prof. Fernando Figueira (IMIP).
DISCUSSÃO: a maioria das pacientes era parda (65,1%) e a idade média foi 25,5 anos, primíparas (65,1%) e tinham sido submetidas à cesariana (75,5%). O distúrbio hipertensivo mais prevalente foi a pré-eclâmpsia (74,0%) seguido da hipertensão arterial crônica (11,0%) e eclâmpsia (6,0%). Hemorragia foi observada em 19,0% das mulheres. O tratamento mais utilizado foi a hidratação (70,0%) e oligúria representou uma das consequências da LRA mais prevalente (84,8%). Hemodiálise foi necessária em 13,0% dos casos e 4,0% evoluíram para o óbito. A recuperação da função renal ocorreu até a alta em quase 70,0% dos casos. As principais causas de LRA foram os distúrbios hipertensivos e hemorragia/choque hemorrágico.
Palavras-chave:
Lesão renal aguda, Gestação, Unidade de terapia intensiva
IntroductionAcute kidney injury (AKI) is a syndrome characterized by an abrupt decrease of the glomerular filtration rate (GFR) in such a level that the elimination of residual products such as urea, creatinine and other uremic toxins is diminished.
1There is still a relevant discussion regarding its diagnosis. Currently, the parameters used for AKI diagnosis were established in 2004 by the criteria of Risk, Injury, Failure, Loss, End-Stage (RIFLE), and in 2007, the criteria of Acute Kidney Injury Network (AKIN).
2,3AKI may occur at any stage of pregnancy, prepartum or postpartum. There are two frequency peaks, one in the first trimester, associated with infections (usually septic abortions) and the other one in the third trimester and puerperium, related to obstetric complications, mainly hemorrhage and hypertension.
1As with the general population, the AKIs are divided into three groups: prerenal, intrarenal and postrenal. The prerenal AKI is observed when the decline of kidney function occurs due to a physiological response to kidney hypoperfusion, however without structural malformation in the cell. The intrarenal causes occur due to direct lesion on the renal parenchyma, and the postrenal causes are related to obstructions in the urinary tract.
4Although it is considered a rare event in obstetric patients, AKI is a serious complication of the pregnancy-puerperal cycle, and its main causes are prepartum and postpartum hemorrhage, hypertensive syndromes and sepsis. Due to higher maternal age and the increase of incidence of hypertensive disorders in pregnancy, the rates increased almost three times in the last decades in the United States, however the AKI incidence related to pregnancy is low in developed countries due to better prenatal care.
4Observing the frequency and severity of this disease in women in the pregnancy-puerperal cycle, besides the scarcity of studies about this subject and data from our region, being aware that the early screening and the adequate conduction of the condition modifies the prognosis of the renal patient, we believe that it is relevant to identify characteristics inherent to women with AKI in the pregnancy-puerperal cycle.
5Thus, the present study was performed with the attempt of reporting the sociodemographic, clinical and obstetric profile of women with AKI hospitalized in the obstetric ICU in a reference maternity hospital in Recife – PE.
DescriptionA case series was performed, including patients hospitalized in the obstetric ICU of the maternity of the Institute of Integrative Medicine Professor Fernando Figueira (IMIP), in Recife, Pernambuco, Brazil, which had AKI in the pregnancy-puerperal cycle, during the period between September 2012 and September 2013.
For data collection, a list of all patients discharged from the obstetric ICU was generated, with the identification of AKI cases. Afterwards, the medical records from the medical files service were retrieved. Information obtained from the records were registered in a specific form.
Sociodemographic, clinical and obstetric characteristics were described; as well as the possible AKI causes, the most altered laboratory parameters, the treatment used (conservative or dialysis) and the consequences or complications of AKI.
Women in the pregnancy-puerperal cycle with AKI diagnosis during the hospitalization in the obstetric ICU of IMIP were included, Acute Kidney Injury was defined as the presence of oliguria (diuresis below 25 ml/h) or the increase of nitrogen excretion at any moment of the hospitalization.
For data processing and analysis, the Epi-Info 7.1 software was used. Tables of distribution of frequency were built for the categorical variables. For the quantitative variables, the measurements of central tendency and dispersion were calculated.
The project was approved by the Research and Ethics Committee of the Institute of Integrative Medicine Professor Fernando Figueira, under number 3731-13, September 12, 2013. Since it is a retrospective research, it was not possible to contact all women in the sample, so we solicited the exemption of the Free and Informed Consent Form.
DiscussionIn the study period, there were 6518 births in the service, with 1676 women being admitted to the obstetric ICU. There were reports of acute kidney injury in 113 patients. After checking the eligibility criteria, 13 patients were excluded (five patients who had an incomplete record, hindering the adequate assessment and eight that did not match AKI diagnosis after a rigorous review of their records). Considering every woman admitted to the ICU, AKI was diagnosed in 6.0% of the hospitalizations, corresponding to 1.5% of every birth that took place in the service during the study period.
The age of the patients varied from 14 to 44 years, with a mean age of 25.5 years. Most were brown (64.1%), had a partner (76.6%) and 47.4% were from the countryside of Pernambuco. Regarding the schooling level, 57.3% had complete high school and 30.0%, elementary school.
With regard to parity, 65 (65.1%) were primigravidae. Most women (90%) were puerperal in the moment of admission at ICU, and of the 10 women that were hospitalized pregnant, the mean gestational age of ICU hospitalization was 26 weeks. The most frequent type of delivery was cesarean section (75.5%). Most pregnant women have had some prenatal consultation (97.5%) (Table 1).
Concerning the main AKI causes, 91% of patients presented hypertensive disorders. Preeclampsia was the main clinical form of hypertension (74.0%). Among other causes, the one that stood out the most was hemorrhage/hemorrhagic shock, corresponding to 19.0% of patients.
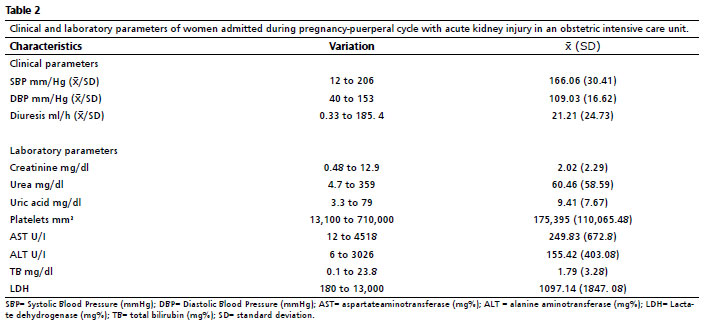
Considering the worst clinical and laboratory parameters found, we observed a mean systolic blood pressure (SBP) of 166 mmHg and a mean diastolic blood pressure of 109 mmHg. In relation to serum levels of urea, the mean was 60.4 mg% when considering the worst parameter and 96.9% of women presented urea level above 10mg% during hospitalization. With regard to creatinine, the mean was 2.0 mg% when considering the worst parameter and creatinine above 0.5mg% was observed in 94.5% of women. Concerning hourly diuresis analyzed during the hospitalization, we observed a mean of 21.2 ml/ and a percentage of 84% of women that presented diuresis under 25ml/h during hospitalization. Platelet count had a mean of 175,395/mm
3, and 18,000/mm
3 was the worst parameter found. Thrombocytopenia under 100,000/mm
3 was observed in little more than 30.0% of patients. The AST (aspartate aminotransferase) values varied from 12.0 and 4518.0 U/I (mean= 249.8U/I), whilst the ALT (alanine aminotransferase) was from 6.0 to 3026.0 U/I (mean = 155.4U/I). The LDH (lactate dehydrogenase) varied from 180.0 to 13,000.0 U/L, mean = 1097.1U/L. The total bilirubin (TB) varied from 0.1 to 23.8mg/dl with a mean of 1.7mg/dl, in relation to the worst parameters found (Table 2).
The results of our study demonstrate that, in spite of being rare in the general obstetric population, when selecting high-risk pregnant women, acute kidney injury is frequent, corresponding to 6% of admissions to obstetric ICU and aggravating significantly the maternal prognosis. This frequency was lower than those observed in other studies also carried out in Brazilian obstetric ICUs, which demonstrated a frequency of acute kidney injury of approximately 20% of admissions,
6 however, it was similar to that of a study conducted in 2014, in Egypt.
7 It is possible that the more severe admission criteria adopted in an ICU may modify the frequency of AKI, besides, since it is a study carried out from a hospital discharge diagnosis, and not from the individual assessment of each admission, it is possible that patients that could have the diagnosis were not included.
With regard to the distribution of AKI causes, we found predominance of hypertensive disorders, hemorrhage and sepsis, in this order. Other studies published also found results similar to the present casuistry.
8,9The present study, in a similar manner to other case series about AKI in the pregnancy-puerperal cycle,
10,11 demonstrated a predominance of AKI cases in puerperal women. This higher prevalence at puerperium may be related to the profile of our patients in relation to the AKI cause, since in our casuistry, hypertensive disorders predominate, which many times imply an early interruption of the pregnancy with referral to ICU only at puerperium. It is relevant the fact that only three women that were admitted in the study demonstrated AKI with 20 weeks or less of pregnancy. In Brazil, in spite of abortion is not yet legal, the techniques adopted for insecure pregnancy interruption usually involve the use of prostaglandins, which decreases the frequency of septic abortions and may explain this finding.
As clinical parameters, SBP, DBP and diuresis at admission were assessed, and its worst parameters. Articles approaching this subject are still scarce, and it is not well elucidated which are the real values for blood pressure to the development of AKI, however, a study conducted in Brazil
6 demonstrated similarity to what was found in the present study.
Most of our patients demonstrated oliguria (84.6%) at some moment, however, this diuresis was recovered during 24 hours with the use of hydration and/or medicines.These data differ from those found in a study from Morocco
8, in which around 33% of women presented oliguria, however, in this case, the 24 hours diuresis was always assessed, and not the daily variations such as was done in the present study. A study carried out in India,
12 however, describes a frequency of oliguria of 64%, closer to our data.
Oliguria is one of the most described characteristics in studies, and most patients demonstrated oliguria.
6,8 This finding is very important, since it was demonstrated that presented higher time of oliguria had an impaired kidney recovery, so that it is an important mortality predictor.
13 In spite of the majority of our patients presented oliguria at some moment, the recovery of kidney function was high, which probably explains our relatively low mortality rate, of 4%. A similar result was found in other study,
9 in which 6% of patients evolved to death, whilst another study found a largely higher mortality, of 28%.
6,8 In spite of a lower mortality found in our sample, we still consider that it is a high mortality rate for an obstetric population, composed generally by women previously healthy, corroborating the severity of this diagnosis.
In relation to laboratory characteristics of patients, there are few studies describing with details the level of exams found. The mean platelet count in admission was 168,975/mm
3, higher to that found by another author (94,969/mm
3).
6 Analyzing the levels of transaminases, urea, creatinine, AST, ALT and LDH in admission were lower than those found in a study carried out in Fortaleza-CE.
6 In relation to laboratory exams found with the patients of the present study, we may consider that a predominance of milder levels of the disease had occurred, due to the rigorous screening and early stage diagnosis. We may also relate this difference to the higher severity of the group of patients in the aforementioned study, in which all of the patients need to have dialysis, thus leading to a significant increase of these transaminases.
We consider, however, that the described results add important points to the current knowledge on AKI in pregnancy and may represent the starting point for other studies, since they are still scarce in the country and in the region. For a more accurate investigation, other prospective studies are necessary, with broader casuistries, besides the urgency of validation for diagnosis criteria for AKI in this group of patients.
The results found in the present study are important and corroborate the data found in the literature, which affirm the severity of AKI. However, further prospective studies are necessary to elucidate the main risk factors that lead to the development of the disease in women at the pregnancy-puerperal cycle, so that we can early intervene with the attempt of decrease the development of complications that put the life of the mother-child binomial at risk. Besides, it is primordial to repeat similar analyses currently, in order to evaluate, inclusively, if there was modification in the characteristics of patients attended at the unit.
The severity of this condition justifies the importance of studying women that develop this intercurrence, attempting to early identify those who present higher risk of developing AKI.
References1. Hong S, Fang N. Clinical characteristics and prognosis of postpartum acute kidney injury. J Int Med Res. 2021; 49 (2).
2. Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P, ADQI workgroup. Acute renal failure – definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Critical Care. 2004, 8: 204-12.
3. Mehta RL, John A, Kellum JA, Shah SV, Molitoris BA, Ronco C,
et al. Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Critical Care. 2007; 11: 1-8.
4. Elizabeth TH, Silvi S. Acute kidney injury in pregnancy. Adv Chronic Kidney Dis. 2020; 27: 455-60.
5. Srinil1 S, Panaput T. Acute kidney injury complicating septic unsafe abortion: clinical course and treatment outcomes of 44 cases. J Obstet Gynaecol Res. 2011 Nov; 37: 1525-31.
6. Geraldo BSJ, Suzanne VS, Gabriel CC, Vanessa RV, Juliana GRO, Amanda MTR,
et al. Lesão renal aguda em pacientes obstétricas gravemente doentes: um estudo transversal em uma unidade de terapia intensiva do nordeste do Brasil. Braz J Nephrol. 2017; 39: 357-61.
7. Godara SM, Kute VB, Trivedi HL, Vanikar AV, Shah PR, Gumber MR,
et al. Clinical Profile and Outcome of Acute Kidney Injury Related to Pregnancy in Developing Countries: A Single-Center Study from India. Saudi J Kidney Dis Transpl. 2014; 25: 906-11.
8. William RC, Ulla KH, Alison LC, Chimwemwe JM, Priscilla M, Ausbert M,
et al. Incidence, aetiology and outcomes of obstetric-related acute kidney injury in Malawi: a prospective observational study. BMC Nephrol. 2018; 19-25.
9. Viana RC, Novaes MRC, Calderon IMP. Mortalidade Materna - uma abordagem atualizada. Com Ciênc Saúde. 2011; 22 (Supl. 1): S141-52.
10. Kamal EM, Behery MM, Sayed GA, Abdulatif HK. RIFLE classification and mortality in obstetric patients admitted to the intensive care unit with acute kidney injury: a 3-year prospective study. Reprod Sci. 2014; 21: 1281-7.
11. Sivakumar V, Siivaramakrishna G, Saimaresh VV, Sriramnaveen P, Krihnakishore C, Rani CS,
et al. Pregnancy-related acut renal failure: a ten-year experience. Saudi J Kidney Dis Transpl. 2011 Mar; 22 (2): 352-3.
12. Ferreira DP, Amorim FF, Matsuura AJ, Sousa JL, Santana AR, Souza JA,
et al. Pregnancy‑related acute kidney injury: mortality and survival of patients treated at a maternal intensive care unit. J Nephrol. 2020 Dec; 33 (6): 1361-7.
13. Gurrieri C, Garovic VD, Gullo A, Sprung KBJ, Narr BJ, Weingarten TN. Kidney injury during pregnancy: associated comorbid conditions and outcomes. Arch Gynecol Obstet. 2012; 286: 567-73.
Author's contributionSouza I,Katz L, Coutinho I and Amorim MM: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review and editing.
All authors approved the final version of the article and declare no conflicts of interest.
Received on July 4, 2023
Final version presented on October 17, 2023
Approved on October 23, 2023
Associated Editor: Alex Sandro Souza


 ; Leila Katz2
; Leila Katz2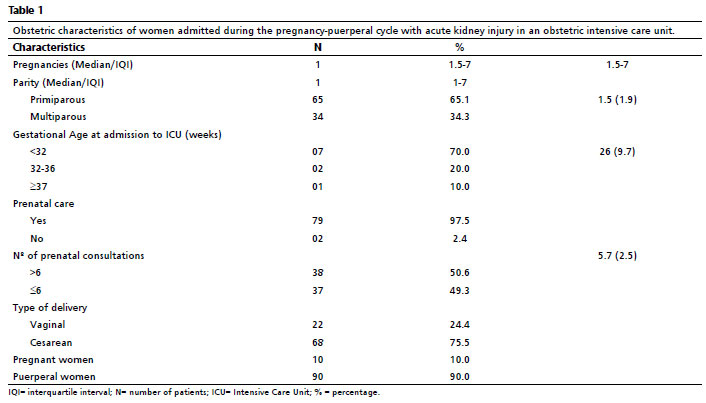






 Ler em português
Ler em português