ABSTRACT
OBJECTIVES: to analyze the temporal trend in maternal, care and newborns characteristics, in the city of Guarapuava, Paraná, Brazil in the period of 2010 to 2019.
METHODS: ecological temporal tendency study is based on Sistema de Informações sobre Nascidos Vivos (Live Birth Information System). To verify changes on the topics, the Prais-Winsten generalized linear regression was applied.
RESULTS: data from 28,919 live births were analyzed in 2019, 15.9% of the pregnancies were adolescents, 49.8% were cesarean deliveries and 9.2% were premature childbirths. A reduction in teenage pregnancy was observed, with annual percentage variation (APV) for mothers aged ten to 14 being -0.14% (p=0.005) and 15 to 19 years old -0.82% (p=0.004); there was an increase in mothers' schooling, with an APV of 60.09% (p=0.026) for eight to 11 years of schooling and 11.27% (p<0.001) for 12 or more; there was an increase of 15.33% (p<0.001) for seven or more prenatal consultations and a decrease in the Apgar classifications considering the risk, with scores from zero to two in the 1st minute with an APV=-0.12 (p=0.010) and scores from three to five in the 5th minute with APV=-0.07 (p=0.011).
CONCLUSIONS: The city of Guarapuava presents important decreased tendencies in early pregnancy and an increase in mothers' schooling, besides the changes regarding the conditions in which their children are born and how they are welcomed.
Keywords:
Time series studies, Health information systems, Birth certificates, Pregnancy in adolescence, Prenatal care
RESUMO
OBJETIVOS: analisar a tendência temporal de características maternas, assistenciais e dos recém-nascidos do município de Guarapuava-PR no período de 2010 a 2019.
MÉTODOS: estudo ecológico de tendência temporal com dados do Sistema de Informações sobre Nascidos Vivos. Para verificar mudanças nas características avaliadas, utilizou-se regressão linear generalizada de Prais-Winsten.
RESULTADOS: analisaram-se dados de 28.919 nascidos vivos; em 2019, 15,9% das gestações foram de adolescentes, 49,8% dos partos cesáreos e 9,2% partos prematuros. Observou-se redução da gravidez na adolescência, com variação percentual anual (VPA) para mães com dez a 14 anos sendo -0,14% (p=0,005) e 15 a 19 anos -0,82% (p=0,004); aumento da escolaridade das mães, com VPA de 60,09% (p=0,026) para oito a 11 anos de estudo e 11,27% (p<0,001) para 12 ou mais; aumento de 15,33% (p<0,001) para sete ou mais consultas de pré-natal realizadas pelas gestantes e queda nas classificações de Apgar consideradas de risco, com notas zero a dois no 1º minuto com VPA=-0,12 (p=0,010) e notas três a cinco no 5º minuto com VPA=-0,07 (p=0,011).
CONCLUSÕES: Guarapuava apresentou importantes tendências de redução da gravidez precoce e aumento de escolaridade das mães, além de mudanças sobre as condições em que nascem seus filhos e sobre como são acolhidos.
Palavras-chave:
Estudos de séries temporais, Sistemas de informação em saúde, Declaração de nascimento, Gravidez na adolescência, Cuidado pré-natal
IntroductionThe
Sistema de Informações sobre Nascidos Vivos (Sinasc) (Information System on Live Births) was implemented nationally by the Ministry of Health in 1990 aiming to generate indicators on prenatal, childbirth care and the epidemiological profile on live births.
1,2 The
Declaração de Nascido Vivo (DNV) (Live Birth Statement) is used as the standard document throughout the country.
3 Since its implementation, the system has evolved in terms of coverage and quality,
1,2 with estimated coverage of 98% in 2015.
1Time series studies from the 2000s onwards using Sinasc data have been carried out in local, regional and national level, showing changes in maternal, care and newborns characteristics.
4-12In two studies, one being local (Niterói-RJ) between 2000 and 2009
4 and the other national from 2008 to 2017,
9 there was a descrease on teenage pregnancy, but with the macro-regional diferences, the North and Northeast have the highest prevalence rates when comparing to the other macro-regions.
9 Childbirths also increased in Niterói-RJ
4 with mothers aged 35 or over and their schooling profile showed a significant improvement in the analyzed period. Another study was carried out with data from cities in the extreme South of Bahia State between 2002 and 2017 also highlights an improvement on pregnant women's schooling level of.
10With regard to the characteristics of care provided to pregnant women, several studies pointed out an increase of seven or more prenatal consultations,
7,10,11 although this increase is unequal when looking at schooling, race/color, age and marital status.
7,11 From the point of view in childbirth care, several studies highlight the increase in surgical birth rates.
4,5,10,12 A national survey from 2000 to 2010 showed an association between cesarean sections and an increase in maternal age and schooling,
5 and another national survey with data from 1994 to 2019 points out to a projection of 57.4% of cesarean sections in the country by 2030 and proportions of over 70% in the Southeast and South regions.
12Two local studies were carried out in Niterói-RJ
4 State and Botucatu-SP
6 State between 2000 and 2010 and a regional study in cities in the extreme South of Bahia State
10 between 2002 and 2007 and 2012 and 2017 that assessed newborns' characteristics shortly after childbirth, revealed an increase in prematurity
4,6,10 and a decrease in low birth weight.
4 While a national study was carried out between 2012 and 2019 reported a decreased trend in prematurity, from 10.87% to 9.95%, especially among the most vulnerable women (illiterate and indigenous);
8 also in this study, women aged 45 or over and with four to six prenatal consultations had the highest proportions of prematurity.
8The possibility of analyzing information from the system in a city level facilitates the planning on health actions and the implementation of programs in the area of care for women and children, and also supports the monitoring in committees of infant and maternal mortality. Considering the importance of decentralizing health actions, some studies have advocated the Sinasc data analysis at a local level,
4,6,10,13 but some cities have not yet carried out such studies.
In view of the above, the aim of this study was to describe the temporal trend on maternal, care and newborns characteristics in the city of Guarapuava-PR from 2010 to 2019, based on data obtained from Sinasc, in an attempt to ascertain whether there have been any changes in these characteristics over the evaluated time.
MethodsThis is an ecological temporal trend study on maternal, care and newborns characteristics in the city of Guarapuava-PR in a ten-year period (2010 to 2019) using data available on Sinasc in 2021.
Sinasc allows the following selections: city; place of birth; mother's age, schooling and marital status; length of pregnancy; type of pregnancy; adequacy of the number of prenatal consultations; type of delivery; prenatal consultations; sex; newborn's color/race; Apgar 1
st and 5
th minute; birth weight; congenital anomaly and type of congenital anomaly.
The study participants were all live births and their mothers considering births by residence from 2010 to 2019, were available on Sinasc.
The maternal variables considered for the study were: age; schooling; marital status and type of pregnancy; the care variables were: place of birth; type of delivery; number of prenatal consultations; the newborns variables were: length of pregnancy; gender; color/race; 1
st minute Apgar; 5
th minute Apgar; birth weight and congenital anomaly.
The dependent variables were maternal, care and newborns. As an independent variable, we used the years of the time series (2010 to 2019). The categorization of most of the variables followed the distribution adopted in Sinasc and in studies based on this system and its variables.
4-6,14,15The data was extracted from the
Departamento de Informática do Sistema Único de Saúde (DATASUS)
15 (Informatics Department of the Public Health System) and entered into the Microsoft Excel
® program for later analysis.
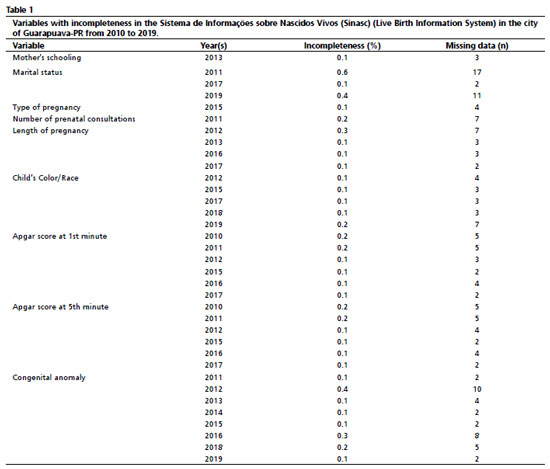
Incompleteness data was calculated based on the number of missing data for each of the maternal, care and newborns variables in the years covered by the study, using the scale suggested by Romero and Cunha
16 as a reference point: excellent, when the variable is incomplete by less than 5%; good (5 to 10%); fair (10 to 20%); poor (20 to 50%); and very poor (50% or more).
The time trend analysis of the characteristics mentioned was carried out using the generalized Prais-Winsten
17 linear regression in the IBM SPSS (Statistical Package for the Social Sciences) version 25.0. This regression method was chosen because of the autocorrelation serial often found in population data measurements.
17According to Antunes and Cardoso
17 the prevalence values of the maternal, care and newborn characteristics analyzed in the city should be log-transformed in order to reduce the heterogeneity of variance in the regression analysis residuals.
The rates of annual increase in the prevalence of maternal, care and newborns characteristics, as well as the respective confidence intervals, were obtained by applying the following formulas:
17,18 Annual increase rate=(-1+10β)*100%
CI95%=-1+10(β ±t(0.05;n-1)xEP)
The regression coefficient (β) and the standard error (SE) of the beta estimate were provided by the Prais-Winsten regression, and the t-value was obtained from the two-tailed Student's t-distribution table, with a 5% significance level, considering the number of years in the series -1
10,18,19The time trend was interpreted by looking at the confidence interval; when the value zero was contained in the interval, the trend was considered stationary; otherwise, the trend would be increasing while the rate of increase was positive, or decreasing when it was negative, when
p<0.05.
Due to the nature of the study and the use of a database in the public domain and without the possibility of identifying the individual, the study did not need to be assessed by a
Comitê de Ética em Pesquisa com Seres Humanos (COMEP) (Human Research Ethics Committee), in accordance with
Conselho Nacional de Saúde (CNS) (National Health Council) Resolution 510 of April 7, 2016.
20ResultsData was analyzed referring toa total of 28,919 newborns between 2010 and 2019, taking into account births per household in the city of Guarapuava-PR. Regarding data incompleteness, there was a 100% reduction in incompleteness for the variables "Apgar 1st minute" and "Apgar 5th minute", both of which went from 0.2% of ignored data in 2010 to 0% in 2019 (Table 1). The variables "mother's age", "place of birth", "type of delivery", "child's sex" and "birth weight" did not show missing records in any of the years evaluated.
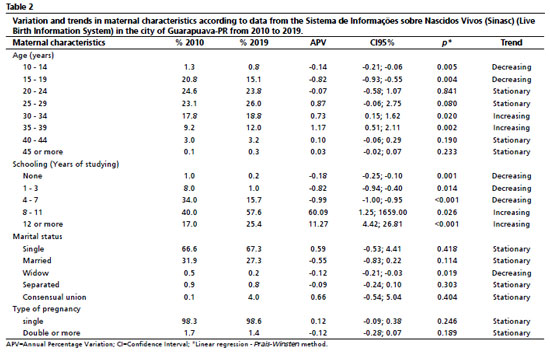
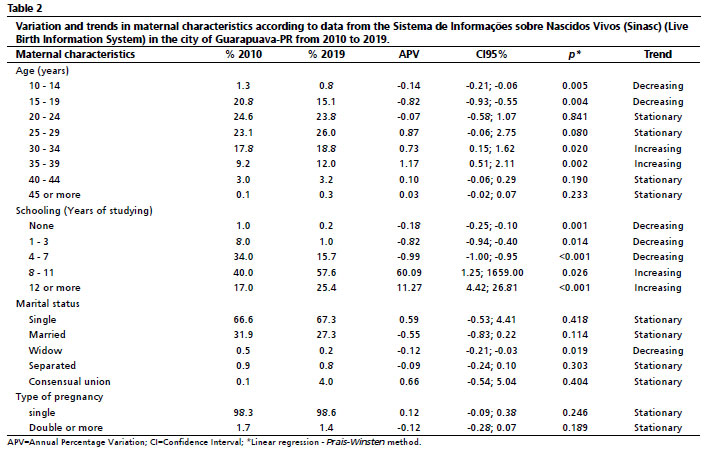
Among the main maternal characteristics, the prevalence of teenage pregnancy was 22.1% in 2010 and 15.9% in 2019, as described in Table 2. Regarding the variation and trend of these characteristics, there was a decrease in the proportion of teenage mothers (10-14 and 15-19 years) and an increasing trend in the 30-34 and 35-39 age groups. The "mother's schooling" variable (in years of schooling) showed a decreased trend for lower levels of schooling (none, one to three and four to seven years) and an increased trend for higher levels of schooling (8-11 and 12 or more). As for the "mother's marital status" variable, the proportion of widowed mothers showed a decreased trend (Table 2).
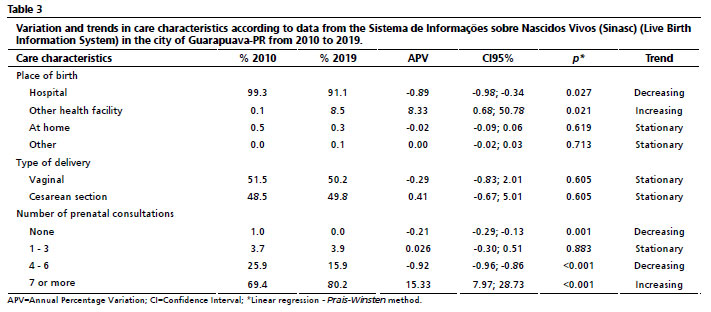
With regard to the indicators related to care characteristics, Table 3 shows that more than ninety percent of births took place in hospitals. The number of births in hospitals showed a decreased trend, while the number of births in other health establishments showed an increased trend. The percentage of cesarean sections was close to that of vaginal births (50%) and the trend of vaginal and cesarean births showed a stationary trend. As for the number of prenatal consultations carried out by the mother, there was an increased trend towards seven or more consultations (Table 3).
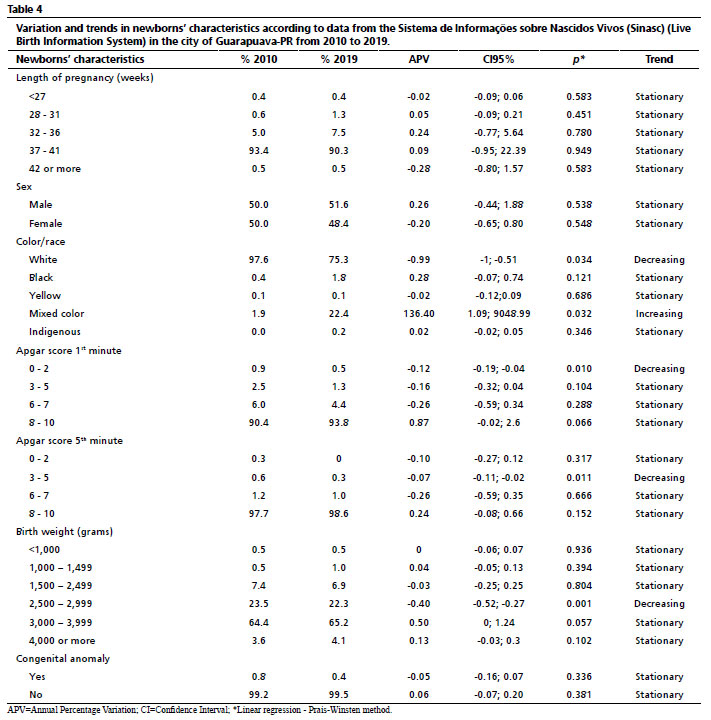
From the data obtained on the newborns' characteristics (Table 4), prematurity, considering live births under 37 weeks, was 6% in 2010 and rose to 9.2% in 2019. For the "color/race" variable, there was a decreased trend for the identification of "white" and an increased trend for "mixed color". With regard to the Apgar score in the 1
st minute of the newborns' life, there was a decreased trend for those who received a score between zero and two. As for the Apgar score in the 5
th minute, there was a decreased trend in newborns classified with scores between three and five. The prevalence of low birth weight (<2,500 grams) was 8.4% in 2010 and 2019. There was a decreased trend for the birth weight ranging from 2,500 to 2,999 grams (Table 4).
DiscussionThe variables analyzed using Sinasc over the ten years of the study in the city of Guarapuava-PR showed excellent data completeness. Regarding to maternal characteristics, the decrease in teenage pregnancies and the increase in maternal schooling levels were highlighted. In terms of care, there was a decrease in births in hospital environment and an increase in births in other health facilities, as well as an increase in pregnant women having seven or more prenatal consultations. Newborns showed a decreased trend in white racial identification and an increase in mixed color racial identification, as well as a decrease in lower Apgar scores in the 1
st and 5
th minutes.
In terms of data completeness, the city of Guarapuava showed high rates of completion, and there was a general increase on the information of the categories that had some percentage of data ignored in the initial years of the survey. According to Romero and Cunha's criteria,
16 all the variables, except marital status in 2016, had an "excellent" rating, since none of them had more than 5% incompleteness over the studied years. This quality of data is of great importance for studies such as this one, providing a basis sociodemographic analysis.
2,10,21With the changes made to the DNV since 2011 and the work of the Cities Health Departments in training staff to fill it out the questionnaire correctly, there has been a significant improvement in the completeness of most of the Sinasc variables.
1,14Despite this improvement, a review of the literature on analyzing the quality of Sinasc data points out to the main factors that can lead to ignored or blank data that still persist, such as: deficiencies related to the professional responsible for filling out the DNV, methodological problems in the definitions of how to fill in the variables and data that is difficult to obtain due to the lack of knowledge or refusal of the informant.
21Regarding the maternal profile, there was a reduction in teenage pregnancies, which corroborates a national study that showed a reduction of 37.2%, with the percentage of teenage mothers decreasing from 23.4% in 2000 to 14.7% in 2019.
22 While two studies were carried out in the North region reported higher prevalences of teenage pregnancy, 25.48% in Acre State between 2015 and 2019 and the values ranging from 14.2% to 21.4% in the health regions of Rondônia State in 2019.
23,24 These findings reinforce regional differences, showing that the South and Southeast regions show an improvement in this indicator when compared to the North, Northeast and Midwest regions.
9,22 The findings of trends in maternal characteristics are comparable to those studies in other Brazilian regions which have also pointed out to a reduction in teenage pregnancies,
4,9,22 an increase in the number of older mothers
4 and an increase in these women's schooling level.
4,10Brazil, like other developing countries, underwent significant modernizations in terms of economic and social development during the 20th century, which were accompanied by important changes in demographic issues.
25 The increase in schooling, which was related to better use of health services, associated with the greater inclusion of women in the job market and access to and improvement of contraceptive methods, has led many women to overcome social determinants and seek family planning, reducing their fertility rates and having pregnancies at older ages than before.
25,26Thus, the data obtained for both maternal age and schooling in the city of Guarapuava is in line with this scenario of advances in education and family planning. However, it is important for local health care to be prepared for the possible consequences of the trend towards pregnancies at older ages, in view of the repercussions as in gestational, maternal and perinatal levels.
4,25,26Regarding the results on women's marital status analyzed, findings in the literature describe a possible association between the absence of marital support and the tendency to manifest depressive conditions and high levels of stress among pregnant women,
23,24 while the presence of marital support was associated with greater adherence at prenatal care. Thus, the decreased trend in the prevalence of widowed mothers found may indicate a beneficial factor for the local health situation.
There was also an evidence of decreased trend for childbirths in hospitals and an increased trend in other health facilities. No studies were found that investigated changes in the pattern of seeking out other health facilities for childbirth. The literature consulted describes that in Brazil, 2-3% of childbirths take place in other health facilities that are not counted as hospital childbirths, and depending on the State and region of the country this figure can reach 9%.
27 This result requires further investigation for this change, possibly considering other variables such as maternal/family income.
Cesarean deliveries were close to the 50% level, which is high for the city, but this is the reality in cities and States that have reported figures that can reach 60% and more than 80% depending on the evaluated health region.
4,24,28 The stationary trend in cesarean deliveries should be analyzed by health managers as a result in being improved, seeking a decrease in births by this form of delivery. A study carried out in Patos de Minas-MG State between 2011 and 2015 found a significant association between surgical deliveries and maternal age over 35 and a higher number of prenatal consultations.
13Despite the stationary trend related to cesarean deliveries, there was an increase in the number of prenatal consultations attended by seven or more pregnant women in this study. This result represents a significant advance for the city of Guarapuava, which in 2006 stood out among the cities in the regional health district in Paraná State as having the highest rate of pregnant women with an insufficient number of prenatal consultations (51.3%).
29 This increase in adherence and access to prenatal care is also described in other national studies
1,7,11 and local data,
10,23 which signals an important advance when it comes to pregnant women and newborns' health in Brazilian cities.
The prevalence of prematurity was similar to other studies4,
24,28 and the trend in rates was stationary. Local studies was carried out in Niterói-RJ State between 2000 and 2009,
4 in Botucatu-SP State between 2001 and 2010,
6 and in States in the extreme South of Bahia between 2002 and 2007 and 2012 and 2017
10 showed an increase in the trend of prematurity, while a national study was carried out between 2012 and 2019
8 signaled a decreased trend in these rates. The cities should join forces to reduce prematurity rates by monitoring premature births, identifying their determinants and following the evolution of their occurrence in specific contexts, in order to draw up policies and early interventions for the health of pregnant women and children.
6There has been an increasing trend towards identifying newborns as mixed color which, from the point of view of health management, is essential to analyze vulnerabilities and intervention needs.
30 Although race/color is an objective variable, it can have a subjective classification due to the circumstances and context of the investigation.
30 In the city of Guarapuava, it was possible to verify that those responsible for the newborn seem to be more capable and confident in identifying the color of their child.
A decreased trend was recognized in some risk in the Apgar scores, an important factor for the scenario of the city, given that in the study by Melo and Mathias,
29 the city of Guarapuava stood out for its high rate of Apgar scores of less than eight in the 5
th minute, a score which can indicate fetal anoxia and is related to a greater demand of resources and a greater risk of morbidity and mortality for the newborn.
3,29The proportion of low birth weight was similar to local and State studies,
4,24,28 and a decreased trend was identified in the birth weight ranging in 2,500 to 2,999 grams, considered as sufficient for World Health Organization standards. However, there were no changes in trends for other weight categories, which is of no concern to the city at the moment, although constant monitoring of this variable is necessary.
The limitations of this study include the use of secondary data obtained directly from Sinasc, which depends on entering the data contained in the DNV, which was not analyzed in the current study; and the fact that other variables collected in the DNV, which are not publicly available in Sinasc, such as the mother's color/race, parity and maternal occupation, were not evaluated.
The study showed changes in the maternal-infant, and care at birth characteristics in the city of Guarapuava-PR between 2010 and 2019. A new reproductive profile was observed, with a trend towards an increase in women's age and schooling, the search for health facilities other than hospitals for childbirths, as well as an increase in the number of prenatal consultations. In addition, there was a greater racial identification of the newborn, as well as some trends in relation to their survival which are extremely important for assessing the quality of the health service offered, both in prenatal care and during the perinatal period, such as the Apgar score.
Further studies are needed as for specific factors that lead to the trends in each variable and other variables included in the DNV that were not analyzed, but which may interfere with maternal and neonatal health outcomes.
References1. Ministério da Saúde (BR). Como nascem os brasileiros: uma análise da adequação da assistência pré-natal e das indicações de cesárea por critérios de risco epidemiológico a partir do Sinasc. In: Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância de Doenças e Agravos não Transmissíveis e Promoção da Saúde. Saúde Brasil 2017: uma análise da situação de saúde e os desafios para o alcance dos Objetivos de Desenvolvimento Sustentável. Brasília (DF): Ministério da Saúde; 2018. p. 19-38. [access in 2023 Jul 20]. Available from:
http://tabnet.datasus.gov.br/cgi/sinasc/saude_brasil_2017_analise_situacao_saude_desafios_objetivos_desenvolvimento_sustetantavel.pdf2. Szwarcwald CL, Leal MC, Esteves-Pereira AP, Almeida WS, Frias PG, Damacena GN,
et al. Avaliação das informações do Sistema de Informações sobre Nascidos Vivos (SINASC), Brasil. Cad Saúde Pública. 2019; 35 (10): e00214918.
3. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Análise Epidemiológica e Vigilância de Doenças Não Transmissíveis. Declaração de Nascido Vivo: manual de instruções para preenchimento. 4
th ed. Brasília (DF): Ministério da Saúde; 2022. [access in 2023 Nov 06]. Available from:
https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/svsa/vigilancia/declaracao-de-nascido-vivo-manual-de-instrucoes-para-preenchimento4. Rozario S, Brito AS, Kale PL, Fonseca SC. Série temporal de características maternas e de nascidos vivos em Niterói, RJ. Rev Bras Saúde Mater Infant. 2013; 13 (2): 137-46.
5. Rattner D, Moura EC. Nascimentos no Brasil: associação do tipo de parto com variáveis temporais e sociodemográficas. Rev Bras Saúde Mater Infant. 2016; 16 (1): 39-47.
6. Balbi B, Carvalhaes MABL, Parada CMGL. Tendência temporal do nascimento pré-termo e de seus determinantes em uma década. Ciênc Saúde Colet. 2016; 21 (1): 233-41.
7. Mallmann MB, Boing AF, Tomasi YT, Anjos JC, Boing AC. Evolução das desigualdades socioeconômicas na realização de consultas de pré-natal entre parturientes brasileiras: análise do período 2000-2015. Epidemiol Serv Saúde 2018; 27 (4): e2018022.
8. Martinelli KG, Dias BAS, Leal ML, Belotti L, Garcia EM, Neto ETS. Prematuridade no Brasil entre 2012 e 2019: dados do Sistema de Informações sobre Nascidos Vivos. Rev Bras Est Pop. 2021; 38: e0173.
9. Dechandt MJ, Kluthcovsky ACGC, Pereira BLR, Wosniak EJM. Analysis of adolescent fertility rates and temporal trend in Brazil (2008 to 2017). Res Soc Dev. 2021; 10 (6): e19710615664.
10. Moraes MMS, Rocha EMS, Soares TFS, Moura GP, Nascimento MKF, Santos LS. Sistema de informações sobre nascidos vivos: Qualidade e perfil de nascimentos no extremo sul baiano. Rev Baiana Saúde Pública. 2021; 45 (2): 82-102.
11. Santos FL, Carvalho BC, Santos JCO, Ferreira LLL, Lima ACR. Panorama nacional da adesão ao pré-natal: série histórica de 2009 a 2018. J Nurs Health. 2022; 12 (1): e2212120433.
12. Pires RCR, Silveira VNC, Leal MC, Lamy ZC, Silva AAM. Tendências temporais e projeções de cesariana no Brasil, macrorregiões administrativas e unidades federativas. Ciênc Saúde Colet. 2023; 28 (7): 2119-33.
13. Silva EV, Costa MAA, Almeida KC, Araujo LMB, Amâncio NFG. Relação do tipo de parto com o perfil epidemiológico da assistência pré-natal e perinatal em um município de Minas Gerais. Rev Bras Saúde Mater Infant. 2020; 20 (1): 249-56.
14. Ministério da Saúde (BR). Coordenação Geral de Informações e Análises Epidemiológicas. Secretaria de Vigilância em Saúde. Consolidação do Sistema de Informações sobre Nascidos Vivos – 2011. Brasília (DF): Ministério da Saúde; 2013. [access in 2023 Jul 20]. Available from:
http://tabnet.datasus.gov.br/cgi/sinasc/Consolida_Sinasc_2011.pdf15. Ministério da Saúde (BR). DATASUS. Nascidos vivos - desde 1994 [
Internet]. Brasília (DF); 2023. [access in 2021 Mai 31]. Available from:
https://datasus.saude.gov.br/nascidos-vivos-desde-199416. Romero DE, Cunha CB. Avaliação da qualidade das variáveis epidemiológicas e demográficas do Sistema de Informações sobre Nascidos Vivos, 2002. Cad Saúde Pública. 2007; 23 (3): 701-14.
17. Antunes JLF, Cardoso MRA. Uso da análise de séries temporais em estudos epidemiológicos. Epidemiol Serv Saúde. 2015; 24 (3): 565-76.
18. Atty ATM, Guimarães RM, Andrade CLT. Tendência Temporal da Mortalidade por Câncer de Boca e da Cobertura de Atenção Primária no Estado do Rio de Janeiro. Rev Bras Cancerol. 2022; 68 (3): e-042082.
19. Aprelini CMO, Reis EC, Enríquez-Martinez OG, Jesus TR, Molina MCB. Tendência da prevalência do sobrepeso e obesidade no Espírito Santo: estudo ecológico, 2009-2018. Epidemiol Serv Saúde. 2021; 30 (3): e2020961.
20. Conselho Nacional de Saúde (BR). Resolução nº 510, de 7 de abril de 2016. Dispõe sobre as normas aplicáveis a pesquisas em Ciências Humanas e Sociais cujos procedimentos metodológicos envolvam a utilização de dados diretamente obtidos com os participantes ou de informações identificáveis ou que possam acarretar riscos maiores do que os existentes na vida cotidiana. Brasília (DF): DOU 25 de maio de 2016; Seção 1:46. [access in 2021 Fev 09]. Available from:
http://conselho.saude.gov.br/resolucoes/2016/Reso510.pdf21. Pedraza DF. Sistema de informações sobre nascidos vivos: uma análise da qualidade com base na literatura. Cad Saúde Colet. 2021; 29 (1): 143-52.
22. Monteiro DLM, Monteiro IP, Machado MSC, Bruno ZV, Silveira FA, Rehme MFB,
et al. Trends in teenage pregnancy in Brazil in the last 20 years (2000–2019). Rev Assoc Med Bras 2021; 67 (5): 759-65.
23. Silva SO, Fialho LL, Soares SS, Rodrigues ARM, Arruda EF. Características maternas de nascidos vivos no Acre: análise sociodemográfica e obstétrica entre 2015 e 2019. Rev Enferm Contemp. 2023; 12: e4853.
24. Amaral AD, Oliveira FT, Stevanato JM, Balestrin S, Mesquita JB. Características das mães e recém-nascidos em um estado da Amazônia legal. Braz J Develop. 2022; 8 (6): 43503-21.
25. Carreira GB, Dutra VGP, Silva JHCM, Guimarães RM. Desigualdade social, desenvolvimento humano e padrão de fecundidade no Brasil, 2000-2010. Rev Bras Saúde Mater Infant. 2019; 19 (1): 233-48.
26. Trigo IG, Eller JX, Vaz MR, Calil C, Silva LR, Barboza BP. Idade Materna Avançada e Seus Desfechos. Rev Cad Med. 2019; 2 (3): 146-51.
27. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Sistema de Informações sobre Nascidos Vivos (SINASC). Proporção de partos hospitalares [
Internet]. Brasília (DF); 2012. [access in 2024 Jan 08]. Available from:
http://tabnet.datasus.gov.br/cgi/tabcgi.exe?idb2012/f07.def28. Souza DML, Maia LCS, Zêgo ZDF, Jaeger GP, Maciel WS. Prevalência de prematuridade e fatores associados no estado do Rio Grande do Sul. Braz J Health Rev. 2019; 2 (5): 4052-70.
29. Melo EC, Mathias TAF. Características das mães e dos recém-nascidos em municípios-sede de regional de saúde no Paraná a partir dos dados do SINASC. Cogitare Enferm. 2010; 15 (2): 293-301.
30. Kabad JF, Bastos JL, Santos RV. Raça, cor e etnia em estudos epidemiológicos sobre populações brasileiras: revisão sistemática na base PubMed. Physis. 2012; 22 (3): 895-918.
Acknowledgements: We would like to thank the
Fundação Araucária de Apoio ao Desenvolvimento Científico e Tecnológico do Estado do Paraná for the Support of Scientific and Technological Development of the State of Paraná for the Scientific Initiation grant awarded to the first author.
Authors' contribution: Jardim IMM: data collection, analysis and interpretation; writing and final revision of the manuscript. Melhem ARF: analysis, interpretation of data and final revision of the manuscript.
Saldan PC: study design, data analysis and interpretation, drafting and final revision of the manuscript.
All the authors have approved the final version of the article and declare no conflicts of interest.
Received on May 16, 2023
Final version presented on February 7, 2024
Approved on February 16, 2024
Associated Editor: Karla Bomfim


 ; Angélica Rocha de Freitas Melhem2
; Angélica Rocha de Freitas Melhem2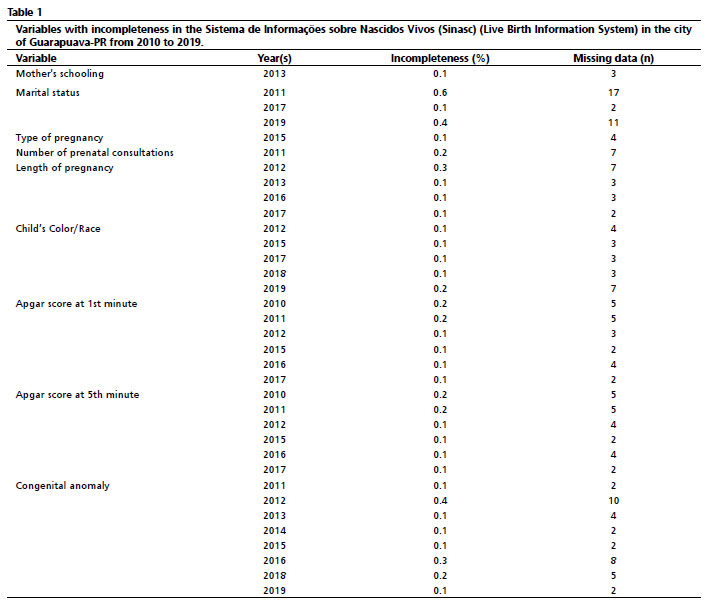






 Ler em português
Ler em português