ABSTRACT
OBJECTIVES: to analyze the trend and spatial distribution of hepatitis B in pregnant women in Brazil.
METHODS: ecological study based on all notified cases of hepatitis B in pregnant women through the Information System for Notifiable Diseases - Sinan between 2009 and 2018. Hepatitis B virus (HBV) detection rates were calculated in all municipalities. Spatial analysis was performed using the Global Moran Index for global data and local indicators of spatial association (Lisa) for the 5,570 municipalities. For trend analysis by State, the Prais-Winsten generalized linear regression model was used.
RESULTS: 15,253 pregnant women with HBV were reported. High detection rates were observed in the municipalities of São Miguel da Boa Vista-SC (68.96/1000 live births (LB)), Araguaiana-MT (68.18/1000 LB), Reserva do Cabaçal-MT (80, 00/1,000 LB), São Geraldo da Piedade-MG (75/1000 LB), Porto Mauá-RS (111, 11/1000 LB), in the respective bienniums. Moran (I) (I=0.056) showed a positive spatial association. In Lisa, 78 municipalities were included in the high-high cluster, 51.28% in the South region and 48 in the low-low cluster with 72.91% in the Southeast. There was an increasing trend in Maranhão (p=0.004) and Pernambuco (p=0.007) and a decrease in Mato Grosso (p=0.012), Paraná (p=0.031) and Santa Catarina (p=0.008).
CONCLUSION: the detection of hepatitis B in pregnant women was observed in most Brazilian municipalities, with an increasing trend in two states and a decrease in three others.
Keywords:
Hepatitis B, Information system, Pregnant women
RESUMO
OBJETIVOS: analisar a tendência e distribuição espacial da hepatite B em gestantes no Brasil.
MÉTODOS: estudo ecológico a partir de todos os casos notificados de hepatite B em gestantes pelo Sistema de Informação de Agravos de Notificação – Sinan entre 2009 e 2018. Foram calculadas as taxas de detecção do vírus da hepatite B (HBV) em todos os municípios. A análise espacial foi realizada por meio do Índice Global de Moran para os dados globais e os indicadores locais de associação espacial (Lisa) para os 5.570 municípios. Para análise de tendências por Estado, utilizou-se o modelo de regressão linear generalizada de Prais-Winsten.
RESULTADOS: foram notificadas 15.253 gestantes com HBV. Observou-se altas taxas de detecção nos municípios de São Miguel da Boa Vista-SC (68,96/1000 Nascidos vivos (NV)), Araguaiana-MT (68,18/1000 NV), Reserva do Cabaçal-MT(80,00/1.000 NV), São Geraldo da Piedade-MG (75/1000 NV), Porto Mauá-RS (111,11/1000 NV), nos respectivos biênios. Moran (I) (I=0,056) apresentou associação espacial positiva. No Lisa observou-se 78 municípios inserido no cluster alto-alto, sendo 51,28%na região Sul e 48 no cluster baixo-baixo com 72,91% no Sudeste. Verificou-se tendência crescente no Maranhão (p=0,004) e Pernambuco (p=0,007) e diminuição no Mato Grosso (p=0,012), Paraná (p=0,031) e Santa Catarina (p=0,008).
CONCLUSÃO: Observou-se a detecção de hepatite B em gestantes na maioria dos municípios brasileiros, com tendência crescente em dois estados e diminuição em outros três.
Palavras-chave:
Hepatite B, Sistema de informação, Gestantes
IntroductionHepatitis B isa highly contagious viral infection, caused by Hepatitis B virus (HBV), which has oncogenic potential and tropism associated with liver cells. Hepatitis B infection can result in either an acute infection or a chronic infection, the latter being responsible for the development of hepatic cirrhosis and/or hepatocellular carcinoma, standing out as a global public health problem.
1,2HBV prevalence is low in the national scope, although it is distributed heterogeneously, varying into less than 1% up to 8%, with states considered as having high prevalence, such as Acre, Rondônia, Amazonas, Paraná, Mato Grosso, Santa Catarina, Goiás, Pará, Minas Gerais, Rio de Janeiro, Bahia and Amapá.
3 This oscillation resounds in detection rates of pregnant women, since in this areas, the vertical and horizontal ways for close contact in childhood are the main forms of transmission of the virus.
4The worldwide prevalence of pregnant women with HBV varies from 0.32 to 14.02%,
5,6 while in Brazil, in studies carried out in several states, a variation of 0.13 to 1.9% was observed.
2,7-9 Even with the low endemicity, there is a risk of vertical transmission, when the mother infected by the virus transmits it to the newborn, mainly at the moment of birth and the perinatal period.
7 When newborns are infected, they can be chronic carriers in up to 90% of cases due to the immaturity of the immune system.
10Due to this, the serological screening of pregnant women during the prenatal period is mandatory, as well as the regularization of the vaccination situation when necessary. International and national health authorities recommend the execution of accessible and reliable diagnosis tests. The execution of HBsAg laboratory test or rapid test should occur in the first consultation, regardless of the gestational age, and at the third trimester of pregnancy.
7In cases of pregnant women with HBV, invasive procedures should be avoided and breastfeeding is not contraindicated. With regard to the newborn, in spite of maternal serology, it is recommended the first dose of the vaccine against Hepatitis B in up to 24 hours of birth. In front of positive maternal serology, the specific Hepatitis B Immune Globulin (HBIG) should also be administered in the first 12 hours of life.
11These procedures are due to strategies that aim to enhance the quality of assistance and humanization of care to pregnant women, and they are preconized by Brazilian health policies, attempting to ensure the birth of a healthy child and guarantee the wellbeing of both mother and baby.
12These measures show effectiveness in the reduction of vertical transmission, however, there are still flaws in the implementation of these strategies by health services, resulting in vertical transmission of HBV, as demonstrated in several studies carried out with pregnant women, punctually, in many locations of the country.
2,7,9,13,14 There is higher scarcity of studies that assessed the spatial distribution of Hepatitis B in this population.
15,16 In this way, the panorama of vertical HBV transmission in pregnant women is unknown at the local level in the country, even with the implementation of the Stork Network and others Networks of Healthcare that provide diagnosis tests of Hepatitis B, constituting the existence of possible barriers in healthcare access in the country's public health.
Thus, this study aims to analyze the trend and spatial distribution of Hepatitis B in pregnant women in Brazil, from 2009 to 2018.
MethodsEcological study of spatial analysis that aimed to assess the spatial and temporal dynamics of Hepatitis B occurrence in pregnant women, in the 27 Federative Units (FU) of Brazil and their respective municipalities, between 2009 and 2018.
All cases reported in the Notification Aggravation Information System (SINAN – Portuguese acronym) was defined as pregnant women with Hepatitis B, that is, all pregnant women that presented serological evidence of HBsAg in the prenatal period. In this system, the analyzed variables were: pregnant women, year of diagnosis/symptoms, FU of notification, municipality of notification, race, gender, age group, clinical form, etiological classification and source/mechanism of infection. The number of live births was obtained from the Live Birth Information System (SINASC – Portuguese acronym), available in the DATASUS (Portuguese acronym for "Department of Informatics of the Unified Health System") website.
The detection rate of Hepatitis B in pregnant women, variable of interest, was calculated from the number of confirmed Hepatitis B cases in pregnant women in a given year of notification and place of residence as the numerator and the number of live births, in the same year, in the same place as the denominator, multiplied by 1000.
17 There is no available standard, in the literature, of categorization for hepatitis B in pregnant women, thus, the detection rate in the analyzed period was categorized in multiples of 5.0/1.000 live births.
In order to verify the changes of HBV spatial standards, theme maps were elaborated into biennials (2009-2010, 2011-2012, 2013-2014, 2015-2016 and 2017-2018) for a better visualization and comprehension of detection rates of Hepatitis B in pregnant women by municipality with the QGIS 3.16.3 Odense software, based on data from the digital municipal mesh of Brazil provided by the Brazilian Institute of Geography and Statistics (IBGE – Portuguese acronym).
Crude rates were calculated to express the risk of Hepatitis B occurrence in pregnant women, although it is a rare event and susceptible to substantial variations, which lead to high instability. Therefore, the gross detection rates were softened by the Empiric Bayesian Method, which possesses lower variability and higher adequacy to the real risks of occurrence of the event in each geographic area analyzed. Local empirical Bayes estimates use information from other areas that compose the study region, in order to decrease the effect of random fluctuations of the attributes associated with risk, in which, observing the spatial correlation between neighbor areas, show as result softer maps, with more information and with more reliable rates and with better quality of the used indicators.
16In order to verify whether changes of standards and heterogeneity of spatial dependences of Hepatitis B cases in pregnant women per municipality in the years 2009-2018 occurred randomly in the space, or if the occurrence of cases in municipalities influences the occurrence in neighbor municipalities, the Geoda 1.18 software was used. For this spatial analysis, we opted to use Global Moran's Index (I) and the local indicators of spatial autocorrelation (LISA) in order to observe local data of 5570 municipalities in Brazil.
Global Moran's Indexes and LISA conducted spatial autocorrelation, which measures the relationship between observation and spatial proximity, considering that observations that are spatially next to each other possess similar values. For the Global Moran's calculation (I), a spatial autocorrelation is conducted, with covariance, from the product of the deviations in relation to the mean. This index tests if neighbor areas present higher similarity with regard to the studied indicator of what is expected randomly. For this, a spatial weight matrix of the first order adjacency type was used, since it is more adequate to capture spatiality of data, as it verifies the interaction horizontally, vertically and in diagonals. The result varies from -1 to +1, in which positive values (0 and +1) indicate autocorrelation, that is, the object tends to be similar to the values of its neighbors, whilst negative values (between 0 and -1) correspond to an inverse correlation, that is, the value of the attribute in a region is not dependent of values of this same variable in different areas. Global Moran's Index represents the autocorrelation considering only the first neighbor.
LISA produces a specific value for each municipality and allows the visualization of clusters of municipalities with values similar to the selected indicators. The clusters can be: correlations of the high-high type show municipalities with high rates of detection, surrounded by other municipalities also with high detection rates; those of low-low type, that indicates municipalities with low detection rates, surrounded by municipalities with low detection rates at the same indicator; those of the high-low type denote municipalities with high detection rate, surrounded by municipalities with low detection rates of this indicator; and those of low-high type describe municipalities of low detection rates surrounded by municipalities with high detection rates of the same indicator.
The trend analysis was executed for all states by means of the Prais-Winsten Generalized Regression model,
16 which is indicated for trend analyses, data that corrects the temporal autocorrelation of the residuals, starting from the ecological assumption that incidences may be influenced with each other in the years of the temporal series. The softening of rates for temporal series was executed by means of the moving average of third order. The analysis of the diagrams of incidence dispersion and of autocorrelation of residuals allowed identifying the behavior of the trend: stable (if
p>0.05); decreasing (if
p<0.05 and negative regression coefficient (β1)) and increasing (if
p<0.05 and positive regression coefficient (β1)). The coefficient of Prais-Winsten model regression and the annual variation of rates of detection of hepatitis B in pregnant women in the period (in percentage) were estimated using the formula: (-1+10-^b)x 100, since the regression uses the logarithm of rates (10^b). Stata 13 software was used for the trend analysis.
Since it is a research on databases and aggregated information, this study exempts the submission to Research and Ethics Committees.
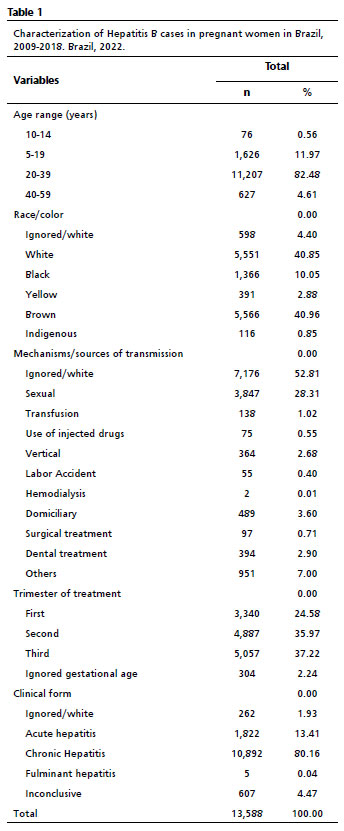
ResultsIn the period from 2009 to 2018, 13,588 pregnant women that had hepatitis B virus, mostly from the age group between 20 and 39 years (82.48%), brown skin (40.96%), infected sexually (28.31%), with diagnosis on the third trimester (37.22%) and classified as chronic carriers (80.16%) (Table 1).
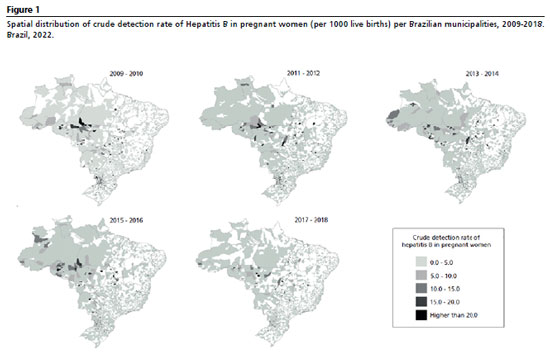
When analyzing crude rates of detection of Hepatitis B in pregnant women between 2009 and 2018, it was observed a concentration of cases in municipalities from states of the North region (Amazonas, Rondônia and Acre), Midwest region (Mato Grosso) and South region (Paraná and Santa Catarina). The 2009-2019 biennial obtained 11.13% (265) of municipalities that notified with detection rate ≥5.0 cases per 1 thousand live births (LB), with São Miguel da Boa vista standing out (68.96/1000 LB), in Santa Catarina. In 2011 and 2012, this percentage was 10.51% (264) municipalities and Araguaiana in Mato Grosso obtained the highest detection rate (68.18/1000 LB). In the years 2013 and 2014, 12.15% (306) of municipalities, of which Reserva do Cabaçal (80.00/1000 LB), in Mato Grosso, stood out. Therefore, in 2015 and 2016 9.27% municipalities (337), and São Geraldo da Piedade in Minas Gerais reached the highest rate (75/1000 LB). In the years 2017 and 2018, 8.91% municipalities (178), Porto Mauá in Rio Grande do Sul had the highest rate (Figure 1).
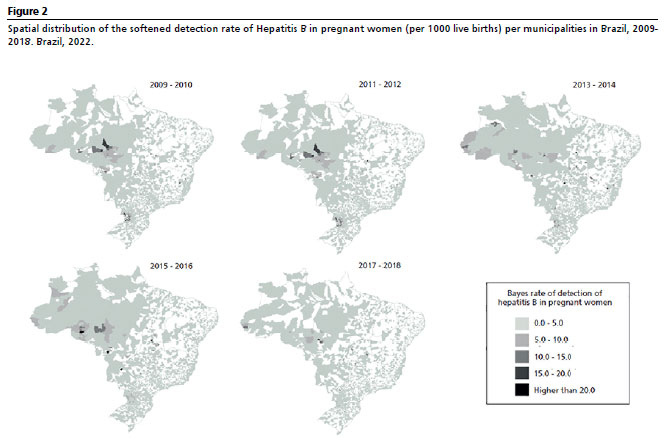
The softened rates, in all biennials, were lower than the crude rates. The 2013-2014 period also presented a higher number of municipalities with higher rates (Figure 2).
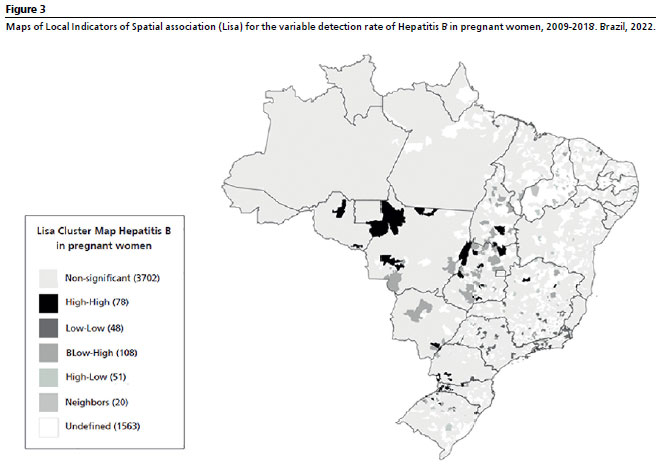
The Global Moran's Index (I) obtained for the period between 2009 and 2018 (I=0.056) presented a positive spatial association. Whilst in LISA, it was possible to observe that 78 municipalities were inserted in the high-high cluster, characterizing a strong spatial correlation to each other, due to higher detection rates of HBV in pregnant women. There was higher concentration of municipalities in the South region, reaching 51.28% (40 municipalities), but smaller niches were identified in other regions of the country, except Northeast Region (Figure 2).
The municipalities that belong to the low-low cluster, possess the mean of neighbors under the global mean, totaled 48, mostly located in the Southeast region (72.91%) (35 municipalities) and in sparse locations of the other regions, except the Midwest region (Figure 2).
The low-high and high-low clusters refer to the municipalities with the opposite behavior, thus are considered transitional municipalities. That is, in low-high are described the municipalities with low detection rate of neighbors above the global mean (108 municipalities). While the high-low are the municipalities that possess a high detection rate of neighbors below the global mean (51 municipalities) (Figure 2).
All municipalities enrolled in the 4 areas included in Lisa present significant values, with
p<0.05, and 3702 municipalities showed results without significance. The other 1583 were considered undefined since they did not have notification in the study period (Figure 3).
When assessing the trend of Hepatitis B detection rate in pregnant women in the states, it was verified that it was crescent in Maranhão (
p=0.004) and Pernambuco (
p=0.007) and descending in Mato Grosso (
p=0,012), Paraná (
p=0.031) and Santa Catarina (
p=0.008). In the North and Southeast regions and the other states of other regions, it was stable during the study period (Table 2).
DiscussionThe present study aimed to demonstrate the spatial distribution and trend of hepatitis B cases in pregnant women in Brazil, in the period between 2009 and 2018, and with this, verified locations that are historically endemic regarding Hepatitis B, with high rates of detection. Even more concerning are the states that demonstrated an increase in these indexes, which until heretofore were not considered of high endemicity for official statistics. Once it is a vaccine-preventable disease that has diagnosis tests for early detection available in the Unified Health System (SUS).
In spite of the relevance, the study demonstrated limitations related to the quality of data coming from the systems used, such as low completeness of fields and underreporting, which makes possible potential biases and compromise the reliability of performed actions, impairing the evaluation of executed measures and the management of surveillance activities. Still, in order to mitigate these limitations, the age group corresponding to the reproductive period of the woman was defined in the data selection, according to what was available in Sinan.
The age group of 20 to 39 years was predominant between pregnant women, similar to other national
18 and international studies.
19 In this phase, women are in the apex of sexual activity, consequently more susceptible to sex without protection, a fact that interfere in the infection by Hepatitis B, since in adults the way of transmission is frequently horizontal and of late detection. Thus, educational actions that seek to decrease the number of cases should be focused on this specific public.
7With regard to race, brown race was the more constant, as in the study carried out by Lobo
et al.,
20 in the city of Manaus. The people that self-declared themselves black or brown are responsible for the majority of consultations at public health services, being denominated
SUS-dependentes (SUS-dependent). Nevertheless, they constitute a population group with high social vulnerability, due to inequality of life conditions and in the access to healthcare of quality.
21With regard to the mechanism/source of infection, there was more frequency in the sexual type, according to the results of a study carried out in Acre.
7 This fact is justified by the confidence and intimacy acquired in stable relationships and unawareness about ways of transmission of HBV. With this, partners tend to limit or abolish the use of condoms, which may expose this group to different sexual transmitted diseases.
22Gestational age in the moment of diagnosis is a determinant factor for the implementation of treatment, in attempt of decreasing the viral load and consequently prevent vertical transmission.
12 Due to it, it should be done as early as possible for a better follow-up of the pregnant women,
7 although in the present study most diagnoses were performed in the second and third trimester. It is presupposed that the difficult access of female users to the service, distance of health units, late onset of prenatal consultations, delay in the schedule of essential tests requested by health professionals and the non-execution of rapid tests in prenatal consultations are unfavorable factors to the early diagnosis of infection in pregnant women.
22The classification as chronic carriers were preponderant in the study, similar to researches performed in Maranhão
23 and Santa Catarina.
24 The chronic type of Hepatitis B increases the risk of vertical transmission, and in case of immunoprophylaxis is not performed, the chance of becoming chronic, for the newborn, is about 90%, and because of this, in face of the presence of HBsAg, the pregnant women needs to be monitored in relation to the viral load, and the treatment should be implemented in order to interrupt the replication of the virus and promote the control of the inflammatory response.
10By means of the analysis of the spatial distribution, it was observed an increase of the number of municipalities with rates of detection ≥5.0 of cases per live birth until the 2013 and 2014 biennial, with a decrease after these years, similar to what is found in the literature.
25 This datum is directly linked to the improvement in the access to tests, which occurred via implementation of rapid tests in the prenatal routine, as preconized by the Stork Network. Consequently, there was an increase in the number of notifications, making it possible to follow up the positive cases after birth with better elucidation of vertical transmission of hepatitis B in the country.
24The 2017-2018 biennial presented lower number of municipalities with rates ≥5.0 cases per 1000 live births, and this may be associated with the decrease of viral hepatitis cases in the country in the years 2014 and 2015, reaching the lowest levels since 2010, with trend of decrease until the year 2018, demonstrating the effectiveness of public policies regarding the implementation of rapid tests and the expansion of the target public of Hepatitis B vaccine.
26 This reflects the decrease of the detection rate in pregnant women.
The municipalities that presented the highest detection rates in each analized biennial were São Miguel da Boa Vista (Santa Catarina), Araguaiana (Mato Grosso), Reserva do Cabaçal (Mato Grosso), São Geraldo da Piedade (Minas Gerais) and Porto Mauá (Rio Grande do Sul). In the high-high cluster were concentrated most of the municipalities of the South region and there were no municipalities of the Northeast region belonging to the cluster. When inserted in the cluster low-low, they were the majority of municipalities that are located in the Southeast region, without any from the Midwest region. This finding demonstrates the heterogeneous way of distribution of Hepatitis B cases in pregnant women.
The municipalities of the South region that were evidenced in the detection rates legitimate the majority of municipalities belonging to the high-high cluster. Since the region presents high incidences of HBV infection, higher than the national rate, occasioned by the immigration of Italians, Spanish, and Portuguese, mainly from the region of the European Mediterranean,
27 which may explain the behavior of Hepatitis B in pregnant women in the South region.
The Southeast region, even retaining the highest part of the Brazilian population, concentrated the majority of municipalities included in the low-low clusters, with only one municipality among those that were evidenced in the analyzed period. This finding may be associated with an expressive decrease of prevalence of transmission of disease in adults since the implementation of the universal HBV vaccine and the effectiveness of treatment, better quality of the epidemiological surveillance system, better access to health services, better life conditions and higher Human Development Indexes (HDI).
28The absence of municipalities of the Northeast region in the high-high cluster between the municipalities that were evidenced in the analyzed period may be justified by the fact that the region has less Hepatitis B cases, even in the general population as well as in pregnant women.
17 However, this may be explained by the lower social class of the majority of the infected population, impairing the access to health services for both diagnosis and treatment, emphasizing the urgency for health education campaigns. Also, it can be suspected that underreporting occurs, justifying the lower incidence rate.
26Even not presenting any municipality in the low-low cluster, the Midwest region obtained municipalities with highlighted detection rates in the observed period, justifying its intermediary endemicity.
17 Due to the migratory process that occurred in the 1970 and 1980 decades in the Amazonia region, after this a surge of HBV infection was identified due to bad hygiene conditions and intimate contact between immigrants. Besides, the population of gold miners influenced the increase of these rates, since they possessed several risk factors, such as multiple partners, sexual intercourse without protection, frequent visits to health units for traumatism, malaria, and the use of reused syringes and piercing objects.
27 Such factors, associated with the infection in reproductive age and consequent increase of vertical transmission risk.
With regard to the trend of detection rate in Maranhão and in Pernambuco, Maranhão occupied in 2020 the fourth place in number of hepatitis B cases in the Northeast,
17 but there is municipalities which present the HBsAg prevalence superior to the state mean, such that of 2.3% found in a study conducted with five municipalities from Maranhão in 2016.
29 With regard to pregnant women, a study conducted in 2007 in the capital of Maranhão observed that 0.9% were chronic carriers.
23 Pernambuco state, in the Northeast ranking, is ahead of Maranhão, which is in the third place.
17 The epidemiological bulletin of the state demonstrated an increasing trend on the number of cases and in the coefficient of incidence of Hepatitis B incidence in the period of 2000 to 2018, possibly due to the expressive reduction of the vaccine coverage, reaching 50.5% in 2020,
30 reverberating in the detection rates of pregnant women.
In Mato Grosso, Paraná and Santa Catarina the decrease present in the trend diverges from values found in the spatial analysis, since there were municipalities in these states with high rates. Notwithstanding, this decrease in the trend of cases, in the general population and in pregnant women, is certified by epidemiological bulletins in these locations.
17The stability in the trend of the other states may demonstrate an unsatisfactory result with regard to the Hepatitis B control, due to flaws in the screening, early diagnosis, effective treatment and prevention measures, which are broadly disseminated by the official departments of public health.
12The results of this study indicate the existence of geographical inequalities related to HBV infection in pregnant women, since in the South region it still present many cases, but with decrease trend, mainly in Paraná and Santa Catarina states, however there were two states, Maranhão and Pernambuco, which presented increase in the trend in the analyzed period.
The epidemiological profile of pregnant women, also identified in the present study, exposes the high risk of vertical transmission of hepatitis B virus, and consequently, neonatal complications that may occur. Thus, the detection practices during prenatal period contribute to identifying infected people and decrease the impact and dissemination of the virus in Brazilian municipalities. Finally, since it is pioneer in analyzing spatial distribution and temporal trend of hepatitis B cases in pregnant women, this study made it possible to glimpse the evolution of detection rates, as well as allowing the evaluation of a high number of pregnant women.
References1. World Health Organization (WHO). Hepatitis B. 2017. [
Internet]. [access in 2018 Abr 23]. Available from:
http://www.who.int/en/news-room/fact-sheets/detail/hepatitis-b2. Farias NSO, Holcman MM, Compri AP, Silva CRC, Figueiredo GM, Moreira RC,
et al. Ocorrência de hepatite B em gestantes e seguimento de crianças expostas no estado de São Paulo, em 2012. Epidemiol Serv Saúde. 2020; 29 (2): e2019443.
3. Souto FJD. Distribution of hepatitis B infection in Brazil: the epidemiological situation at the beginning of the 21 st century. Rev Soc Bras Med Trop. 2016; 49 (1): 11-23.
4. Duarte G, Pezzuto P, Barros TD, Mosimann Junior G, Martínez-Espinosa FE. Protocolo Brasileiro para Infecções Sexualmente Transmissíveis 2020: hepatites virais. Epidemiol Serv Saúde. 2021; 30 (spe 1): e2020834.
5. Shedain PR, Baral G, Sharma KR, Dhital S, Devkota MD. Prevalence and Mother-to-newborn Transmission of Hepatitis B Virus in Tertiary Care Hospital in Nepal. J Nepal Health Res Counc. 2019;17 (3): 278-84.
6. Alassan KS, Imorou RS, Sonombiti H, Salifou K, Ouendo EM. Séroprévalence et facteurs associés à l'hépatite virale B chez les gestantes à Parakou en République du Bénin [Seroprevalence and factors associated with viral hepatitis B among pregnant women in Parakou, Republic of Benin]. Pan Afr Med J. 2019; 33: 226.
7. Sanson MCG, Feitoza HAC, Saraceni V, Koifman RJ, Bessa ARS. Prevalência e perfil epidemiológico da Hepatite B em gestantes: um estudo populacional em uma cidade da Amazônia Ocidental brasileira, no período de 2007 a 2015. Rev Bras Saúde Mater. Infant. 2018; 18 (4): 711-21.
8. Vargas L, Bastos F, Guimarães A, Amaral S, Fausto T, Arriaga M,
et al. Seroprevalence and factors associated with Human Immunodeficiency virus, Human T lymphotropic virus and Hepatitis B/C infections in parturient women of Salvador - Bahia, Brazil. Braz J Infect Dis. 2020; 24 (4): 279-87.
9. Barros MMO, Ronchini KROM, Soares RLS. Hepatitis B and C in pregnant women attended by a prenatal program in an universitary hospital in Rio de Janeiro, Brazil: retrospective study of seroprevalence screening. Arq Gastroenterol. 2018; 55 (3): 267-73.
10. Silva TGQ, Nakasse TSL, Corrêa MCB, Moretto IM, Geraldo ALY, Ramos OO,
et al. Atualização em hepatite b: revisão bibliográfica. J Dev. 2020; 6 (12): 97930-46.
11. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância das Doenças Transmissíveis. Manual de Normas e Procedimentos para Vacinação. Brasília (DF): Ministério da Saúde; 2014. [access in 2022 Nov 22]. Available from
https://bvsms.saude.gov.br/bvs/publicacoes/manual_procedimentos_vacinacao.pdf12. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Doenças de Condições Crônicas e Infecções Sexualmente Transmissíveis. Protocolo Clínico e Diretrizes Terapêuticas para Prevenção da Transmissão Vertical do HIV, Sífilis e Hepatites Virais. Brasília (DF): Ministério da Saúde; 2019. [access in 2022 Nov 22]. Available from:
https://prceu.usp.br/wp-content/uploads/2020/05/miolo_pcdt_tv_08_2019.pdf13. Freire JO, Schuch JB, Miranda MF, Roglio VS, Tanajura H, Victa AGLB,
et al. Prevalência de HIV, Sífilis, Hepatites B e C em gestantes de uma maternidade de Salvador. Rev Bras Saúde Matern Infant. 2021; 21: 945-53.
14. Uchôa NTM, Rêgo RCS, Azevedo PVM, Matos Rocha TJ, Santos EO, Wanderley F dos S. Seroprevalence of infection by syphilis, HIV 1/2, toxoplasmosis, hepatitis B and hepatitis C in pregnant women assisted by the health service of Penedo-AL. RSD. 2022; 11 (5): e0811521158.
15. Silva TPR, Gomes CS, Carmo AS, Mendes LL, Rezende EM, Velasquez-Melendez G,
et al. Análise espacial da vacinação contra hepatite B em gestantes em área urbana no Brasil. Ciência Saúde Colet. 2021; 26 (3): 1173-82.
16. Falavina LP, Lentsck MH, Mathias TAF. Tendência e distribuição espacial de doenças infecciosas em gestantes no estado do Paraná-Brasil. Rev Latino-Ame Enferm. 2019; 27.
17. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Boletim Epidemiológico. Hepatites Virais; 2021. Brasília (DF): Ministério da Saúde; 2021. [access in 2022 Nov 22]. Available from:
https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/especiais/2021/boletim-epidemiologico-de-hepatite-2021.pdf18. Gruhn EG, Marino JB, Alves MG, Piza SMG, Alegre-Maller ACP. Análise epidemiológica e manejo de gestantes portadoras de hepatite B acompanhadas no centro especializado de doenças infecto parasitárias da cidade de Cascavel (PR). Rev Thêm Sci. 2020; 10 (1E): 131-41.
19. Kinfe H, Sendo EG, Gebremedhin KB. Prevalence of Hepatitis B Virus Infection and Factors Associated with Hepatitis B Virus Infection Among Pregnant Women Presented to Antenatal Care Clinics at Adigrat General Hospital in Northern Ethiopia. Int J Womens Health. 2021; 13: 119-27.
20. Lobo L, Costa P, Abreu G, Oliveira N, Medeiros M, Sachett J,
et al. Characterization of the rapid test for HIV/AIDS, syphilis and viral hepatitis in pregnant women. Mundo Saúde. 2019; 43: 281-305.
21. Silva HKA, Rocha MA, Rebouças ES, Santos RV, Soares SCR, Moreira MH,
et al. Risk factors associated with persistence of gestational syphilis: an integrative review. RSD. 2022; 11 (6): e31111629203.
22. Tenorio LV, Azevedo EB de, Barbosa JCG, Lima MKS, Pereira MMBS, Barbosa HCV. Factors that hard the early diagnosis of syphilis in pregnancy. RSD. 2020; 9 (9): e377997225.
23. Souza MT, Pinho TL, Santos MD, Santos AD, Monteiro VL, Fonsêca LM,
et al. Prevalence of hepatitis B among pregnant women assisted at the public maternity hospitals of São Luís, Maranhão, Brazil. Braz J Infect Dis. 2012; 16 (6): 517-20.
24. Kupek E, Oliveira JF. Transmissão vertical do HIV, da sífilis e da hepatite B no município de maior incidência de AIDS no Brasil: um estudo populacional no período de 2002 a 2007. Rev Bras Epidemiol. 2012; 15: 478-87.
25. Mello RF, Mendes SS, Sousa OMS, Martins NG, Cardoso LBA. Revisão sobre a epidemiologia da hepatite b no estado do Rio de Janeiro. Cad Medicina-UNIFESO. 2019; 2 (1).
26. Sousa ARA, Alves AAC, Mamede AL, Maciel CNAT, Marques DMS, Talassi GG,
et al. Estudo Epidemiológico sobre Hepatite na Região Nordeste entre 2010 a 2018 através de dados do DATASUS. Rev Elet Acervo Med. 2021; 1 (2): e9391.
27. Santos ECC, Pereira MA. Situação epidemiológica brasileira sobre as hepatites B e C no período de 2000 a 2016. Braz J Health Rev. 2021; 4 (5): 18612-29.
28. Melo MC, Jacob LMS, Cabral ERM, Rolim ACA. Variação anual percentual de doses vacinais para hepatite B na região Sudeste do Brasil. Rev Prev Infec Saúde. 2018; 4: 7028.
29. Nunes JDC, Silva DLFD, Fonseca LMB, Felipe IMA, Ferreira BR, Santana RC,
et al. Unexpected findings of hepatitis B and delta infection in northeastern Brazil: a public health alert. Ann Hepatol. 2021; 22: 100272.
30. Secretaria Estadual de Saúde. Pernambuco. Diretoria Geral de Vigilância de Doenças Transmissíveis. Boletim Hepatites Virais. 2021. [access in 2022 Nov 22]. Available from:
http://portal.saude.pe.gov.br/sites/portal.saude.pe.gov.br/files/informe_hepatites_pe_2021.pdfAuthor's contribution: Albuquerque IC: data collection and analysis and writing, Soeiro VMS: data analysis and writing; Lima RA: writing and review; Ferreira ASP: writing and final review.
All authors approved the final version of the article and declared no conflicts of interest.
Received on March 18, 2023
Final version presented on July 27, 2023
Approved on August 7, 2023
Associated Editor: Melânia Amorim


 ; Vanessa Moreira da Silva Soeiro2
; Vanessa Moreira da Silva Soeiro2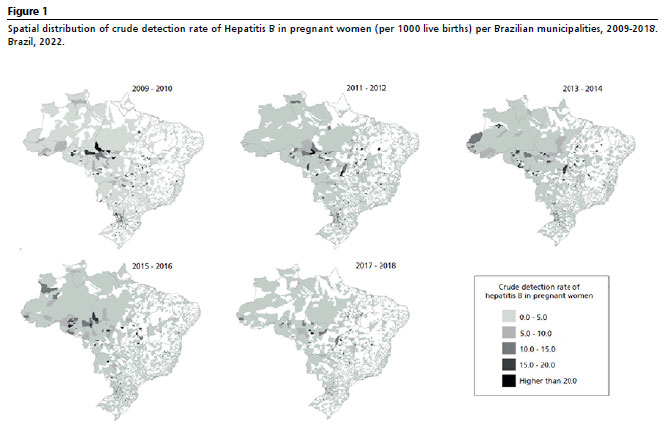






 Ler em português
Ler em português