ABSTRACT
OBJECTIVES: to evaluate the effect of oropharyngeal colostrum immunotherapy on the length of hospital stay in preterm newborns with very low birth weight.
METHODS: interventional ambispective study, which consisted of eight daily administrations of 0.2 ml (four drops) of colostrum, totaling up to 56 syringes (for up to seven days). The control was historic. The main independent variable: length of hospital stay (days). Survival analysis was performed using the Kaplan-Meier Method and the survival effect was estimated - Log Rank Test (Mantel-Cox) and Breslow Test (Generalized Wilcoxon). A significance level of 5% was adopted.
RESULTS: of the 109 mother/child pairs, 56 were part of the treatment and 53 were part of the control group. There was no association between oropharyngeal colostrum immunotherapy and length of stay for preterm newborns with very low birth weight in the general sample. However, after stratification, a shorter hospital stay (42 versus 51 days, HR= 1.78, CI95%=1.02-3.09, p=0.04) was demonstrated among premature infants with ≥28 gestational weeks undergoing oropharyngeal colostrum immunotherapy.
CONCLUSIONS: we found an association between oropharyngeal colostrum immunotherapy and shorter median length of hospital stay in the subgroup of premature infants ≥ 28 weeks of gestational age, but we did not find significant differences in those <28 weeks.
Keywords:
Immunotherapy, Colostrum, Infant premature, Clinical trial
RESUMO
OBJETIVOS: avaliar o efeito da imunoterapia orofaríngea de colostro no tempo de internamento hospitalar de recém-nascidos pré-termos de muito baixo peso.
MÉTODOS: estudo de intervenção, ambispectivo, que consistiu em oito administrações diárias de 0,2 ml (quatro gotas) de colostro, totalizando até 56 seringas (por até sete dias). O controle foi histórico. A variável independente principal: tempo de permanência hospitalar (dias). Realizada análise de sobrevivência pelo Método de Kaplan-Meier e estimado o efeito da sobrevida - Teste de Log Rank (Mantel-Cox) e Teste de Breslow (Wilcoxon Generalizado). Adotou-se o nível de significância de 5%.
RESULTADOS: das 109 duplas mães/filho, 56 fizeram parte da análise do grupo tratamento e 53 do controle. Não houve associação entre imunoterapia orofaríngea de colostro e tempo de internamento de recém-nascidos pré-termos de muito baixo peso na amostra geral. Após estratificação demonstrou-se menor tempo de permanência hospitalar (43 versus 51 dias, HR=1,78, IC95%= 1,02-3,09, p=0,04) entre os prematuros com ≥28 semanas gestacionais submetidos a imunoterapia orofaríngea de colostro.
CONCLUSÕES: encontrou-se associação entre imunoterapia orofaríngea de colostro e menor mediana de tempo de internamento hospitalar no subgrupo de prematuros ≥ 28 semanas de idade gestacional, porém não foram encontradas diferenças significativas naqueles < 28 semanas.
Palavras-chave:
Imunoterapia, Colostro, Recém-nascido prematuro, Ensaio clínico
IntroductionPreterm newborns (PTNB) are those who were born before 37 weeks of pregnancy.
1 Although the survival rate of PTNB has been improving in the last decades due to the advances in neonatal intensive care, there are still important challenges to be overcame, such as the reduction of neonatal mortality due to necrotizing enterocolitis and sepsis, as well as the limitation with the nutrition of preterm newborns.
1 Characteristics that are inherent to preterm birth itself contribute to these vulnerabilities, such as the immaturity of the immune and digestive systems, which postpone the length of hospital stay.
In order to overcome these challenges, it has been suggested, mainly for extreme low weight (ELW) PTNBs, weighing less or equal than 1500g, the oropharyngeal colostrum immunotherapy (OCI), by means of the offer of raw colostrum from their mothers. A safe, inexpensive, viable and well-tolerated strategy,
2,3, which provides immunostimulatory effects due to the exposition of PTNBs to bioactive immunological factors present in colostrum, such as the cytokines, oligosaccharides, secretory immunoglobulin A, lactoferrin and antioxidants.
2,4 Besides, the gastrointestinal trophic factors present in breast milk function on immature gastrointestinal cells, improving the tolerance to food consumption,
5 reducing the time necessary to reach full enteral nutrition
3,6-10 and favoring adequate weight gain.
7;9;11Several researchers evaluated the immunomodulatory benefits of OCI regarding different outcomes, such as lower length of oxygen therapy,
5 prevention of necrotizing enterocolitis,
3,6 sepsis,
6,12 nosocomial infection
13 and pneumonia associated with invasivemechanical ventilation,
3,5 among others. These pathologies, when present, increase the exposure of the preterm newborns to the hospital microbiome, which is composed by pathogenic bacteria that worsen their clinical conditions and lead to higher length of hospital stay.
The association between the use of OCI and time of hospitalization was already researched in some studies; however, the outcomes were largely divergent. With regard to clinical trials, four demonstrated favorable outcome for the intervention group
5,7,14,15 and eight did not observe this association.
6,8,9,12,16-19 Meta-analysis researches, published between 2020 and 2023, found out that hospitalization was significantly reduced in the treatment group.
11,20,21 however, previous studies have demonstrated favorable outcome for the control group
22 or did not observe significant difference.
2,3,10,13The divergence between results reinforce the need for further investigations regarding the effect of OCI in the length of hospital stay of preterm newborns, a relevant subject for public health. In this regard, the present study aimed to assess the effect of oropharyngeal colostrum immunotherapy in the length of hospitalization of preterm newborns with extreme low weight.
MethodsThis manuscript is presented according to the guidelines of CONSORT 2010.
23 It is an ambispective interventional study, with an intervention group composed by PTNB-ELW hospitalized in a NICU of a public hospital, located in a large city of Brazilian Northeast. The onset of the intervention occurred in up to 72 hours of life. Further details regarding the methodology is available in a protocol published in 2020 by Cruz Martins
et al.
24The treatment group with OCI was composed by PTNB-ELW that were clinically stable in the three hours that preceded the onset of therapy, considering: heart rate, temperature, respiratory frequency, blood pressure and oxygen saturation. The maternal exclusion criteria were: relate of drug abuse, mental disease, multiparity (triplets and more), pathologies that contraindicate breast-feeding; and those referring to the PTNB-ELW: use of vasopressors > 10mcg/Kg/min, indication of immediate surgical intervention, presence of syndromes or malformations. Early neonatal deaths and the use of doses of treatment under 75% of the planned doses, according to protocol
24, were considered as loss of follow-up.
The treatment group was recruited between October 2018 and August 2020. The control group established was a historic one, composed of PTNB-ELW who were born in the same maternity hospital and were hospitalized in the neonatal intensive and intermediate care units between May 2015 and November 2016. This group did not use OCI, since that was a period that preceded the implementation of this protocol in the hospital, which occurred in 2018. In turn, data collection was performed by means of the consultation of medical records archived in the Service of Medical Files and Statistics of the institution. The allocation rate of the intervention group was 1:1.
The intervention consisted in the use of colostrum aiming immunological supplementation of the PTNB-ELW, with medical prescription. The procedure consisted in daily administration of 0.2ml (drops) of colostrum, dripped in seconds on the oropharyngeal mucosa, totaling up to 56 syringes. When the PTNB-ELW used more than 75% of the planned doses, the therapy was considered complete.
24 The vital conditions of the PTNB-ELW were monitored during the intervention. In case of alteration of criteria of clinical stability, in the moment of OCI, the offer would be immediately interrupted and retaken after clinical stabilization.
The main dependent variable (exposition) was the OCI. The main independent variable (outcome) was the length of hospitalization, measured in days. In both groups, sociodemographic maternal characteristics where researched: age (<18 years, ≥18 years), self-declared race/color (black/non-black), paid work (no, yes), location of residence (rural, urban); prenatal and birth variables: gestational age (<28 weeks, ≥28 weeks), primiparity (yes, no), twinning (no, yes), number of prenatal consultations (<6 consultations, ≥6 consultations), type of delivery (surgical, vaginal), infection during pregnancy (yes, no), use of prenatal corticoid (yes, no), time of amniotic membrane rupture in relation to delivery (≥24 hours, > 24 hours), and variables referring to the PTNB-ELW: sex (female, male), birth weight (≥ 1000 grams, >1000 grams), Apgar score at 5
th minute (≥ 5 minutes, >5 minute), bronchopulmonary dysplasia diagnosis (yes, no) and hyaline membrane disease - respiratory distress syndrome (yes, no).
The OCI protocol had a sample size calculation of 350 participants.
24 For the current outcome – time of hospitalization, since it is a finite population, without reposition and with a mean of admission in the neonatal unit of 68 PTNB-ELW for the last five years (136 individuals), it was necessary to readjust the sample calculation by means of the finite population correction factor.
25 Thus, the estimate of the sample size for this study was of 76 participants. We opted for an addition of 15% for eventual losses, totaling 88 participants, 44 in each group.
Initially, data doubled-blind entered in the IBM-SPSS software (version 24.0, Chigago, IL, USA, serial number:10101181103), independently by different previously trained health professionals, with further comparison of data from both databases with the use of the EPIDATA software. Diverging results were corrected, and validated data composed a single database. The STATA 15.1 software (serial number: 401506208261) was used to perform data analysis.
Descriptive analysis of variables of the two groups (intervention and control) was performed for the entirety of newborns and for groups stratified into preterm <28 gestational weeks and ≥28 gestational weeks. The normality of continuous variables was verified by means of the Shapiro-Francia test. In order to verify differences between the groups, in these variables, the Student's t-test or Mann-Whitney U test were applied. The categorical co-variables were assessed by means of the chi-square Test or Fisher's exact Test. A significance level of 5% was adopted.
Finally, the Kaplan-Meier Method was applied in order to assess the dimension of the survival effect in the hospitalization time between the comparison groups. The effect of survival was estimated in the beginning of the curve by means of the Log Rank Test (Mantel-Cox), and from the middle to the end with the Breslow Test (General Wilcoxon), with a significance level of 5%. In addition, the hazard ratio (HR) of the time of hospitalization was calculated, followed by its confidence interval of 95% (CI95%).
The losses were monitored during the follow-up of the research, and the impact of the losses were assessed with the sensibility analysis, demonstrating that the lost PTNBs had the same base characteristics than those who remained in the study. None of the PTNB-ELW treated with OCI demonstrated adverse effects during or after the administration of colostrum doses, according to registration in the medical records.
The study was conducted within ethical standards, approved by the Research and Ethics Committee of the State University of Feira de Santana under CAAE number 93056218.0.0000.0053, and is registered in the Brazilian Clinical Trial Registry (ReBEC – Portuguese acronym) under registry RBR-2cyp7c e UTN U1111-1222-0598.
Results145 mother/child pairs were eligible for the study, however, four pairs did not meet the inclusion criteria and one presented an incomplete record, being excluded.140 mother/child pairs participated in the study, of these, 109 completed the follow-up and 31 were considered losses, since two had discontinued intervention and 29 had early neonatal death (Figure 1).
Of the 109 mother/child pairs of the study, 56 participated in the treatment group analysis, and 53, in the control group (Figure 1). For the newborns from the treatment group, 2605 syringes containing colostrum were administered. It is worth highlighting that 46% (26/56) of the participants followed initiated immunotherapy in the first 24 hours of life and 73% (41/56) in up to 48 hours of life.
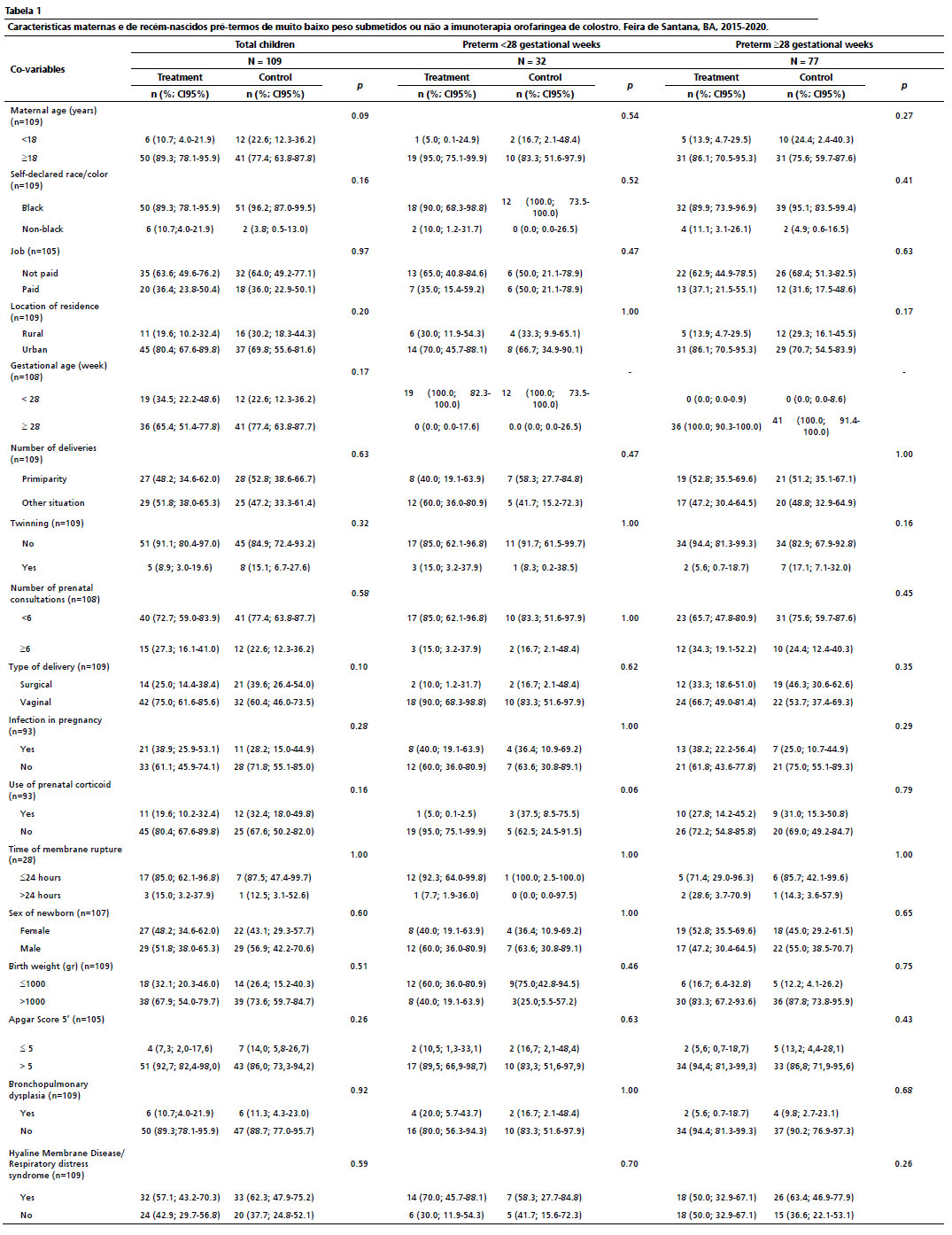
The maternal and neonatal characteristics were described in Table 1, according to control and treatment groups. It was noted that there were no significant differences of these characteristics between the groups. The length of hospitalization in the treatment and control group was (44 versus 49 days, HR= 1.23, CI95%= 0.83-2.25,
p=0.21). However, when the analysis stratified per subgroups was performed (<28 gestational weeks and ≥28 gestational weeks), we found statistically significant difference, with lower hospital stay (43 versus 51 days, HR= 1.78 CI95%= 1.02-3.09,
p= 0.04) between preterm newborns with ≥28 gestational weeks submitted to OCI. The preterm newborns ≥28 gestational weeks did not obtain statistical significance (62 versus 45 days, HR= 2.19, CI95%= 0.46-10.35,
p= 0.32) with regard to the length of hospitalization.
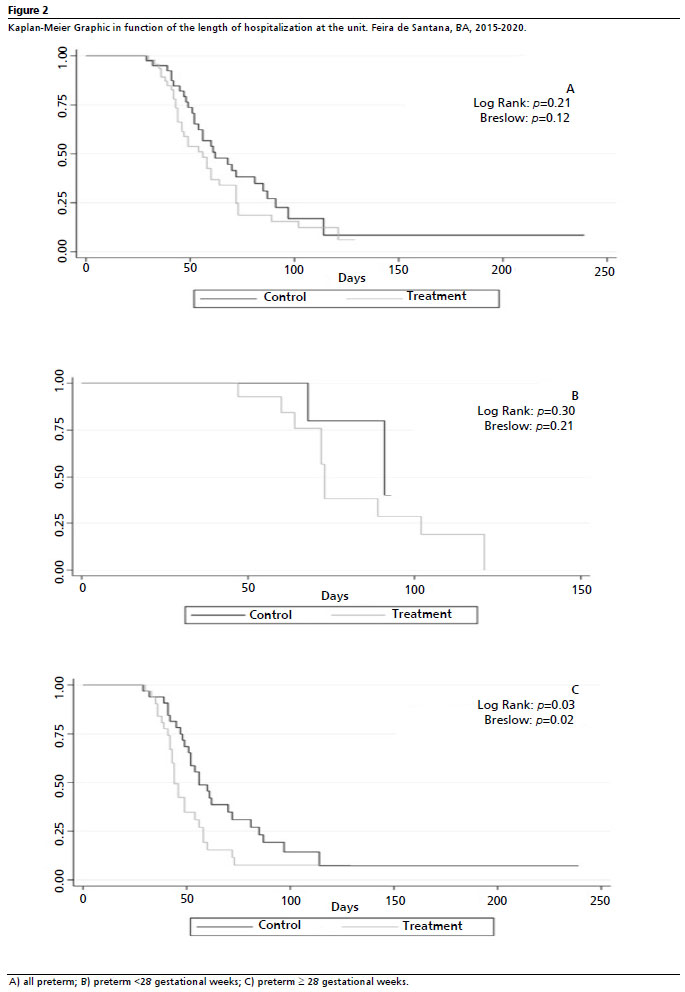
Figure 2 presents the comparison of the survival curves of length of hospitalization of the treatment and control group (A), of preterm newborns <28 gestational weeks (B) and preterm newborns ≥28 gestational weeks (C). The survival curves did not present significant differences with
p= 0.21 and 0.12 in the general sample according to the Log Rank test (Mantel-Cox) and Breslow (General Wilcoxon) test, respectively. However, after stratification, data corroborated the association between OCI and length of hospitalization of PTNB-ELW for those ≥28 gestational weeks (
p= 0.03 and
p=0.02) (Figure 2).
DiscussionIn the present study, we foundan association between OCI and a smaller median of length of hospitalization in the group of preterm newborns ≥ 28 gestational age weeks. This finding is in line with the result of the last published meta-analyses,
11,20,21 which assessed only controlled clinical trials
5,6,8,12,14,15,17-19 and reported lower length of hospitalization in the group of preterm newborns <34 and ≥32 weeks of gestational age in OCI, respectively.
11,20,21 However, the result that we found differs from other meta-analysis
22 that had favorable outcomes for the control group.
On the other hand, when assessing the effect of OCI in newborns that are extremely preterm (≥28 weeks) we did not find significant differences between the groups, a finding reported in other studies conducted with preterm newborns,
2,3,10,13 although without stratification by gestational age. The gestational age between the several conducted studies may be a factor that contributes to the differences between the results. Clinical trials that assessed newborns with gestational age between 26 and 31 weeks,
18,19 <28weeks,
8,12 as well as PTNB with birth weight under 1000g
6,9 did not find association between OCI and length of hospitalization as well.
A systematic review from the year 2023 assessed 23 studies published with data from eleven countries, among these South Africa (1), Canada (1), China (4), United States of America (8), Eritrea (1), Ethiopia (1), India (2), Iran (1), Israel (1), Poland (1) and Turkey (2) and identified the gestational age, among other risk factors for higher stay of preterm newborns in NICUs, which are: birth weight, sepsis, necrotizing enterocolitis, bronchopulmonary dysplasia and retinopathy of prematurity; and reassured the need for further studies that investigate factors that affect the duration of hospitalization of PTNBs.
26 The challenge to this risk factors may represent an improvement in the survival of preterm newborns, with impacts in the reduction of length of hospitalization, and consequently public costs with health focused on this segment of the population.
In this way, being aware of the biological plausibility, it is expected that OCI favors higher protection to the most immature PTNB-ELW, since there is a direct relationship between prematurity and physiological and immunological immaturity, which generate physiological instabilities, such as the inability of exclusive oral nutrition, inability of maintaining the normal body temperature and of maintaining stability of cardiorespiratory function.
27 However, it is necessary to consider that the lower the weight and gestational age at birth, the higher the time necessary to achieve these competences, which naturally imply in diseases of the preterm newborn due to comorbidities,
27 need for invasive therapies
28 and higher hospitalization time. These parameters may have contributed to the lower protective effect of OCI in the group of preterm newborns with lower gestational age.
Besides the gestational age, other factors may help to justify the lack of consensus between the published studies, such as variability of assistance conducts,
16,29 administration of colostrum with different techniques, volumes, frequency, time of onset and duration of exposition,
5-7,13,18,29 access to milk banks, hospital routines and conducts favorable to breastfeeding,
7,17,18 different study and analyses designs,
16 sample sizes and power of study,
7,18,29 different basal characteristics between the treatment and control groups and loss of follow up.
17The main merit of the present study was to draw attention to the importance of considering the gestational age between preterm newborns, when assessing the association of OCI and length of hospitalization. On the other hand, we draw the attention to some limitations, such as the small sample size, and the impossibility of randomization due to an obligation defined by the research and ethics committee. In an attempt to minimize the effects of non-randomization, due to the use of historical control, sensibility analysis
30 and statistical method were used in order to identify an eventual variability of base characteristics of participants and control possible biases.
Lastly, we conclude that a reduction of length of hospitalization of preterm newborns ≥28 gestational weeks with extremely low birth weight treated with oropharyngeal colostrum immunotherapy has occurred. The findings suggest the need for considering gestational age in further researches, as well as multicentric studies, with enough power to define the clinical effectiveness of OCI, an important measure that contributes with the reduction of health costs, lower risk of sequels in medium and long term, with possible benefits for families and society.
References1. World Health Organization (WHO). Born too soon: decade of action on preterm birth. [Internet]. Geneva: WHO; 2023. [access in 2023 Nov 27]. Available from:
https://www.who.int/publications/i/item/97892400738902. Panchal H, Athalye-Jape G, Patole S. Oropharyngeal colostrum for preterm infants: a systematic review and meta-analysis. Adv Nutr. 2019 Nov; 10 (6): 1152-62.
3. Ma A, Yang J, Li Y, Zhang X, Kang Y. Oropharyngeal colostrum therapy reduces the incidence of ventilator-associated pneumonia in very low birth weight infants: a systematic review and meta-analysis. Pediatr Res. 2020 Jan; 89 (1): 54-62.
4. Martín-Álvarez E, Diaz-Castro J, Peña-Caballero M, Serrano-López L, Moreno-Fernández J, Sánchez-Martínez B, et al. Oropharyngeal Colostrum Positively Modulates the Inflammatory Response in Preterm Neonates. Nutrients. 2020 Feb; 12 (2): 413.
5. Abd-Elgawad M, Eldegla H, Khashaba M, Nasef N. Oropharyngeal administration of mother's milk prior to gavage feeding in preterm infants: A pilot randomized control trial. J Parenter Enteral Nutr. 2020 Jan; 44 (1): 92-104.
6. OuYang X, Yang CY, Xiu, WL, Hu YH, Mei SS, Lin Q. Oropharyngeal administration of colostrum for preventing necrotizing enterocolitis and late-onset sepsis in preterm infants with gestational age ≤ 32 weeks: a pilot single-center randomized controlled trial. Int Breastfeed J. 2021 Aug; 16 (1): 59.
7. Romero-Maldonado S, Soriano-Becerril DM, García-May PK, Reyes-Muñoz E, Muñoz-Ortíz EG, Carrera-Muiños S, et al. Effect of Oropharyngeal Administration of Colostrum in Premature Newborns ≤32 Weeks of Gestation on the Immune Response and Neonatal Morbidity: A Double-Blind Randomized Clinical Trial. Front Pediatr. 2022 Jul; 10: 891491.
8. Rodriguez NA, Groer MW, Zeller JM, Engstrom, Fogg L, Du H, et al. A randomized controlled trial of the oropharyngeal administration of mother's colostrum to extremely low birth weight infants in the first days of life. Neonatal Intensive Care. 2011; 24 (4): 31-5.
9. Seigel JK, Smith PB, Ashley PL, Cotten CM, Herbert CC, King BA, et al. Early administration of oropharyngeal colostrum to extremely low birth weight infants. Breastfeed Med. 2013 Dec; 8 (6): 491-5.
10. Nasuf AWA, Ojha S, Dorling J. Oropharyngeal colostrum in preventing mortality and morbidity in preterm infants. Cochrane Database Syst Rev. 2018 Sep; 9 (9): CD011921.
11. Tao J, Mao J, Yang J, Su Y. Effects of oropharyngeal administration of colostrum on the incidence of necrotizing enterocolitis, late-onset sepsis, and death in preterm infants: a meta-analysis of RCTs. Eur J Clin Nutr. 2020 Aug; 74 (8): 1122-31.
12. Lee J, Kim H, Jung YH, Choi KY, Shin SH, Kim E, et al. Oropharyngeal colostrum administration in extremely premature infants: An RCT. Pediatrics. 2015 Feb; 135 (2): e357-66.
13. Tang R, Yao XY, Shi LP. The Effects of Colostrum on Gastrointestinal Function and Related Diseases in Premature Infants: A Comprehensive Meta-Analysis of Randomized Controlled Trials. Yangtze Medicine. 2018 Dec; 2 (4): 271-80.
14. Romano-Keeler J, Azcarate-Peril MA, Weitkamp J-H, Slaughter JC, McDonald WH, Meng S, et al. Oral colostrum priming shortens hospitalization without changing the immunomicrobial milieu. J Perinatol. 2017 Jan; 37 (1): 36-41.
15. Sharma D, Kaur A, Farahbakhsh N, Agarwal S. Role of oropharyngeal administration of colostrum in very low birth weight infants for reducing necrotizing enterocolitis: A randomized controlled trial. Am J Perinatol. 2020 Jun; 37 (7): 716-21.
16. Thibeau S, Boudreaux C. Exploring the use of mothers' own milk as oral care for mechanically ventilated very low-birth-weight preterm infants. Adv Neonatal Care. 2013 Jun; 13 (3): 190-7.
17. Ferreira DMLM, Oliveira AMM, Leves DV, Bem EB, Fatureto GG, Navarro NF, et al. Randomized controlled trial of oropharyngeal colostrum administration in very-low-birth-weight preterm infants. J Pediatr Gastroenterol Nutr. 2019 Jul; 69 (1): 126-30.
18. Aggarwal R, Plakkal N, Bhat V. Does oropharyngeal administration of colostrum reduce morbidity and mortality in very preterm infants? A randomised parallel-group controlled trial. J Paediatr Child Health. 2021 Sep; 57 (9): 1467-72.
19. Sudeep KC, Kumar J, Ray S, Dutta S, Aggarwal R, Kumar P. Oral Application of Colostrum and Mother's Own Milk in Preterm Infants-A Randomized, Controlled Trial. Indian J Pediatr. 2022 Jun; 89 (6): 579-86.
20. Cai M, Lin L, Peng Y, Chen L, Lin Y. Effect of Breast Milk Oral Care on Mechanically Ventilated Preterm Infants: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front Pediatr. 2022 Jul; 10: 899193.
21. Peng B, Yu L, Qian J, Zheng B, Zhang Y, Zhu C. Oral Application of Mother's Own Milk for Reducing Necrotizing Enterocolitis in Preterm Infants: An Updated Meta-Analysis of RCTs. Evid Based Complement Alternat Med. 2023 Apr; 2023: 7378064.
22. Garg BD, Balasubramanian H, Kabra NS, Bansal A. Effect of oropharyngeal colostrum therapy in the prevention of necrotising enterocolitis among very low birthweight neonates: A meta-analysis of randomised controlled trials. J Hum Nutr Diet. 2018 Oct; 31 (5): 612-24.
23. Schulz KF, Altman DG, Moher D. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. BMJ Med. 2010; 8: 18.
24. Cruz Martins C, Ramos MSX, Amaral MVC, Costa JSP, Cerqueira ES, Vieira TO, et al. Colostrum oropharyngeal immunotherapy for very low birth weight preterm infants: protocol of an intervention study. BMC Pediatrics. 2020 Aug; 20 (1): 371.
25. Ramachandran KM, Tsokos CP. Mathematical Statistics with Applications. Índia: Elsevier; 2012.
26. Fu M, Song W, Yu G, Yu Y, Yang Q. Risk factors for length of NICU stay of newborns: a systematic review. Front Pediatr. 2023 Mar; 11: 1121406.
27. Ferreira DMLM, Abdallah VOS, Camelo Júnior JS. Colostroterapia em recém-nascidos pré-termo: uma visão atual. In: Sociedade Brasileira de Pediatria; Procianoy RS, Leone CR, (org). PRORN Programa de Atualização em Neonatologia: Ciclo 18. Porto Alegre: Artmed Panamericana; 2020. p. 33-56. (Sistema de Educação Continuada a Distância, v. 1).
28. Montagne P, Cuillière ML, Molé C, Béné MC, Faure G. Immunological and nutritional composition of human milk in relation to prematurity and mother's parity during the first 2 weeks of lactation. J Pediatr Gastroenterol Nutr. 1999 Jul; 29 (1): 75-80.
29. Nascimento MBR, Floriano ML, Giacomet MDM, Duarte MM, Reis MAM. Estudo exploratório sobre a utilização da Colostroterapia em Unidade Neonatal de uma maternidade brasileira. Saúde Pesq. 2020 Jun; 13 (2): 389-97.
30. Ghadessi M, Tang R, Zhou J, Liu R, Wang C, Toyoizumi K, et al. A roadmap to using historical controls in clinical trials - by Drug Information Association Adaptive Design Scientific Working Group (DIA-ADSWG). Orphanet J Rare Dis 2020 Mar; 15 (1): 69.
Author's contribution: CruzMartins C, Ramos MSX, Lyrio AO, Costa MGR: conceptualization, search for funding, data analysis and interpretation, writing and review of the version to be published. Veira TO and Cruz SS: study design and critical review of the version. Vieira GO: researcher responsible for the study, working from the conceptualization until the writing and review of the final version.
All authors approved the final version of the article and declare no conflicts of interest.
Received on March 24, 2023
Final version presented on January 21, 2024
Approved on February 2, 2024
Associated Editor: Karla Bomfim


 ; Camilla da Cruz Martins2
; Camilla da Cruz Martins2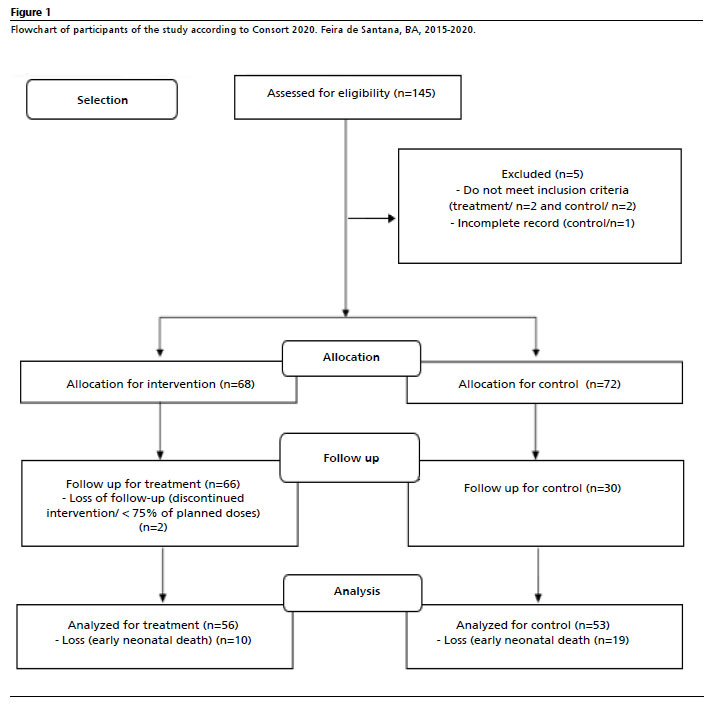






 Ler em português
Ler em português