ABSTRACT
OBJECTIVES: to evaluate the association between breastfeeding and Autism Spectrum Disorder (ASD) in children and adolescents.
METHODS: this is a case-control study carried out in the north of the state of Minas Gerais, Brazil, which included 248 children and adolescents diagnosed with ASD (case group) and 886 children and adolescents without a diagnosis of ASD (control group).Interviews were conducted with the mothers of children and adolescents and a semi-structured questionnaire was used to collect data. For data analysis, a multiple logistic regression model was adopted. The magnitude of associations was estimated by the odds ratio (OR). Three multiple models were fitted: Model 1: presence or absence of breastfeeding; Model 2: duration of breastfeeding; Model 3: duration of exclusive breastfeeding.
RESULTS: ASD was associated with the absence of breastfeeding in the three adjusted models: Model 1: OR=2.1, CI95%=1.1-4.1; Model 2: OR=2.3, CI95%=1.2-4.5; Model 3: OR=2.3, CI95%=1.2-4.5.
CONCLUSIONS: individuals with ASD were more likely to have not received breastfeeding, however, due to the nature of case control studies, it cannot be stated that breastfeeding prevents ASD. Conducting a cohort study may clarify this relationship.
Keywords:
Breast feeding, Autism spectrum disorder, Observational study, Odds ratio
RESUMO
OBJETIVOS: avaliar a associação entre aleitamento materno e Transtorno do Espectro do Autismo (TEA) em crianças e adolescentes.
MÉTODOS: trata-se de um estudo caso-controle realizado no norte de Minas Gerais, Brasil, que incluiu 248 crianças e adolescentes com diagnóstico de TEA (grupo caso) e 886 crianças e adolescentes sem diagnóstico de TEA (grupo controle). Foram realizadas entrevistas com as mães das crianças e adolescentes e utilizado um questionário semiestruturado para coleta dos dados. Para análise dos dados foi adotado modelo de regressão logística múltipla. A magnitude das associações foi estimada pela Odds Ratio (OR). Três modelos múltiplos foram ajustados: Modelo 1: presença ou ausência de aleitamento materno; Modelo 2: duração do aleitamento materno; Modelo 3: duração do aleitamento materno exclusivo.
RESULTADOS: o TEA foi associado à ausência de aleitamento materno nos três modelos ajustados: Modelo 1: OR=2,1, IC95%=1,1-4,1; Modelo 2: OR=2,3, IC95%=1,2-4,5; Modelo 3: OR=2,3, IC95%=1,2-4,5.
CONCLUSÕES: os indivíduos com TEA tiveram maiores chances de não terem recebido aleitamento materno, no entanto, devido à natureza dos estudos de caso-controle, não se pode afirmar que o aleitamento materno previna o TEA. A realização de um estudo de coorte poderá esclarecer essa relação.
Palavras-chave:
Aleitamento materno, Transtorno do espectro autista, Estudo observacional, Razão de chances
IntroductionThe Autism Spectrum Disorder (ASD) is becoming increasingly prevalent, leading to a high socioeconomic impact among families that have any individual with this disorder.
1 A study with data from 2019 to 2020 revealed that ASD prevalence in the United States is of 1 Autistic person per 30 children between three and seventeen years old in that country.
2 The phenotype of individuals with ASD is heterogeneous and genetic and environmental factors are implied in its genesis.
3 ASD is characterized by restrictive and repetitive behavioral standards, besides persistent disabilities in social communication and interaction, which strongly impairs the process of socialization.
3Breastfeeding is one of the first experiences of social interaction of the human being, thus, its absence has been implied in neurodevelopmental disorders.
4 It is characterized by being a unique social process, dynamic and bidirectional, in which more far more than the simple transference of nutrients necessary to children's development occur, since it is established also the first social link of the child.
4 The transference of oxytocin via breast milk positively interferes with some areas that, usually, are affected in individuals with ASD, contributing with the social recognition and the establishment of social bonds, besides also collaborating with the process of neurodevelopment.
5,6The relation between breastfeeding and ASD has been explored by other studies, however, the results are still inconsistent.
4-8 Generally, what has been observed is that children with ASD demonstrate higher indexes of breastfeeding absence, or when it is present, the duration is lower, compared to children considered as neurotypical.
7-10 A systematic review with meta-analysis, carried out in 2019 and included studies from Australia, Canada, Indonesia, India, Japan, Oman, Turkey and the United States, assessed the duration and the type of breastfeeding with ASD, and identified a reduction of 58% of ASD risk among children who were breastfed and 76% in those who received exclusive breastfeeding.
8 Another meta-analysis, published in 2023, analyzed studies carried out in the United States, Egypt, Iraq, Italy and Turkey, in order to assess the association of non-breastfeeding and ASD risk, and estimated that chances of ASD associated with non-breastfeeding was of 1.81 (CI95%= 1.35–2.27).
11Given the importance of breastfeeding to the process of human growth and development and the inconsistency between previous studies and its relationship with ASD, this study aimed to assess the association between breastfeeding and ASD in children/adolescents in the North region of Minas Gerais, Brazil.
MethodsThis study is an excerpt of the research "Autism Spectrum Disorder in Montes Claros: a case-control study", conducted in Montes Claros, a municipality located in the state of Minas Gerais, Brazil. The original research aimed to identify possible associations of prenatal, perinatal and postnatal factors with ASD, among which the relationship between breastfeeding and ASD stand out. Methodological details of this study is available in previous publication.
12For the calculation of the sample size, odds ratio were (OR) estimated at 1.9 and risk exposure of 0.18 of individuals from the control group.
13,14 It was also adopted the power of study of 0.80, significance level of 0.05 and four individuals of control group per each one of the case group. The correction for the design effect was performed with deff= 1.5 and increase of 10% in order to diminish impacts of potential losses. In this way, the estimated sample size was 213 individuals for the case group and 852 for the control group.
The individuals of the case group were enrolled in eight clinics (six of them were private and/or by health insurance and the other two were public), specialized in people with ASD and the Association of Support of the Autistic Person of Northern Minas Gerais (ANDA – Portuguese acronym). The clinics and the ANDA were visited and became conscious about the importance of the study. All of them agreed to participate and provided the contact of mothers of children/adolescents, totaling 398 mothers. Individuals that had medical reports confirming ASD diagnosis and whose mothers agreed in participating in the study were included in the case group. Altogether, the case group comprised 248 individuals aged between two and fifteen years.
The control group included neurotypical children and adolescents, without traces of ASD, enrolled in 63 regular schools from the public and private network of the municipality, and that were in the same age group of the case group, in the ratio of four controls per one case. The schools where the controls were recruited were the same as the cases. Visitations to the directors of these schools to make them aware of the importance of the research were performed. Mothers were invited to participate by means of an invitation letter, informing the purpose and importance of the study. The mothers that returned the invitation letter signed were contacted by the researchers, through phone, for the scheduling of a visitation and clarification about the study. The children/adolescents of this group that presented signs of ASD, after screening with the Modified Checklist for Autism in Toddlers,
15 and/ or that had suspicion of another associated psychiatric disorder, as well as any malformation or syndrome were excluded from the study. The control group included 886 individuals aged between two and fifteen years.
For the data collection, meetings with predetermined locations and timetables were scheduled in person and individually, according to the availability of mothers. Schedules and interviews were performed by a previously trained team of students of Medicine undergraduate course, researchers of the Scientific Initiation Scholar Program. For the mothers of the case group, the interviews occurred in the period between August 2015 and January 2016, and for mothers of the control group, from February to September 2016. A semi-structured questionnaire was used, conceived after literature review and reviewed by a multidisciplinary team. The questionnaire was composed of 213 questions, subdivided in eight clusters: characterization of the subject, demographic and socioeconomic characteristics of parents, prenatal factors, events occurred at birth, neonatal factors, postnatal factors and family factors.
In this study, the analyzed exposition variables were presence or absence of breastfeeding, duration of breastfeeding (exclusive or not) and duration of exclusive breastfeeding. The last two variables were categorized in breastfeeding until six months of life, more than six months, less than six months or did not breastfed. Aiming to control possible confounding factors, the following variables were also analyzed: gender of children (male or female), age of mother at birth (<25 years, between <25 and 34 years, ≥35 years), skin color of the mother (self-declared and categorized into white and non-white), socioeconomic class according to
Criterion of Economic Classification Brazil (A/B, C or D/E classes), twin pregnancy (presence or absence), ASD in family (presence or absence), prematurity (gestational age ≥37 weeks or <37 weeks), crying at birth (presence or absence), meconium in amniotic fluid (presence or absence) and admission in NICU (yes or no).
Descriptive analyses were executed by means of the distribution of frequencies, and, with the objective of verifying the association of ASD with the analyzed variables, the chi-square test (χ
2) was used. The variables that presented a descriptive level of ≥0.20 were selected for the multiple analysis, in which the logistic regression model was adopted, with the backward stepwise procedure. The magnitude of the association between ASD and the variables of exposition was estimated by the odds ratio, with their respective 95% confidence intervals (CI95%). In this step, the significance level of α = 0.05 was adopted. Three multiple models were adjusted: Model 1 included the variable presence or absence of breastfeeding; Model 2 included the variable duration of breastfeeding; Model 3 included the variable duration of exclusive breastfeeding. The three models were adjusted by the possible confounding variables investigated.
The Hosmer & Lemeshow test and the pseudo R
2 Nagelkerke statistic were used to verify the quality of adjustment of the multiple models. It was verified the absence of multicollinearity between the dependent variables from the execution of a correlation matrix. The Statistical Package for the Social Sciences software (SPSS version 23.0, IBM – Chicago, USA) was used to conduct data analyses.
This study was approved by the Research and Ethics Committee of the State University of Montes Claros, opinion number 534.000/14.
ResultsThe total sample was composed of 1134 children and adolescents. Of these, 248 were children/adolescents with ASD and 886 without signs of this disorder. The mean age of both groups was similar (
p=0.398), being 6.4 years for the case group (± 3.5) and 6.6 (± 3.4) for the control group. In the case group, it was observed around four boys per each girl with ASD, and one boy per each girl in the control group (
p<0.001). The percentage of prematurity in the case group (18.5%) was statistically superior to that of the control group (13.2%), as well as the presence of meconium in the amniotic fluid (19.0% versus 10.0%), hospitalization in NICU (16.9% versus 7.0%) and family history of ASD (20.6% versus 6.3%). Other characteristics of the case and control groups are shown in Table 1.
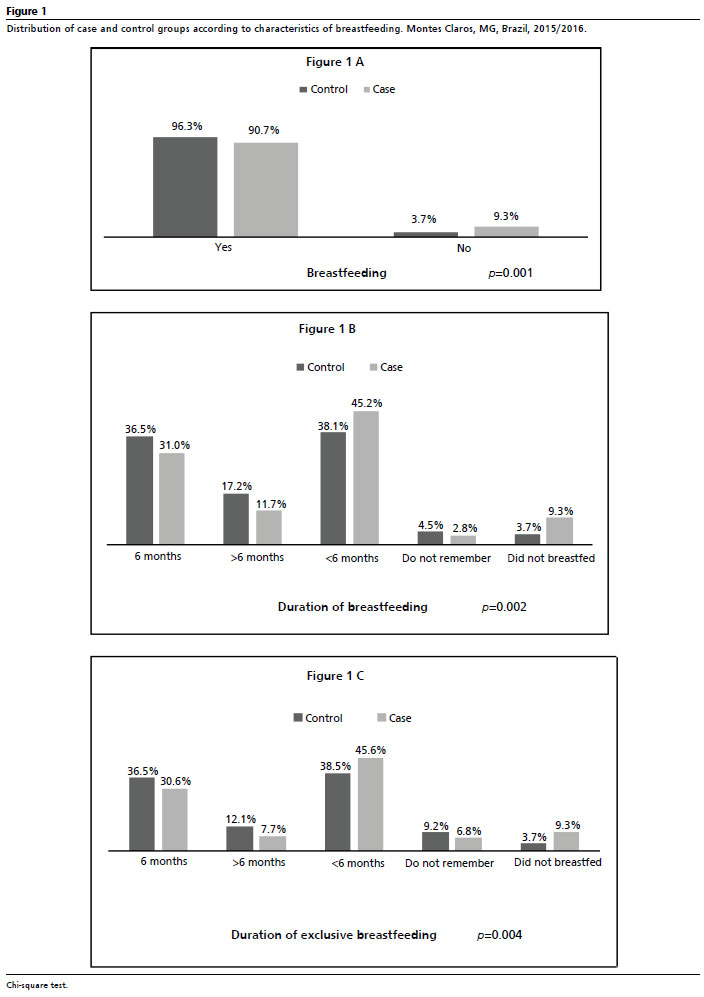
In the case group, it was also observed a higher percentage (9.3%) of children/adolescents that were not breastfed, compared to the control group (3.7%) or demonstrated lower duration of breastfeeding. This proportion persisted even when the duration and type of breastfeeding (exclusive or not) were detailed (Figure 1).
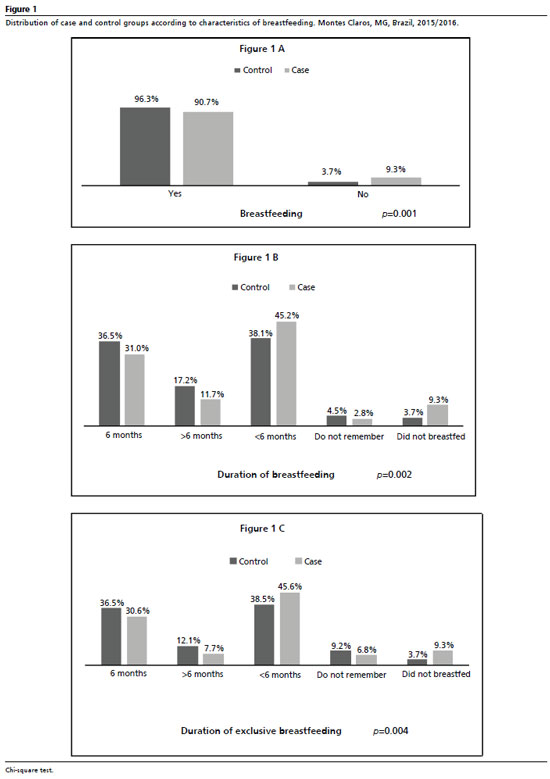
In the bivariate analysis, the following variables presented significant association, to the level of 0.20, with ASD and were selected for the multiple analysis: breastfeeding, duration of breastfeeding, duration of exclusive breastfeeding (Figure 1), gender, prematurity, twin pregnancy, crying at birth, presence of meconium in the amniotic fluid, hospitalization in NICU, family history of ASD, gestational age at birth and skin color of the mother (Table 1). In the multiple analysis, in the three adjusted models, it was noticed that the absence of breastfeeding presented a significant association with ASD (OR= 2.1; OR= 2.3 and OR=2.3). The results indicate that the duration of breastfeeding did not demonstrate association with ASD in the investigated sample. (Table 2).
DiscussionThe present case-control study aimed to assess the association between breastfeeding and ASD in a sample of children and adolescents in the North of Minas Gerais. The results suggest that the chances of not have been exposed to breastfeeding in individuals from the group case were around two times higher than those observed in the control group, after adjustments for the confounding variables investigated. Problems with social interaction and communication are some of the main factors for the diagnosis of individuals with ASD,
3 and then the importance of exploring factors that influence the development of these characteristics. It is already know the positive role performed by breastfeeding in the reduction of the occurrence of several medical conditions in both long and short terms, as well as the future intellectual development of children, promoting an increase in the intelligence quotient indexes.
16.17Besides the aforementioned benefits, other benefits of breastfeeding have been investigated, especially for individuals with ASD.
17 It has been demonstrated that breast milk acts improving communication and adaptability, which are impaired zones for these individuals.
16-18 An Australian cohort, started in 1989, evidenced that lactating children that received breastfeeding for four months or more presented better average scores of adaptability and communication with one year old, whilst those that were breastfed for less than four months presented a 1.82 risk of late adaptability and 1.66 of late communication compared to the others.
19One of the justifications for the possible protective factor of breast milk in the development of ASD is related to the action that it performs in the development of the immune and neurological systems, by means, for example, of the gut microbiota.
20 The gut microbiota is formed in the first years after birth and include a variety of microorganisms.
20 It interacts directly on the central nervous system through the myenteric plexus, constituting the brain-intestine-microbiota axis, which influences directly on the development and behavior of children.
20The gut microbiota produces substances that are essential to the immune maturation and for the neural plasticity, so that the alterations in its composition have been determinant to the development of neural-psychiatric disorders, ASD among them.
20 The action of breastfeeding, the first food human beings have contact with, in the brainintestine-microbiota axis, occurs by means of the building of a healthy microbiota that promotes a good neural development.
21 Besides, alterations in the gut microbiota also have been associated to clinical manifestations and the spectrum of severity of ASD, being gastrointestinal disorders present in children with ASD, being constipation or diarrhea, examples that may be aggravated due to alterations in the microbiota.
21The protective effect of breastfeeding is related to the transference of oxytocin via breast milk during breastfeeding.
5,6,22,23 This neuropeptide is constituted by nine amino acids and is produced by magnocellular neurons of the paraventricular nucleusand the supraoptic hypothalamus nucleus and is implied in the modulation of the social and cognitive behavior of the human being.
5.6 Studies has demonstrated that oxytocin increases group confidence and acts in the improvement of emotional recognition.
22,24 Since social and cognitive deficit are characteristics of ASD, oxytocin has been implied in the physiopathology of this disorder.
Other studies
4,7,24 also corroborate the findings of the present study, in which individuals with ASD had lower chances of exposure to breastfeeding. One meta-analysis, performed in 2019, which includes studies from Turkey, India and United States demonstrated that individuals with ASD had lower chance of having received breastfeeding compared to individuals without ASD, and data persisted when those who received artificial feeding were accounted for.
4 A case- control study, carried out in 2006 that used data from the global research Autism Internet Research Survey, estimates chances 2 times and a half higher of ASD among children that were not breastfed compared to those breastfed for more than six months.
25This study identified the fact that individuals with ASD, when breastfed, presented lower duration of breastfeeding compared to those of the group case. However, in the multiple models, after adjusting for the confounding factors, the duration of breastfeeding did not show significant association with ASD. We highlight that the variables duration of breastfeeding and duration of exclusive breastfeeding had, respectively, 47 (4.4%) and 99 (9.2%) of missing data, since mothers did not remember this information. Some studies demonstrate that the increase of the duration of breastfeeding is related to a reduction on ASD diagnoses.
9,25,26 A multicentric cohort study carried out in Spain, in 2003, demonstrated that breastfeeding for a longer time enhances cognitive development and reduces the manifestation of ASD signs, even after adjustments for confounding factors.
26 Children with breastfeeding for longer time tend to present higher neural sensibility to corporal expressions that indicate happiness, in a manner that breastfeeding interfere in neural trends to manifestations of fear and happiness.
5The lower duration of breastfeeding in individuals with ASD may be explained by the fact that breastfeeding is harder for mothers of the case group, as it has been demonstrated in the literature.
27 There is reports that even before diagnosis, children with ASD already showed some of the characteristics such as reduction of social interaction and lack of cooperation.
27One interesting data obtained in this study, is related to the continuity of exclusive breastfeeding after six months of age. This finding contradicts the guidelines of the main international organs, such as the World Health Organization and Ministry of Health of Brazil, besides going against other studies that demonstrated early onset of complementary food.
28,29 The continuity of exclusive breastfeeding after the six first months of life is not benefic, since breast milk cannot supply all of the nutritional needs of children after the sixth month of life. In this way, the continuity of exclusive breastfeeding after the sixth month, as well as the early introduction of food, are unfavorable, and families should be adequately guided with regard to the guidelines about the proper period of food introduction, and about other problems that can occur due to the early and/or late introduction of foods but the breastmilk.
30Some limitations should be considered in the present study. The main one regards the self-declaration of information by mothers, in which memory bias could have occurred, which impaired the accurate delimitation of the days that the child received breastfeeding. However, it is worth highlighting the importance of the study, with great sample size (248 cases and 886 controls) and the adjustment of models for the variables that demonstrated statistical association with ASD in previous studies.
This study verified that children and adolescents with ASD had higher chances of not having received breastfeeding. However, due to the design of this study, it is not possible to affirm that breastfeeding prevents ASD. The execution of a cohort study may clarify this relationship in a more adequate manner and reinforce, once more, the importance of breastfeeding for the proper children'sgrowth and development.
References1. Baio J, Wiggins L, Christensen DL, Maenner MJ, Daniels J, Warren Z,
et al. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years - Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2014. MMWR Surveill Summ. 2018 Apr; 67 (6): 1-23.
2. Li Q, Li Y, Liu B, Chen Q, Xing X, Xu G,
et al. Prevalence of Autism Spectrum Disorder Among Children and Adolescents in the United States From 2019 to 2020. JAMA Pediatr. 2022 Sep; 176 (9): 943-5.
3. Maenner MJ, Shaw KA, Baio J, EdS1; Washington A, Patrick M,
et al. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years - Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016. MMWR Surveill Summ. 2020 Mar; 69 (4): 1-12.
4. Tseng PT, Chen YW, Stubbs B,
et al. Maternal breastfeeding and autism spectrum disorder in children: a systematic review and meta-analysis. Nutr Neurosci. 2019 May; 22 (5): 354-362.
5. Krol KM, Rajhans P, Missana M, Grossmann T. Duration of exclusive breastfeeding is associated with differences
6. Dölen G. Autism: Oxytocin, serotonin, and social reward. Soc Neurosci. 2015; 10 (5): 450-65.
7. Soke GN, Maenner M, Windham G, Moody E, Kaczaniuk J, Diguiseppi C,
et al. Association Between Breastfeeding Initiation and Duration and Autism Spectrum Disorder in Preschool Children Enrolled in the Study to Explore Early Development. Autism Res. 2019 May; 12 (5): 816-29.
8. Ghozy S, Tran L, Naveed S, Quynh TTH, Zayan AH, Waqas A,
et al. Association of breastfeeding status with risk of autism spectrum disorder: A systematic review, dose-response analysis and meta-analysis. Asian J Psychiatr. 2020 Feb; 48: 101916.
9. Cheng J, Eskenazi B, Widjaja F, Cordero JF, Hendren RL. Improving autism perinatal risk factors: a systematic review. Med Hypotheses. 2019; 127: 26-33.
10. Manohar H, Pravallika M, Kandasamy P, Chandrasekaran V, Rajkumar RP. Role of Exclusive Breastfeeding in Conferring Protection in Children At-Risk for Autism Spectrum Disorder: Results from a Sibling Case-control Study. J Neurosci Rural Pract. 2018; 9 (1): 132-6.
11. Jenabi E, Bashirian S, Salehi AM, Khazaei S. Not breastfeeding and risk of autism spectrum disorders among children: a meta-analysis. Clin Exp Pediatr. 2023 Jan; 66 (1): 28-31.
12. Maia FA, Oliveira LMM, Alves MR,
et al. Transtorno do espectro do autismo e idade dos genitores: estudo de caso-controle no Brasil. Cad Saúde Pública. 2018; 34 (8): e00109917.
13. Quinlan CA, McVeigh KH, Driver CR, Govind P, Karpati A. Parental Age and Autism Spectrum Disorders Among New York City Children 0-36 Months of Age. Matern Child Health J. 2015; 19 (8): 1783-90.
14. Budi LPR, Sitaresmi MN, Windiani IGAT. Paternal and maternal age at pregnancy and autism spectrum disorders in offspring. Paediatr Indones. 2015; 55 (6): 345-51.
15. Alves MR, Maia FA, Almeida MTC, Saeger VSA, Silva VB, Bamdeira LVS,
et al. Estudo de Propriedades Psicométricas do M-Chat no Brasil. Psicol Ciênc Prof. 2022; 42: e238467.
16. Horta BL, de Sousa BA, de Mola CL. Breastfeeding and neurodevelopmental outcomes. CurrOpin Clin NutrMetab Care. 2018;21(3):174-178.
17. American Academy of Pediatrics (AAP). Why breastfeed: Benefits for you & your baby. [
Internet]. [access in 2020 Mar 5]. Available from:
https://www.healthychildren.org/English/ages-stages/baby/breastfeeding/Pages/WhyBreastfeed.aspx18. Mello AMSR, Andrade MA, Ho H, Dias IS. Retratos do autismo no Brasil. 1ª ed. São Paulo: AMA; 2013.
19. Oddy WH, Li J, Whitehouse AJ, Zubrick SR, Malacova E. Breastfeeding duration and academic achievement at 10 years. Pediatrics. 2011; 127 (1):e137-e145.
20. O'Sullivan A, Farver M, Smilowitz JT. The Influence of Early Infant-Feeding Practices on the Intestinal Microbiome and Body Composition in Infants. Nutr Metab Insights. 2016 Oct; 8 (Suppl. 1): 87.
21. Ribeiro R, Nicoli JR, Santos G, Lima-Santos J. Impact of vitamin deficiency on microbiota composition and immunomodulation: relevance to autistic spectrum disorders. Nutr Neurosci. 2021; 24 (8): 601-13.
22. Green JJ, Hollander E. Autism and oxytocin: new developments in translational approaches to therapeutics. Neurotherapeutics. 2010; 7 (3): 250-7.
23. Yamasue H, Domes G. Oxytocin and Autism Spectrum Disorders. Curr Top BehavNeurosci. 2018; 35: 449-65.
24. Bakermans-Kranenburg MJ, van I Jzendoorn MH. Sniffing around oxytocin: review and meta-analyses of trials in healthy and clinical groups with implications for pharmacotherapy. Transl Psychiatry. 2013; 3 (5): e258.
25. Schultz ST, Klonoff-Cohen HS, Wingard DL, Akshoomoff NA, Macera CA, Ji M,
et al. Breastfeeding, infant formula supplementation, and Autistic Disorder: the results of a parent survey. Int Breastfeed J. 2006 Sep; 1: 16.
26. Boucher O, Julvez J, Guxens M, Arranz E, Ibarluzea J, Miguel MS,
et al. Association between breastfeeding duration and cognitive development, autistic traits and ADHD symptoms: a multicenter study in Spain. Pediatr Res. 2017 Mar; 81 (3): 434-42.
27. Bittker SS, Bell KR. Acetaminophen, antibiotics, ear infection, breastfeeding, vitamin D drops, and autism: an epidemiological study. Neuropsychiatr Dis Treat. 2018; 14: 1399-1414.
28. Lemcke S, Parner ET, Bjerrum M, Thomsen PH, Lauritsen MB. Early regulation in children who are later diagnosed with autism spectrum disorder: A longitudinal study within the Danish National Birth Cohort. Infant Ment Health J. 2018; 39 (2): 170-82.
29. Dallazen C, Silva SA, Gonçalves VSS, Nilson EAF, Crispim SP, Lang RMF,
et al. Introdução de alimentos não recomendados no primeiro ano de vida e fatores
30. Schincaglia RM, Oliveira AC, Sousa LM, Martins CA. Práticas alimentares e fatores associados à introdução precoce da alimentação complementar entre crianças menores de seis meses na região noroeste de Goiânia. Epidemiol Serv Saúde. 2015; 24 (3): 465-74.
Author's contribution: Silva BS, Cezar IAM, Bandeira LVS, Oliveira SLN, Saeger VSA: conceptualization of the study, data collection and elaboration of the article.Freire RS and Rezende LF: elaboration and critical review of the article. Alves FD, Silveira MF: conceptualization and study design, supervision of data collection, data analysis and interpretation and critical review of the article. All authors approved the final version of the article and declare no conflicts of interest.
Received on December 16, 2022
Final version presented on December 7, 2023
Approved on December 11, 2023
Associated Editor: Lygia Vanderlei


 ; Fernanda Dias Alves2
; Fernanda Dias Alves2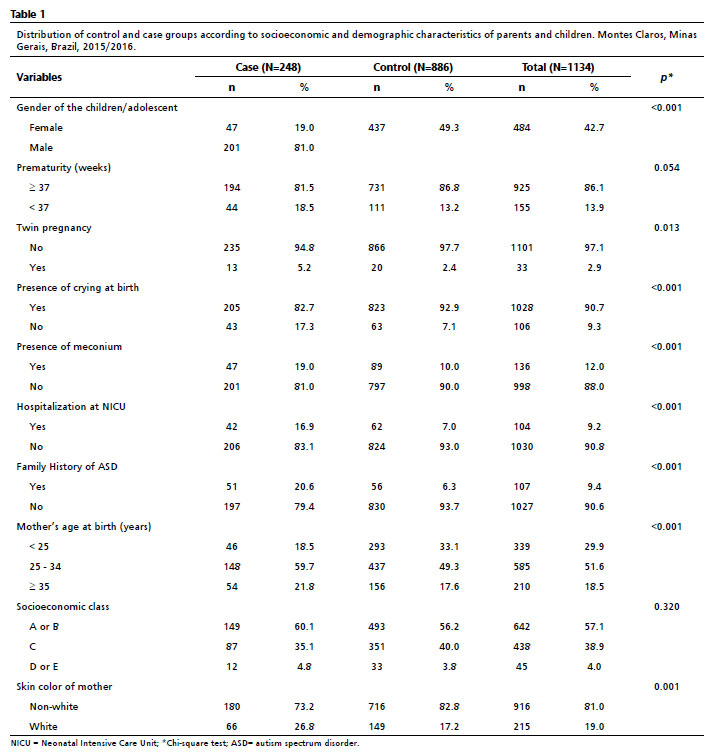







 Ler em português
Ler em português