ABSTRACT
OBJECTIVES: to analyze the prevalence of sugar consumption and associated factors in childcare consultations.Methods: cross-sectional study with 599 children > six months to < 24 months of age, assisted by the Family Health Units. Outcomes: daily consumption of sweetened beverages, sweets/candies, recorded in the Food and Nutrition Surveillance System; independent variables: sociodemographic data. Multiple logistic regression test was applied.
RESULTS: 62.10% of the children consume sugary drinks and 42.23%, sweets/candies. Consuming sugary drinks was associated with the age of 12-17 months and 29 days (OR=2.525; CI95%=1.68-3.78) and 18-17 months and 29 days (OR=2.90; CI95%=1.90-4.43); children living with more than four people at home (OR=1.59; CI95%=1.11-2.26), aged 12-17 months and 29 days (OR=2.05; CI95%=1.34-3.13) and 18-23 months and 29 days (OR=2.51; CI95%=1.62-3.87) were more likely to consume sweets/candies than younger children. Maternal aspects, such as age (OR=0.66; CI95%=0.46-0.93), marital status (OR=1.67; CI95%=1.06-2.6), schooling (OR=2.14; CI95%=1.12-4.08), and presence of government assistance (OR=2.03; CI95%=1.41-2.93), were conditions associated with the consumption of sweets.
CONCLUSIONS: the prevalence of sugar in children's diet was high and was associated with sociodemographic aspects. Health education actions should be carried out in childcare, in order to promote healthy food, minimizing the consumption of sugar.
Keywords:
Food, Sugary drinks, Complementary nutritional information
RESUMO
OBJETIVOS: analisar a prevalência do consumo de açúcar e fatores associados em consultas de puericultura.
MÉTODOS: estudo transversal com 599 crianças >seis a <24 meses de idade, assistidas por Unidades de Saúde da Família. Desfechos: consumo diário de bebidas adoçadas, doces/guloseimas, registrados no Sistema de Vigilância Alimentar e Nutricional; variáveis independentes: dados sociodemográficos. Aplicou-se teste de regressão logística múltipla.
RESULTADOS: 62,10% das crianças consomem bebidas açucaradas e 42,23% doces/guloseimas. Consumir bebidas açucaradas associou-se à idade de 12-17 meses e 29 dias (OR=2,525; IC95%=1,68-3,78) e 18-17 meses e 29 dias (OR=2,90; IC95%=1,90-4,43); crianças residirem com mais de quatro pessoas na casa (OR=1,59; IC95%:1,11-2,26), terem idade de 12-17 meses e 29 dias (OR=2,05; IC95%=1,34-3,13) e 18-23 meses e 29 dias (OR=2,51; IC95%=1,62-3,87) apresentaram maior chance de consumir doces/guloseimas que crianças mais novas. Aspectos maternos como idade (OR=0,66; IC95%=0,46-0,93), estado civil (OR=1,67; IC95%=1,06-2,6), escolaridade (OR=2,14; IC95%=1,12-4,08), e presença de auxílio do governo (OR=2,03;IC95%=1,41-2,93), foram condições associadas ao consumo de doces/guloseimas.
CONCLUSÃO: foi alta a prevalência de açúcar na dieta das crianças e esteve associada a aspectos sociodemográficos. Ações de educação em saúde devem ser realizadas na puericultura, a fim de fomentar a alimentação saudável, minimizando o consumo de açúcar.
Palavras-chave:
Alimentos, Bebidas açucaradas, Informação nutricional complementar
IntroductionThe early stages of a child’s life are sensitive to nutritional and metabolic factors, which affect not only growth and development but also their future health condition.
1 Breastfeeding is recommended as the primary source of the child’s diet, persisting until the age of two, and other food sources should be inserted from six months on, preferably containing proteins, vitamins, and minerals.
2However, food choices are determined by biological, socioeconomic, demographic, and cultural variables in a dynamic process, which varies according to the context and the life stage of individuals.
3-5The development of eating behavior by the child can be influenced by the availability of certain food, as well as by the frequency to which the child is exposed to them, especially from six months of life. During this period, many mothers tend to offer food that are more pleasing to the child’s taste, often not considering healthier choices.
3 Thus, the offer of sweets, such as cookies, chocolate, or even the addition of refined sugar to the milk offered in the bottle, is very common and can contribute significantly to damaging the child’s health.
6The World Health Organization (WHO), in its guidelines, expresses concern regarding the consumption of sugar by children, highlighting that sugary drinks are the main vectors of a caloric diet.
7 Artificial drinks are nutritionally deficient and consist primarily of free of sugar and sodium added. Added sugar are included in preparations to make them look and taste better.
8Excessive calorie intake, observed at increasingly early ages, is related to the occurrence of dental caries and the development of chronic non-communicable diseases, such as obesity, thus compromising the nutritional, oral and general health of individuals.
9 In this sense, it is essential that children are periodically monitored by health professionals to assess their growth and development. This follow-up should be carried out by a multidisciplinary team, and is offered by the
Atenção Primária em Saúde (APS) (Brazilian Primary Health Care) in childcare consultations for children under six years old. The central focus of childcare is disease prevention and health education.
10 These interconnected lines can contribute to healthy behaviors related to the child’s diet.
11Considering that the identification of incorrect eating habits is essential to avoid damage to children’s health, this theme therefore supports actions to promote health in childhood. Thus, this study aimed to know the prevalence of consumption of sweetened beverages, sweets, or treats in children from six months to 23 months and 29 days of age, accompanied at childcare, and to identify the maternal socioeconomic and demographic variables that are associated with this consumption.
MethodsThis is an analytical cross-sectional study with children from six months to 23 months and 29 days old. The city studied is medium-sized, from the countryside of São Paulo. It has an estimated population of 388,412 thousand inhabitants, a territorial area of 1,378,501km², and a demographic density of 264.47 inhabitants/km.
12 According to reports made available by the Municipal Secretariat of Health, from January to April 2016, there were a total of 1169 children aged from zero to 23 months and 29 days registered at the Family Health Units (FHU) in the city. The public healthcare network consists of 122 establishments of the
Sistema Único de Saúde(SUS)(Public Health System) including 52 FHUs, 20 Basic Health Units, 32 Reference Centers in Primary HealthCare, four Emergency Medical Care Units, in addition to specialized clinics, centers, and outpatient clinics.
The sample size was calculated in EPI INFO7 considering a confidence level of 95%, a test power of 80%, unexposed/exposed rate = 1, response percentage in the unexposed group of 73%, and OR=1.8, obtaining a minimum sample size of 582 individuals randomly selected in the micro areas of public health agents belonging to the 52 FHUs.
The sample included women aged between 18 and 50 years old, with children from six to 23 months and 29 days, and who were aware of their child’s feeding the day before. Interviews with people other than the mother herself were excluded from the sample.
The study was conducted with 599 children in the included age group, registered as users of the 52 FHUs in the city, from February to July 2017. Initially, telephone contact was made with the FHU managers to schedule the date and time of data collection.
For the collection of socioeconomic data, the following variables were considered: family income, number of people in the household, type of housing, and mother’s schooling level. Also, questions were added regarding demographic characteristics (age, marital status, number of children and whether the mother had a job, who was the head of the family, whether the home had television and/or internet, and whether they received government assistance).
This study used the
Formulário de Marcadores de Consumo Alimentar do Ministério da Saúde – Sistema de Vigilância Alimentar e Nutricional(Food Consumption Markers Form of the Brazilian Ministry of Health – Food and Nutrition Surveillance System) for children from six to 23 months and 29 days of age, which was based on an evaluation document and indicators of infant and child’s feeding practices, published by WHO.
13The form presents questions aimed in detecting the quality and timely introduction of food, identifying risks or protection for nutritional deficiencies and the occurrence of overweight. It contains 20 closed questions where the mother answers: Yes, No, or Does not know. In this instrument, the child’s age and sex were also filled in.
The dependent variable (consumption of sweet food or treats and sweetened beverages) was dichotomized into yes/no.
The sweetened beverages considered were: soft drink, bottled juice, powdered juice, bottled coconut water,
guaraná or syrups, fruit juice with added sugar; sweet food or treats were considered as: cookies, sweets, cakes, chocolates, candies, chewing gum, among other sugary products.
The independent variables age, marital status, number of children the mother has, family income, number of people in the household, type of home, mother’s schooling level, and whether the home has television and/or internet were dichotomized by the median; the child’s age was divided into the categories: 06 to 11 months and 29 days, 12 to 17 months and 29 days, and 18 to 23 months and 29 days, according to the guidelines suggested by the marker.
To evaluate the association between the consumption of sweet food, treats, and sweetened beverages and the independent variables, multiple logistic regression analysis was applied. Variables with
p≤0.20 in the crude analysis were tested in the multiple logistic regression model, and those that continued to be associated with the consumption of these food and beverages, with
p≤0.05 after adjustment for the other variables analyzed, remained in the multiple model. The Odds Ratio (OR) and the respective 95% confidence intervals (CI) were estimated. The significance level adopted was 5%. All statistical tests were performed by the SAS 9.4 program (SAS Institute Inc., Cary, NC, USA. release 9.4, 2010).
The study was approved by the Research Ethics Committee of the
Faculdade de Odontologia de Piracicaba- FOP-Unicamp (CAAE: 61502116.6.0000.5418).
ResultsTable 1 shows the frequent distribution of consumption of sweetened beverages as a function of the variables analyzed. Of the total of 599 children analyzed, this consumption was found in 372 (62.10%) of them; 50.75% were female.
Regarding the children’s mothers, 52.08% were ≤27 years old, 82.82% were married/other, 73.62% had up to two children, and 72.48% had a monthly income of up to R$1,874.
Of the total sample, mothers with children aged 18 to 23 months and 29 days (71.74%), mothers up to 27 years old (47.12%), single mothers (71.57%), with three or more children (68.99%), with an income up to R$1,874.00 (64.35%), living with more than four people at home (68.09%), ≤ graduated from high school (63.08%), and who received government assistance (67.02%) have children who consume more sweetened beverages.
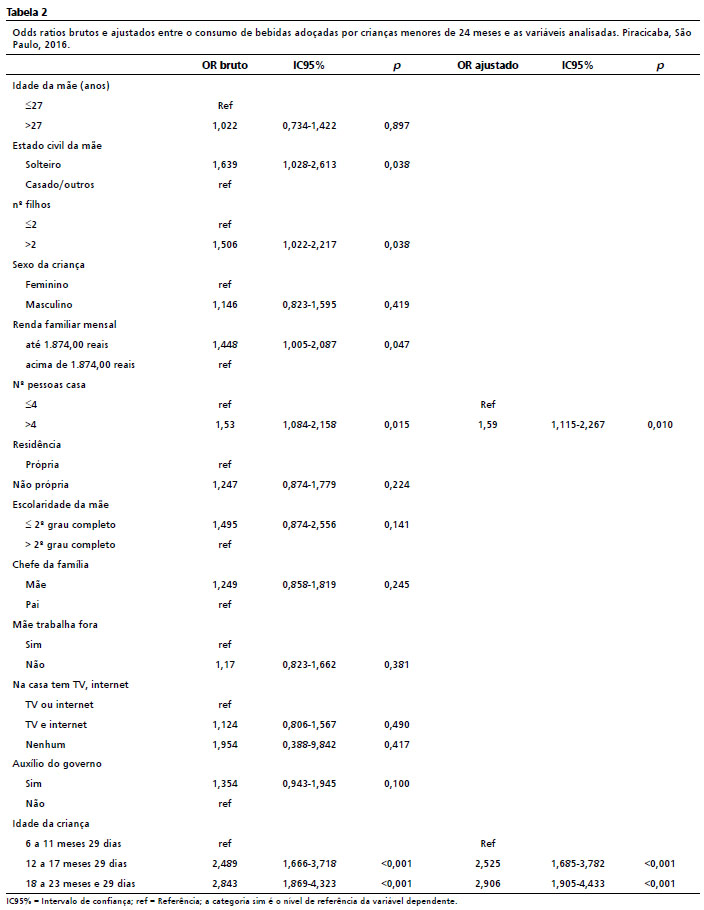
Table 2 presents the crude and adjusted odds ratios between consumption of sweetened beverages and the analyzed variables. In the crude analysis, the factors associated with the consumption of sweetened beverages were the mother’s marital status, the number of children, the family’s monthly income, the number of people in the household, and the child’s age. In the adjusted analysis, children aged 12 to 17 months and 29 days and 18 to 23 months and 29 days had a higher chance (OR=2.525; CI95%=1.685-3.782;
p<0.001 and OR=2.906; CI95%=1.905-4.433;
p<0.001, respectively) of consuming sweetened beverages. In terms of the number of people in the household, there was a higher chance (OR=1.590; CI95%=1.115-2.267;
p=0.010) of consuming sweetened beverages by children who live with more than four people.
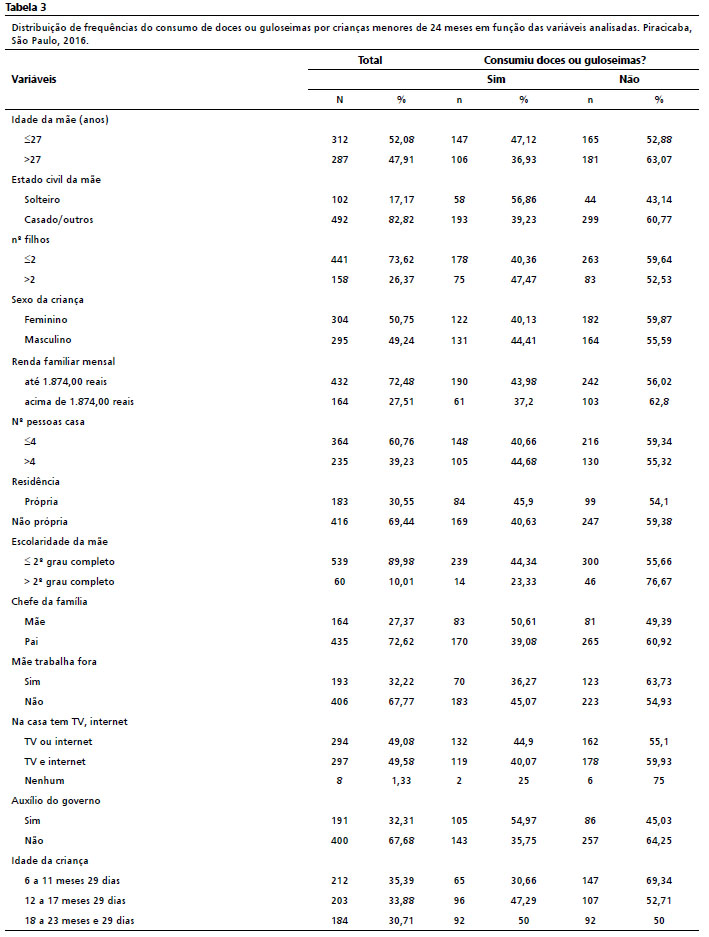
Table 3 shows the frequency distribution of consumption of sweets or treats as a function of the variables analyzed. Consumption was observed in 253 children (42.23%).
Of the total sample, mothers with children aged 12 to 17 months and 29 days (47.29%) and 18 to 23 months and 29 days (50%), mothers up to 27 years old (47.12%), single mothers (56.86%), with three or more children (47.47%), with an income up to R$ 1,874.00 (43.98%), who lives with more than four people at home (44.68%), ≤ graduated from high school (44.34%), and receives government assistance (54.97%) have children who consume more sweets or treats.
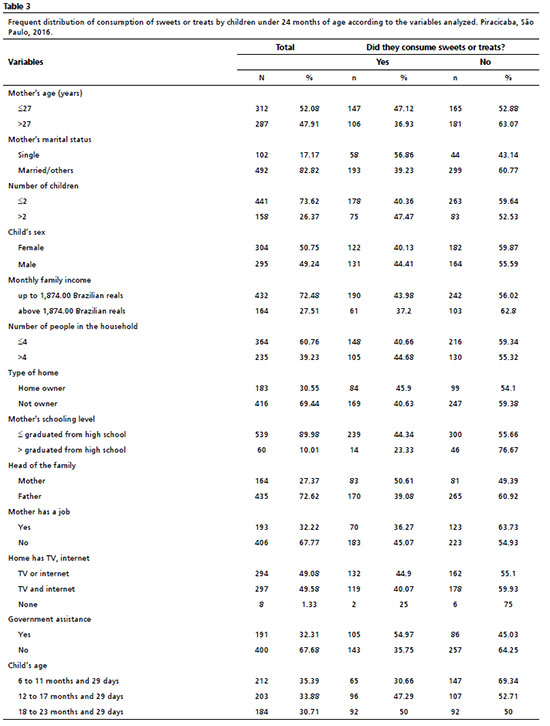
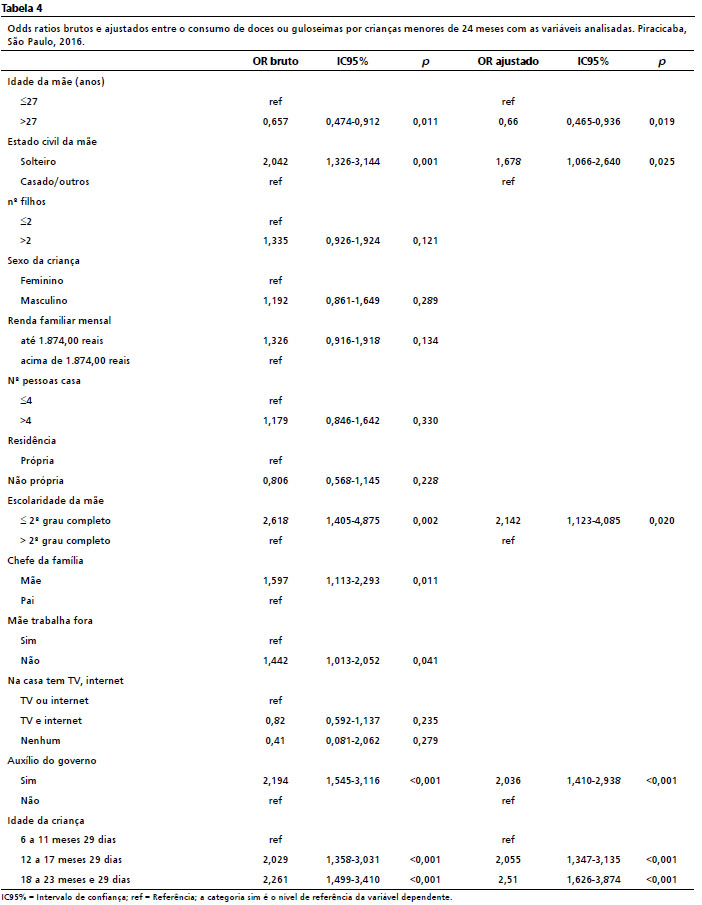
Table 4 presents the crude and adjusted odds ratios between consumption of sweets or treats and the analyzed variables. The maternal factors associated with the consumption of sweets or treats in the crude analysis were: age, marital status, mother’s schooling, being head of the family, having a job, receive government assistance, and the child’s age. In the multiple analysis, the children who had the highest chance of consuming sweets or treats were those aged 12 to 17 months and 29 days and 18 to 23 months and 29 days (OR=2.055; CI95%=1.347-3.135;
p<0.001 and OR=2.510; CI95%=1.626-3.874;
p<0.001, respectively). Children whose mothers were single, ≤ graduated from high school, and who receives government assistance had a higher chance (OR=1.678; CI95%=1.066-2.640;
p=0.025, OR=2.142; CI95%=1.123-4.085;
p=0.020, and OR=2.036; 95% CI=1.410-2.938;
p=0.001, respectively) of consuming sweets or treats. On the other hand, those whose mothers aged > 27 years old had a lower chance (OR=0.660; CI95%=0.465-0.936 and
p=0.019) of consuming sweets or treats.
DiscussionBased on the results, one can observe early introduction of sugar is presented, and often in excess, in the diet of the children studied, 62.10% of the sample consumes sweetened beverages and 42.23% consume sweets or treats.
Published studies have shown results similar to these, indicating high sugar consumption by children.
3,5 An analysis that used data from the National Health Survey and included information from 2,541 children between 12 and 23 months of life, whose families answered specific questions for this age group, identified that 85.5% of the respondents stated that the children consumed sugary and inappropriate food daily.
4Excessive consumption of sweetened beverages has been associated with the occurrence of overweight in the pediatric population, which favors the early development of chronic non-communicable diseases, such as diabetes and hypertension.
9 According to current recommendations, the intake of free of sugar should be equivalent to less than 10% of the total daily energy intake.
7 A multicenter study conducted in five Brazilian cities found that the consumption of sweetened beverages, including soft drinks and artificial juices, corresponded to 37% of the energy from liquids consumed daily by children aged three to six years old.
14 This alerts to the need for control measures in sugar consumption from the birth of the child.
Similarly, Vega
et al.15 reported that more than a third of Brazilian preschoolers, representing almost three million children, consumed sweetened beverages for four days a week or more, also identifying that the highest prevalence of frequent consumption of sweetened beverages was observed in the age group of 36 to 47 months. The consumption of at least once a week of sweets and soft drinks was verified in more than 70% of the children, and the highest frequency of daily consumption of sweets and soft drinks was observed in children from the south of the country.
16A study conducted with 304 children aged 24 months found that breastfeeding was not the exclusive food until six months of age in 47.4% of the children. The same research also identified that inappropriate eating practices were associated with the fact that the mother worked outside the home and was under 25 years old, emphasizing the influence of family characteristics on the children’s diet.
17In both cases (consumption of sweetened beverages and sweets or treats), the highest chances of consumption of these products were seen in the age groups from 12 to 17 months and 29 days and 18 to 23 months and 29 days, compared to the age group from six to 11 months and 29 days, indicating that, with advancing age, the consumption of these products tends to increase. Similarly, in a study conducted in public clinics in Finland, the authors identified that almost half of babies under six months of age already consumed sugar (44%), with 56% of children in the 19-24 months age group consuming sugary food and/or drinks more than once a week. Almost all mothers with children 16 months and older reported giving sweets to their children.
18Exposure to sweet flavors, especially in the first months of life, makes the acceptance of the sweet increasingly easier, which compromises the establishment of a solid nutritional base with sugary food preferences that extend over the years.
19 It is also for this reason that the Pan American Health Organization (PAHO) draws attention to the excess of advertisements for sugar-rich food.
20 The marketing used in the media aims to form emotional bonds with children as, for example, they offer fun by the use of cartoons, children’s characters, and gifts. Therefore, the lack of more effective regulation exposes this public and their families to advertising considered invasive and capable of harming any advice on good eating habits that health professionals seek to carry out with families.
21In this study, there was a large consumption of sweetened beverages by the evaluated public, which, when considering the socioeconomic and demographic characteristics of the families due to the consumption of these beverages, was associated with the number of people who live in the household, showing that the chances of consumption were higher at home with more than four people.
It is evident that the consumption of sugar-sweetened beverages by young children is influenced by several factors, including family characteristics and behaviors.
22 As a consequence of the early introduction of sweetened beverages, impaired breastfeeding is observed. A study conducted with 847 children assisted in Primary HealthCare (PHC), in the Federal District, revealed premature food introduction among 38.8% of children under six months of age. In this segment, 18.4% of the babies already consumed drinks with added sugar, honey, or sweetener. The study also pointed out that the lower consumption of beverages with added sugar, honey, and sweeteners contributes to a greater chance of breast milk intake. Among the children aged 12 and 24 months, breast milk intake was associated with lower consumption of processed juice, soda, and sweetened beverages,
23 reinforcing the need to counsel and support interventions for families on this issue. In general, nutritional education aimed for parents is an important aspect to be considered, since it will affect the children’s eating habits and reduce the consumption of sweetened beverages in the family environment, thus reducing the chances of children consuming these products. Also in the United States, a study observed that, to try to reduce the consumption of sweetened beverages for children, there is a need to interfere with the food choices of the adults who accompany them.
24This meeting of the professional with the caretakers promotes bonding with the family, and has an educational nature regarding the consumption of certain food groups during food introduction. Nevertheless, one can observe that an in-depth investigation on the children’s feeding and the cultural diversity of the families is not carried out, which makes it difficult to value the regional food consumed by them. These aspects suggest the need to qualify health professionals to promote a healthy food introduction.
25Concerning the consumption of sweets or treats, mothers aged 27 years or more, single mothers, and mothers with schooling up to high school, and those who receive government assistance showed higher chances of their children consuming these products, corroborating with a study that pointed out that higher consumption of sweets can be associated with lower family income and lower parental schooling.
26Also, with the objective of evaluating the consumption of ultra-processed food by children aged six to 12 months, followed by PHC in a metropolitan region of the state of São Paulo, Relvas
et al.
27 interviewed 196 mothers about their children’s feeding in the past 24 hours. They found the consumption of ultra-processed food by 43.1% of the children. The mother’s schooling level and the fact that the child’s first visit to the basic health unit took place in the first week of life were factors associated with this diet. This reveals that one must listen and understand the factors that influence the caretakers during the transition to the complementary feeding of the child.
This study has some limitations. As it is a cross-sectional study, it is not possible to infer causality, since it does not allow to state at what moment of time the exposure and the outcome occurred. In addition, studies using instruments that record food consumption are subject to random errors due, for example, to the difficulty of individuals in remembering the food consumed, interfering with the accuracy of the data collected and the frequency of consumption of sweetened beverages, sweets, and treats referred by the children’s mothers.
Finally, despite the constant recommendations and policies on healthy infant feeding, the occurrence of dietary inadequacies was evident in the studied population, supporting the idea that children’s dietary patterns converge to the increasingly early introduction of sugary food, which are poor in nutrients and can, in the long term, bring harm to the oral, nutritional, and general health of these individuals. In this way, and due to the fact, that in this age group food choices become the parents and caregivers’ responsibilities, we recommend that health education actions include multidisciplinary teams to clarify the interrelationships of excess sugar in the diet with general health, especially at the time of childcare.
References1. Black MM. Impact of Nutrition on Growth, Brain, and Cognition. Nestle Nutr Inst Workshop Ser. 2018; 89: 185-95.
2. Prell C, Koletzko B. Breastfeeding and Complementary Feeding. Dtsch Arztebl Int. 2016 Jun; 113 (25): 435-44.
3. Lopes WC, Pinho L, Caldeira AP, Lessa AC. Consumo de alimentos ultraprocessados por crianças menores de 24 meses de idade e fatores associados. Rev Paul Pediatr. 2020; 38: e2018277.
4. Rebouças AG, Bernardinho IM, Dutra ER, Imparato JCP, Duarte DA, Flório FM. Fatores associados à prática alimentar de crianças brasileiras de 12 a 23 meses de vida. Rev Bras Saúde Mater Infant. 2020; 20 (4): 1025-40.
5. Freitas LG, Cortés MAP, Stein C, Cousin E, Faustino-Silva DD, Hilgert JB. Qualidade do consumo alimentar e fatores associados em crianças de um ano de vida na Atenção Primária à Saúde. Ciênc Saúde Coletiva. 2020; 25 (7): 2561-70.
6. Carvalho CA, Fonseca PCA, Nobre LN, Silva MA, Pessoa MC, Ribeiro AQ,
et al. Fatores associados aos padrões alimentares no segundo semestre de vida. Ciênc Saúde Coletiva. 2020; 25 (2): 449-59.
7. World Health Organization (WHO). Report of the commission on ending childhood obesity [Internet]. Geneva: WHO; 2016 [access in 2021 abr 5]. Available from:
http://apps.who.int/iris/bitstream/10665/204176/1/9789241510066_eng.pdf?ua=18. Dantas FMK, Nascimento AG, Reis AM, Domingues J, Doria SR, Lopes RGAL. Informação nutricional complementar em bebidas açucaradas consumidas pelo público adolescente e infantil. Vigil Sanit Debate. 2020; 9 (1): 1-11.
9. Paglia L. WHO: healthy diet to prevent chronic diseases and caries. Eur J Paediatr Dent. 2018 Mar; 19 (1): 5.
10. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Saúde da criança: crescimento e desenvolvimento. Brasília (DF): Ministério da Saúde; 2012. (Cadernos de Atenção Básica, nº 33). [access in 2021 apr 5]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/saude_crianca_crescimento_desenvolvimento.pdf11. Góes FGB, Silva MA, Paula GK, Oliveira LPM, Mello NC, Silveira SSD. Contribuições do enfermeiro para boas práticas na puericultura: revisão integrativa da literatura. Rev Bras Enferm
. 2018; 71 (Suppl. 6): 2808-17.
12. Instituto Brasileiro de Geografia e Estatística (IBGE). Cidades: Piracicaba. [
online]. São Paulo, Brasil; 2020. [access in 2021 apr 17]. Available from:
https://biblioteca.ibge.gov.br/visualizacao/periodicos/2972/momun_se_sp_piracicaba.pdf13. World Health Organization WHO). Indicators for assessing infant and young child feeding practices. Geneva: WHO; 2010. [access in 2021 apr 17]. Available from:
https://www.who.int/publications/i/item/978924001838914. Feferbaum R, Abreu LC, Leone C. Fluid intake patterns: an epidemiological study among children and adolescents in Brazil. BMC Public Health. 2012 Nov; 12: 1005.
15. Vega JB, Poblacion AP, Taddei JAAC. Fatores associados ao consumo de bebidas açucaradas entre pré-escolares brasileiros: inquérito nacional de 2006. Ciênc Saúde Coletiva. 2015; 20 (8): 2371-80.
16. Bortolini GA, Gubert MB, Santos LM. Food consumption in Brazilian children by 6 to 59 months of age. Cad Saúde Pública. 2012; 28: 1759-71.
17. Silveira GLL, Neves LF, Pinho L. Fatores associados à alimentação entre crianças atendidas em creches públicas de Montes Claros. Rev Assoc Bras Nutr. 2018; 8 (2): 20-6.
18. Laitala ML, Vehkalahti MM, Virtanen JI. Frequent consumption of sugar-sweetened beverages and sweets starts at early age. Acta Odontol Scand. 2018 Mar; 76 (2): 105-10.
19. Murray RD. Savoring Sweet: Sugars in Infant and Toddler Feeding. Ann Nutr Metab. 2017; 70 (Suppl. 3): 38-46.
20. Organização Panamericana de Saúde (OPAS). Recomendações da Consulta de Especialistas da Organização Pan-Americana da Saúde sobre a Promoção e a Publicidade de Alimentos e Bebidas Não Alcoólicas para Crianças nas Américas. Washington, DC; 2012. [access in 2021 apr 17]. Available from:
https://iris.paho.org/handle/10665.2/359321. Sadeghirad B, Duhaney T, Motaghipisheh S, Campbell NR, Johnston BC. Influence of unhealthy food and beverage marketing on children’s dietary intake and preference: a systematic review and meta-analysis of randomized trials. Obes Rev. 2016 Oct; 17 (10): 945-59.
22. Mazarello Paes V, Hesketh K, O’Malley C, Moore H, Summerbell C, Griffin S,
et al. Determinants of sugar-sweetened beverage consumption in young children: a systematic review. Obes Rev. 2015 Nov; 16 (11): 903-13.
23. Spaniol AM, Costa THM, Bortolini GA, Gubert MB. Breastfeeding reduces ultra-processed foods and sweetened beverages consumption among children under two years old. BMC Public Health. 2020 Mar; 20 (1): 330.
24. Emond JA, Smith ME, Mathur SJ, Sargent JD, Gilbert-Diamond D. Children’s Food and Beverage Promotion on Television to Parents. Pediatrics. 2015 Dec; 136 (6): 1095-102.
25. Modes PSSA, Gaíva MAM, Monteschio CAC. Incentivo e promoção da alimentação complementar saudável na consulta de enfermagem à criança. Contexto Saúde. 2020; 20 (40): 189-98.
26. Dallazen C, Silva SA, Gonçalves VSS, Nilson EAF, Crispim SP, Lang RMF,
et al. Introdução de alimentos não recomendados no primeiro ano de vida e fatores associados em crianças de baixo nível socioeconômico. Cad Saúde Pública. 2018; 34 (2): e00202816.
27. Relvas GRB, Buccini GDS, Venancio SI. Ultra-processed food consumption among infants in primary health care in a city of the metropolitan region of São Paulo, Brazil. J Pediatr (Rio J). 2019; 95 (5): 584-92.
Received on May 26, 2021
Final version presented on May 31, 2022
Approved on June 2, 2022
Authors’ contributionReis RA and Bulgareli JV proposed the design of the study, contributed to the interpretation of the data and to the first draft of the article. Cunha IP, Cainelli E, and Gondinho BVC contributed to the interpretation of the data and to the writing of the final version of the article. Cortellazzi KL, Guerra LM, and Reche NSG contributed to the analysis of the data, the design of the study, and participated in the writing of the article. All authors contributed and approved the final version of the article and declare no conflict of interest.


 ; Inara Pereira da Cunha 2
; Inara Pereira da Cunha 2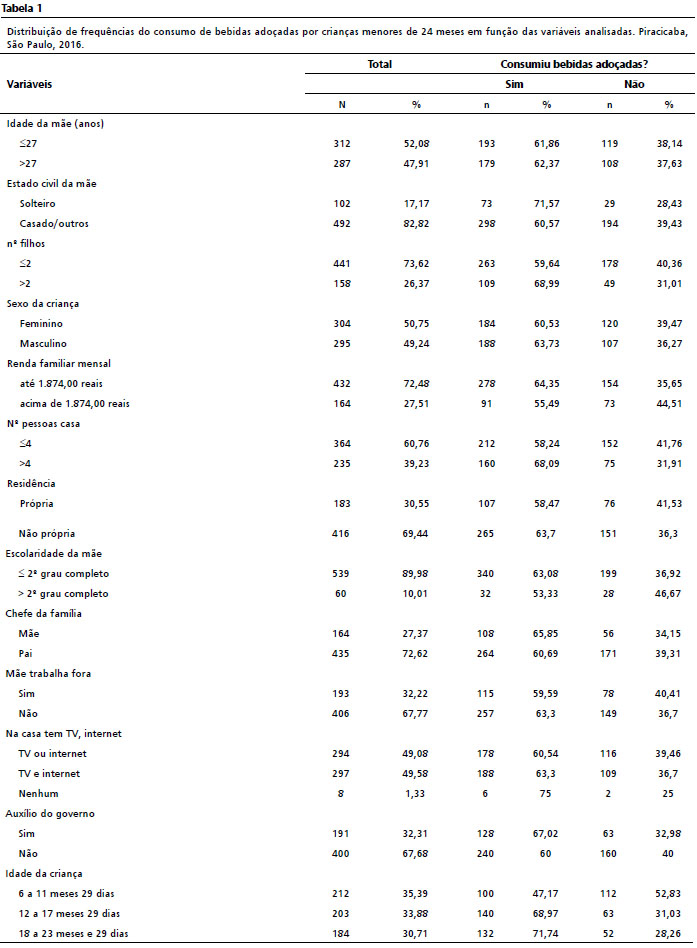






 Ler em português
Ler em português