ABSTRACT
OBJECTIVES: the aim is to determine the prevalence of hypertensive disorders and to describe the sociodemographic aspects and risk factors for preeclampsia, gestational hypertension and intrauterine growth restriction.
METHODS: a descriptive cross-sectional study. Maternal characteristics, history from the first prenatal visit and outcomes were obtained. The prevalence and percentages were calculated and described.
RESULTS: the prevalence of hypertensive disorders was 12.7%, preeclampsia was 8.0%, followed by gestational hypertension at 4.7%. Of the preeclampsia, 54.8% were severe and 11.9% were of early onset. Moreover, 56.5% of the severe preeclampsia had preterm deliveries. IUGR had a prevalence of 5.3%. Based on maternal history, the most relevant risk factors were a family and personal history of preeclampsia and IUGR.
CONCLUSIONS: we found a considerable prevalence of preeclampsia with a high percentage of preterm deliveries, associated with varying severity. This data helps health professionals to be aware of the risk factors that can be followed up for preventing complications. The determination of the risk of developing a hypertensive disorder during pregnancy is fundamental to encouraging proper counseling and care for these women through gestation.
Keywords:
Preeclampsia, Pregnancy induced hypertension, Intrauterine growth restriction, Risk factors, Prevalence, Pregnancy outcomes
RESUMO
OBJETIVOS: determinar la prevalencia de trastornos hipertensivos y describir los aspectos sociodemográficos y los factores de riesgo de preeclampsia, hipertensión gestacional y restricción del crecimiento intrauterino (RCIU).
MÉTODOS: estudio descriptivo de corte transversal. Se obtuvieron características maternas, antecedentes del primer control prenatal y los resultados obstétricos. Se calcularon y describieron las prevalencias y porcentajes.
RESULTADOS: la prevalencia de trastornos hipertensivos fue del 12.7%, la de la preeclampsia fue del 8.0%, seguida de la hipertensión gestacional con el 4.7%. Del total de gestantes con preeclampsia, el 54.8% fueron graves y el 11.9% fue de inicio temprano. Además, el 56.5% de las gestantes con preeclampsia severa tuvieron partos prematuros. La RCIU tuvo una prevalencia del 5.3%. Según los antecedentes maternos, los factores de riesgo más relevantes fueron los antecedentes familiares y personales de preeclampsia y RCIU.
CONCLUSIONES: se encontró una prevalencia considerable de preeclampsia con un alto porcentaje de partos prematuros, asociada a una severidad variada. Estos datos ayudan a los profesionales de la salud a conocer los factores de riesgo que se pueden monitorear para prevenir complicaciones. La determinación del riesgo de desarrollar un trastorno hipertensivo durante el embarazo es fundamental para fomentar el asesoramiento y la atención adecuados para estas mujeres durante la gestación.
Palavras-chave:
Preeclampsia, Hipertensión inducida por el embarazo, Restricción del crecimiento intrauterino, Factores de riesgo, Prevalencia, Resultados del embarazo
IntroductionHypertensive disorders during pregnancy need to be effectively treated promptly to prevent complications in the mother-child dyad.
1 Preeclampsia is an important cause of morbidity and mortality in maternal and perinatal populations.
2-4 It affects about 2-3% of all pregnancies in developed countries, causing 18% of maternal deaths and approximately 40% of fetal mortality.
2,5 The prevalence of preeclampsia in emerging countries is higher, about 6-8%.
1 Additionally, it leads to preterm deliveries, is associated with intrauterine growth restriction (IUGR), and increases the risk of severe complications.
6,7Preeclampsia is the primary cause of maternal morbidity and mortality in Colombia and the second cause in Bogotá. Mortality associated with hypertensive disorders, mainly preeclampsia and eclampsia, was 12.2% in 2012 and 25% in 2013 in Bogotá.
4,8,9 The incidence in Colombia has varied, between 3% and 14% depending on the city.
Multiple groups are working worldwide to research and design guidelines to improve the management of hypertensive disorders to reduce this problem.
8,10 All follow their patients by using maternal history and demographic characteristics
10 or assessing biophysical and biochemical markers,
11 which is necessary for evaluating the risk of developing hypertensive disorders during pregnancy.
The objective of this study was to determine the prevalence of hypertensive disorders and to describe the sociodemographic aspects and risk factors for preeclampsia, gestational hypertension and intrauterine growth restriction in a high-risk population.
MethodsThis descriptive study based on a prospective cohort was done including the pregnant women of the following three main institutions at Bogotá-Colombia, Ecodiagnóstico El Bosque Diagnostic Unit Centre, Fundación Salud Bosque - Clínica El Bosque, and South West Health Services Unit-Hospital Occidente de Kennedy.
To determine the sample size, sensitivity–89% (CI95%=69.8-97.4); with an error of 5% and a statistical power of 95%, was determined
12-14 by combining the pulsatility index of the uterine artery with newer serological tests. This resulted in a sample size of 434 patients. With the addition of a margin of error of 20%, a total of 566 patients were enrolled. Patients were selected based on admission to the gynecology-obstetrics service, taking into account eligibility criteria.
Between October 2014 and May 2018, 566 pregnant women were studied at 11-14 weeks of pregnancy with a fetal crown-rump length (CRL) of 45 to 84 mm. Twin pregnancies (n=6) and women without known maternal and perinatal outcomes (n = 33) were excluded. In total, 527 women were analyzed.
Medical history was taken at the time of admission to the study with attention being paid to hypertension and IUGR risk factors.
Maternal data included age, racial origin (Caucasian, Afro-Caribbean, Asian, or mixed), economic level (low, medium, or high), smoking habits, method of conception, obesity, personal chronic pathologies (hypertension, systemic lupus erythematosus, renal pathology, antiphospholipid syndrome, chronic kidney disease, and pre–gestational or gestational diabetes mellitus), and a personal and family history of preeclampsia and IUGR. An obstetrical history including parity, paternity, and a history of miscarriage was recorded.
2,15,16The outcomes associated with hypertensive disorders, IUGR, management of delivery, and the newborn’s clinical course, were collected from clinical records.
The following definitions were used:
Gestational Hypertension: Onset of high blood pressure after 20 weeks of pregnancy, without proteinuria.
6Preeclampsia: Obstetric disease with systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg when obtained at least 2 times more than 4 hours apart, in pregnant women over 20 weeks of gestation, without a history of chronic hypertension, and proteinuria ≥0.3 g on 24 hours collection or a protein/creatinine ratio ≥0.3 and the absence of any criteria of severe preeclampsia (any symptoms that indicated organ damage or blood pressure ≥160/110).
6,15,17Early preeclampsia: Preeclampsia with an onset at<34 weeks of gestation.
18Late preeclampsia: Preeclampsia with an onset ≥34 weeks of gestation.
18IUGR: Fetal or neonatal weight below the 10
th percentile for gestational age
7,19 associated with Doppler Feto-placentary signs of hemodynamic fetal redistribution secondary to altered circulatory flow or weight below the 3rd percentile for gestational age.
20,21Written informed consent was obtained from all participants. The Ethical Committee of Universidad El Bosque approved the study. Ethical principles for human research based on the Helsinki Declaration and Colombian Resolution 8430 of 1993 were followed in this study, and it was classified as an investigation with minimal risk.
22,23 The privacy of each patient was respected throughout the study.
The prevalence of each hypertensive disorder was calculated by determining the frequency of the various diagnoses and calculating its percentage of the total study population. The clinical and epidemiological variables were determined, and confidence intervals were estimated.
Descriptive statistics, categorical variables, and measures of central tendency for ratio variables were used. The statistical analysis was carried out using SPSS version 25.
ResultsA total of 566 pregnant women were enrolled between 11 and 14 weeks of pregnancy with a fetal CRL of 45 to 84mm. Twin pregnancies (n=6) and patients without documentation of maternal and perinatal outcomes (n=33) were excluded. In total, 527 patients were analyzed.
The average gestational age upon presentation was 12.7±0.69 weeks, the mean maternal age was 27.4±6.4 years, 97.3% were of mixed race, and 49.0% (n=258) were at a medium socioeconomic level, whereas 46.7% (n=246) were of low socioeconomic level. The socioeconomic level has been described as one of the main factors placing a woman at risk for preeclampsia.
3Of the women, 8.9% were obese, whereas 9.5% were of low weight. Overall, 6.6% had hypothyroidism, 3.0% had gestational diabetes, 2.1% had chronic hypertension, and 1.9% were anemic (Table 1). Additionally, 8.4% of the women smoked and 3.6% had other exposure to toxic materials.
Of the women, 36.2% were primigravid, and 63.8% were multigravid. Of the multigravid women, this pregnancy represented primipaternity in 38.7%. Additionally, 27.8% had a history of abortion before the 16
th week of gestation and 2.1% between the 16
th and 23
rd week of gestation.
A total of 20.5% had a family history of preeclampsia, 12.5% had a personal history of preeclampsia, and 8.3% and 6.5% had a family history and a personal history of IUGR, respectively (Table 1). These are recognized as risk factors for developing preeclampsia and IUGR.
4,6,16Hypertensive disorders are considered to be a significant cause of maternal and perinatal morbidity and mortality, and it is still challenging to be able to detect high–risk pregnancies.
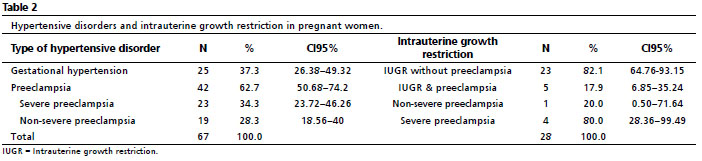
4,18,24 It was found a 12.7% prevalence of hypertensive disorders in our population. The most common hypertension disorders etiology was preeclampsia, 62.7%, with a prevalence of 8.0%, followed by gestational hypertension, 37.3%, with a prevalence of 4.7% (Table 2).
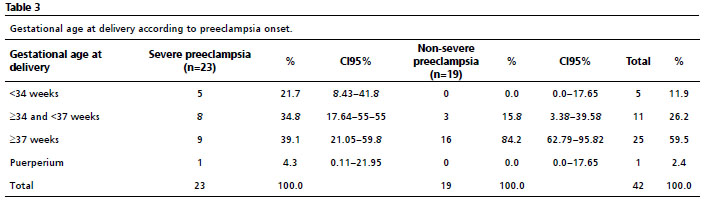
Among the women with preeclampsia (62.7%), 34.3% had severe preeclampsia and 28.3% had non-severe preeclampsia, and there were no cases of eclampsia (Table 3). Along with pre-eclamptic mothers (severe and non-severe) had preterm delivery in 38.1% of cases and full-term delivery in 61.9%. Of all of the severely pre-eclamptic mothers, 56.5% delivered preterm, whereas 15.8% of the mothers with non-severe preeclampsia delivered preterm.
It was found that of the 11 women in our study with a history of chronic hypertension, four of them developed preeclampsia (36.4%). Panaitescu
et al.
25 noted that a history of chronic hypertension, which is present in 1-2% of pregnancies, increased the risk of developing preeclampsia by 5-6 times. Panaitescu
et al.
25 also noted that it is possible that women with chronic hypertension had endothelial dysfunction before pregnancy, which could lead to the development of preeclampsia without impaired placentation, just by having this risk factor.
HELLP syndrome was diagnosed in just one of the pregnant women, with a prevalence of 0.2% and 4.3% of the severe preeclampsia group.
Early onset preeclampsia, <34 weeks, occurred in 11.9% of our pregnant women, with 88.1% developing it at 34 weeks of gestation or later (Table 3). Early onset preeclampsia is associated with preterm delivery before 34 weeks of gestation. However, we found a significant group of women who developed preeclampsia between 34 and 37 weeks, considered to be an intermediate group, which also has an increased risk of adverse outcomes due to preterm delivery.
5,18Moreover, severe preeclampsia concomitant with early onset is two critical factors that lead to pregnancies in a frame mark of high risk. In this group this situation has carried to 21.7% of preterm deliveries, therefore these data determine an essential public health problem requiring more efforts at prevention.
Another important outcome is IUGR (Table 2), which was diagnosed in 28 women with a prevalence of 5.3%. It was found that 17.9% of these pregnancies with IUGR also had preeclampsia. One corresponding to no severe and four of them severe.
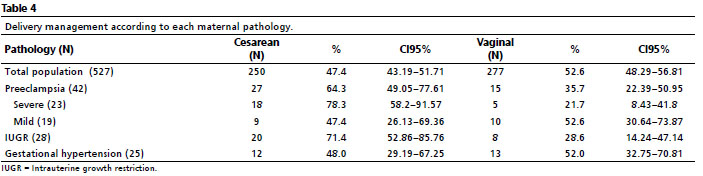
Table 4 notes the distribution of type of delivery by maternal pathological condition. Of all deliveries, 52.6% were vaginal and 47.4% were by cesarean section. Cesarean section was more common when preeclampsia and IUGR were present, 64.3% and 71.4%, respectively.
Of the newborns, 46.1% were female and 53.5% were male. There was one female stillbirth (0.2%) with a diagnosis of IUGR that took place during the 29
th week. There were no neonatal deaths reported. IUGR is known to increase the risk of intrauterine and neonatal death, with a 1.5% risk of death when the fetal weight is less than the 10
th percentile, and 2.5% when it is less than the 5
th percentile.
7Of the 527 newborns, the average weight was 2994.4g (850-4300g). The newborns of the women with preeclampsia had an average weight of 2688g (1320-4059g), in the IUGR it was 2139g (850-2900g), and for gestational hypertension the newborn’s average weight was 2966.4 g (2156-3720g).
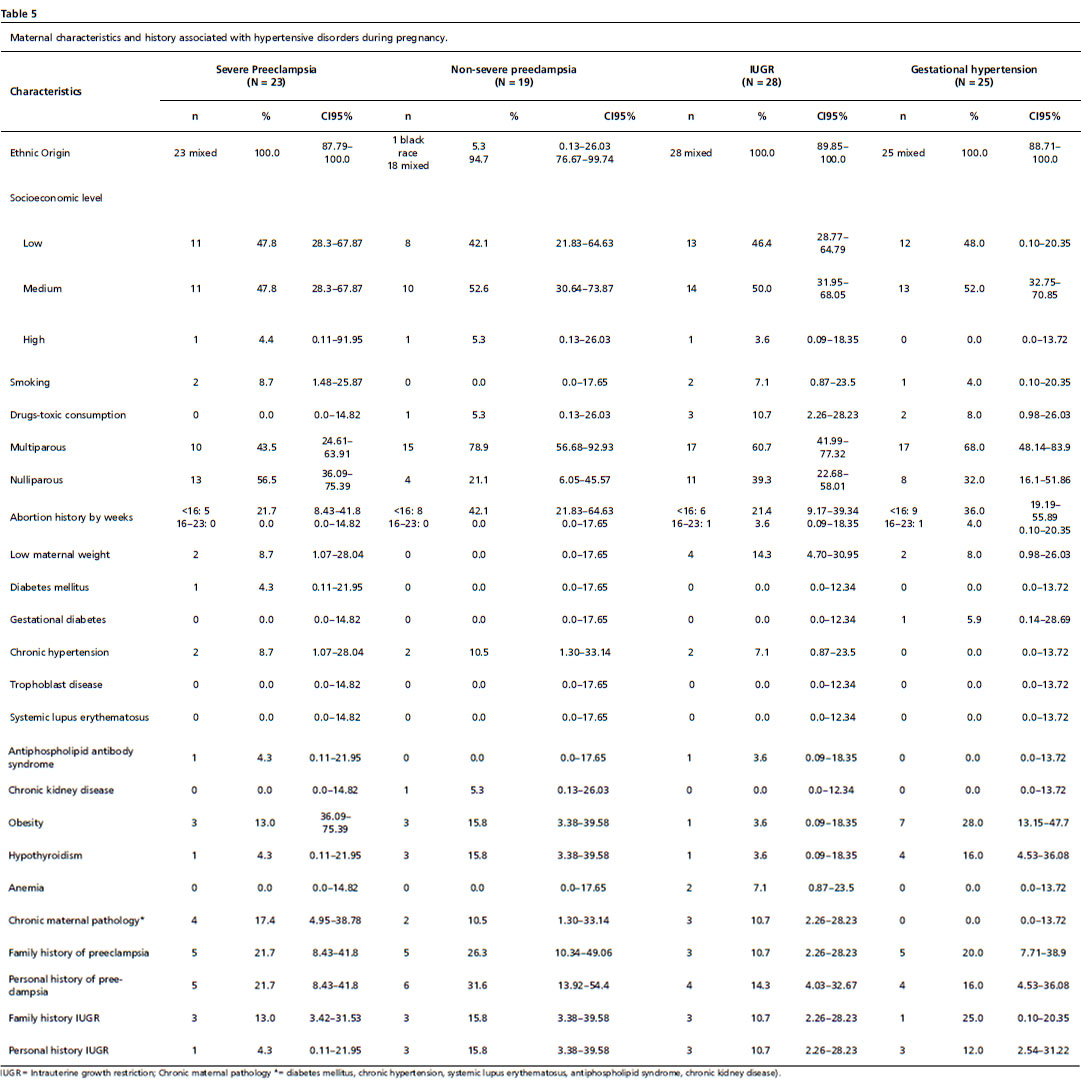
Table 5 details maternal demographic data stratified by types of hypertensive disorders. Mothers with severe preeclampsia were 27.26±6.2 years of age on average (CI95%=23.2-29.1) and entirely of mixed race, and 47.8% and 47.8% were from low and medium socioeconomic status, respectively. Of these mothers, 21.7% had an abortion before the 16
th week and 21.7% had both a personal and family history of preeclampsia. A total of 13.0% had a family history of IUGR, 13.0% were obese, 8.7% had chronic hypertension, and 8.7% were of low weight.
The average age for those with non-severe preeclampsia was 30.47±4.5 years (CI95%=29.8-32.5), and 94.7% were of mixed race. Of these mothers, 42.1% and 52.6% were of low and of medium socioeconomic status, respectively; 78.9% of this group were multiparous and 42.1% had a history of abortion before 16 weeks. A total of 31.6% and 26.3% had a personal and family history of preeclampsia, respectively. In addition, 15.8% had a personal and family history of IUGR, 15.8% were obese, 15.8% had hypothyroidism, and 10.5% had chronic hypertension.
The average age of mothers with an IUGR fetus was 27.14±2.1 years (CI95%=24.3-31.5), and all were of mixed race. A total of 46.4% and 50.0% were from a low and medium socioeconomic level, respectively; 60.7% were multiparous, and 21.4% had a history of abortion before 16 weeks. There was a history of toxic consumption in 10.7% of this group; there was a personal history of preeclampsia in 14.3%, and low weight occurred in 14.3%. In this group, there was an incidence of 10.7% for a family history of preeclampsia, a personal history of IUGR, and a family history of IUGR. Last, 7.1% of this group were anemic, and 7.1% had chronic hypertension.
Finally, the average age for the group with gestational hypertension was 27.39±3.2 years (CI95%=26.5-31.2), and all were of mixed race. Of this group, 48.0% and 52.0% were from a low and medium socioeconomic level, respectively. A total of 68.0% were multiparous, and 36.0% had a history of abortion before 16 weeks. Additionally, 28.0% of this group were obese, and 16.0% had hypothyroidism. There was a 20.0% and 16.0% incidence of a family and personal history of preeclampsia, respectively, and a 25.0% and 12.0% incidence of a family and personal history of IUGR, respectively.
DiscussionDetermining the risk of developing a hypertensive disorder during pregnancy is challenging.
3 The main objective in classifying patients is to be able to intervene and prevent or delay the onset of preeclampsia, thereby reducing maternal and perinatal complications.
5,6,18 Maternal history and demographic factors provide essential information on the mother’s clinical status and are major determinants of risk.
3,8,26 Therefore, these aspects of maternal history must be elucidated at the first prenatal visit at 11-14 weeks of gestation.
2One of the main findings in this study was the high percentage of mothers of low and medium socioeconomic levels, which has previously been described to be a risk factor for preeclampsia.
3 Also, we found disorders of weight to be frequent, and obesity has been described as a primary risk factor for hypertensive disorders, preeclampsia, and IUGR.
4,16,18 Fuchs
et al.
27 noted that increasing body mass index was associated with higher rates of hypertensive disorders, especially preeclampsia of all levels of severity. Another frequent finding was gestational diabetes, which also increased the risk for preeclampsia. It has been previously described that resistance to insulin and endothelial dysfunction is present in both gestational diabetes and preeclampsia.
28The prevalence of hypertensive disorders in our group was 12.7%, which is higher than world data references, but similar to other data in a Colombian population.
4,8,9 Preeclampsia (8.0%) was the most frequent type of hypertensive disorder followed by gestational hypertension with a prevalence of 4.7%. This is similar to findings in other countries in development, indicating that ongoing efforts to prevent preeclampsia are necessary.
3The early onset of preeclampsia is important due to its complications and severity, and it is known to be diagnosed in 1% of pregnancies.
14,18 Our prevalence of 1.5% is higher than previously described. This means that a substantial percentage of pregnant women will be at higher risk of maternal and perinatal adverse outcomes,
18 and efforts should be made to identify them at their initial obstetrical visit at 11-14 weeks.
11The significant prevalence of preeclampsia and a high percentage of preterm deliveries especially associated with severe preeclampsia that we found represents a major public health issue. Moreover, it has been described that preeclampsia is a risk factor for multiple fetal complications especially prematurity.
29 For that reason, it is imperative to continue developing strategies to avoid these unfavorable outcomes.
The overall IUGR prevalence was 5.3% and we found preeclampsia in 17.9% of mothers with IUGR. It must be taken into consideration, that this pathology in association with preeclampsia is a close sign of it. It has been noted that preeclampsia can lead to severe forms of IUGR and that both pathologies may lead to significant complications.
30Finally, previous studies have delineated risk factors for hypertension in pregnancy generally, but none, to our knowledge, have investigated the factors for each type of hypertensive disorder, as we do.
3,4,15,16 We found the primary risk factors for hypertensive disorders of pregnancy were low and medium socioeconomic level, obesity, chronic hypertension, and hypothyroidism, as well as a personal and family history of preeclampsia and a personal and family history of IUGR. We found that maternal age, nulliparity, and ethnic origin were not as high-risk as previously described.
2,15,16 Most of the women who developed any of these pathologies noted were multiparous (63.8%). The risk factors for our population are diverse, and many of the women who developed hypertensive disorders had none of the risk factors described in the literature, even though they had common risk factors such as obesity, chronic hypertension, or a history of preeclampsia and IUGR.
2,15,16As it has been described that there is little information on the epidemiology, maternal characteristics and risk factors for hypertensive disorders in a population of developing countries. Usually, the data offered is associated with preeclampsia as it is known worldwide but, there is a lack of this information concerning IUGR and gestational hypertension. Therefore, the strength of this article is that for the first time they are evaluated at the same time in a high-risk population and reported separately. Additionally, a selection limitation was observed, and it was minimized by clearly describing the study population’s characteristics.
In conclusion, the prevalence of hypertensive disorders in this population was higher than worldwide especially for preeclampsia, associated with a high percentage of preterm deliveries. Additionally, this population is characterized by having varied onset and severity of hypertensive disorders. The determination of the risk for developing hypertensive disorders is fundamental for giving appropriate prenatal care. It also provides the opportunity to initiate appropriate interventions to reduce complications and delay the onset of hypertensive disorders, over all in preeclampsia.
AcknowledgmentsThis study was conducted with the support of El Bosque Research Group of Maternal Fetal Medicine and Gynecology, Ecodiagnóstico El Bosque S. A. S (PMMFGEB-011), Universidad El Bosque (PCI-2013-472), Fundación Salud Bosque - Clínica El Bosque, and South West Health Services Unit-Hospital Occidente de Kennedy..
References1. Ghulmiyyah L, Sibai B. Maternal mortality from preeclampsia/eclampsia. Semin Perinatol. 2012 Feb; 36 (1): 56-9.
2. Garcia-Tizon Larroca S, Tayyar A, Poon L, Wright D, Nicolaides KH. Competing risk model in screening for preeclampsia by biophysical and biochemical markers at 30-33 weeks’ gestation. Fetal Diagn Ther. 2014; 36 (1): 9-17.
3. Poon LC, Nicolaides KH. First-trimester maternal factors and biomarker screening for preeclampsia. Prenat Diagn. 2014 Jul; 34 (7): 618-27.
4. Secretaría Distrital de Salud de Bogotá (CO). Guía de trastornos hipertensivos del embarazo. Bogotá: Alcaldia Mayor de Bogotá DC: SDS; 2014. [access in 2020 Jul 29]. Available from:
http://www.saludcapital.gov.co/DDS/Publicaciones/Guia%20Maternidad-Trastornos_baja.pdf5. Agarwal R, Chaudhary S, Kar R, Radhakrishnan G, Tandon A. Prediction of preeclampsia in primigravida in late first trimester using serum placental growth factor alone and by combination model. J Obstet Gynaecol. 2017 Oct; 37: 877-82.
6. American College of Obstetricians and Gynecologists (ACOG). Task Force on Hypertension in Pregnancy. Washington, DC: ACOG; 2013. [access in 2020 Jul 29]. Available from:
http://www.spog.org.pe/web/phocadownloadpap/HypertensioninPregnancy.pdf7. America College of Obstetricians and Gynecologists Committee on Practice Bull – Obstetrics and Society for Maternal-Fetal Medicin. ACOG Practice Bulletin Nº 204: Fetal Growth Restriction. Obstet Gynecol. 2019 Feb; 133 (2): e97-e109.
8. Romero XC, Gutierrez AM, Rojas NA, Ramirez A, Aldana J, Eslava M,
et al. Incidencia de los trastornos hipertensivos en el embarazo, y características clínico-demográficas en tres instituciones en Bogota, DC, Colombia. Investig Segur Soc Salud. 2018; 20: 21-30.
9. Uriel M, Romero XC. Reality of Preeclampsia in Colombian Pregnant Women. J Gynecol. 2016; 1 (1): 000105.
10. Brown MA. Pre-eclampsia in 2014: Seven ways to make a difference. Pregnancy Hypertens. 2014 Oct; 4 (4): 249-52.
11. Nicolaides KH. A Model for new pyramid of prenatal care based on the 11 to 13 weeks’ assessment. Prenat Diagn. 2011 Jan; 31 (1): 3-6.
12. Poon LC, Akolekar R, Lachmann R, Beta J, Nicolaides KH. Hypertensive disorders in pregnancy: screening by biophysical and biochemical markers at 11–13 weeks. Ultrasound Obstet Gynecol. 2010 Jun; 35 (6): 662-70.
13. Wortelboer EJ, Koster MH, Kuc S, Eijkemans MJC, Bilardo CM, Schielen PCJI,
et al. Longitudinal trends in fetoplacental biochemical markers, uterine artery pulsatility index and maternal blood pressure during the first trimester of pregnancy. Ultrasound Obstet Gynecol. 2011 Oct; 38 (4): 383-8.
14. Espinoza J, Romero R, Kae Nien J, Gomez R, Kusanovic JP, Goncalves LF,
et al. Identification of patients at risk for early onset and/or severe preeclampsia with the use of uterine artery Doppler velocimetry and placental growth factor. Am J Obstet Gynecol. 2007 Apr; 196 (4): 326.e1-13.
15. Ong CY, Liao AW, Cacho AM, Spencer K, Nicolaides KH. First-trimester maternal serum levels of placenta growth factor as predictor of preeclampsia and fetal growth restriction. Obstet Gynecol. 2001 Oct; 98 (4): 608-11.
16. O’Gorman N, Wright D, Poon LC, Rolnik DL, Syngelaki A, De Alvarado M,
et al. Multicenter screening for pre-eclampsia by maternal factors and biomarkers at 11-13 weeks’ gestation: comparison with NICE guidelines and ACOG recommendations. Ultrasound Obstet Gynecol. 2017 Jun; 49 (6): 756-60.
17. Ministerio de Salud (CO). Guias de practica clinica para la prevención, detección temprana y tratamiento de las complicaciones del embarazo, parto o puerperio. Colombia; 2013. [access in 2020 Jul 29]. Available from:
https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/INEC/IETS/Gu%C3%ADa.completa.Embarazo.Parto.2013.pdf18. Poon LC, Nicolaides KH. Early prediction of preeclampsia. Obstet Gynecol Int. 2014 Jul; 2014: 297397.
19. Blue NR, Beddow ME, Savibi M, Katukari VR, Mozurkewich EL, Chao CR. A comparison of methods for the diagnosis of fetal growth restriction between the royal college of obstetricians and gynecologists. Obstet Gynecol. 2018 May; 131 (5): 835-41.
20. Figueras F, Gratacòs E. Update on the diagnosis and classification of fetal growth restriction and proposal of a stage-based management protocol. Fetal Diagn Ther. 2014; 36 (2): 86-98.
21. Karagiannis G, Akolekar R, Sarquis R, Wright D, Nicolaides KH. Prediction of small-for-gestation neonates from biophysical and biochemical markers at 11-13 weeks. Fetal Diagn Ther. 2010; 29 (2): 148-54.
22. World Medical Association (WMA). WMA Declaration of Helsinki- Ethical Principles for Medical Research Involving Human Subjects. Adopted by the 18
th WMA General Assembly, Helsinki, Finland, June 1964; 2018. [access in 2020 Jul 29]. Available from:
https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/23. Ministerio de Salud (CO). Resolución Nº 8430, de Octubre 4 de 1993. Por la cual se establecen las normas científicas, técnicas y administrativas para la investigación en salud. [access in 2020 Jul 29]. Available from:
https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/DE/DIJ/RESOLUCION-8430-DE-1993.PDF24. Conde-Agudelo A, Belizán JM. Risk factors for preeclampsia in a large cohort of Latin American and Caribbean women. BJOG. 2000 Jan; 107 (1): 75-83.
25. Panaitescu AM, Akolekar R, Kametas N, Syngelaki A, Nicolaides KH. Impaired Placentation in Women with chronic hypertension who develop pre-eclampsia. Ultrasound Obstet Gynecol. 2017 Oct; 50 (4): 496-500.
26. Tsiakkas A, Duvdevani N, Wight A, Wright D, Nicolaides KH. Serum placental growth factor in the three trimesters of pregnancy: effects of maternal characteristics and medical history. Ultrasound Obstet Gynecol. 2015 May; 45 (5): 591-8.
27. Fuchs F, Senat MV, Rey E, Balayla J, Chaillet N, Bouyer J,
et al. Impact of maternal obesity on the incidence of pregnancy complications in France and Canada. Sci Rep. 2017 Sep; 7: 10859.
28. Ostlund I, Haglund B, Hanson U. Gestational diabetes and preeclampsia. Eur J Obstet Gynecol Reprod Biol. 2004 Mar; 113 (1): 12-6.
29. Ahumada JS, Barrera AM, Canosa D, Cardenas L, Uriel M, Ibáñez EA,
et al. Factores de riesgo de parto prematuro en Bogotá, Colombia. Rev Fac Med. 2020; 68 (4): 556-63.
30. Srinivas SK, Edlow AG, Neff PM, Sammel MD, Andrela CM, Elovitz MA. Rethinking IUGR in preeclampsia: dependent or independent of maternal hypertension? J Perinatol. 2009 Oct; 29 (10): 680-4.
Received on October 6, 2020
Final version presented on June 7, 2021
Approved on March 28, 2022
Author’s contributionRomero XC: Protocol/project development, data collection and management, data analysis, manuscript writing/editing. Montserrat U: Protocol/project development, data collection and management, data analysis, manuscript writing/ editing. Porras Ramírez A: data management, data analysis. Eslava M: Protocol/project development, data collection. Ramirez A: Protocol/project development, data collection. Franco SR: Protocol/project development, data management, data analysis, manuscript writing/editing. Forero CA: Protocol/project development, data collection.
The authors declare no conflicts of interest


 ; Uriel Montserrat2
; Uriel Montserrat2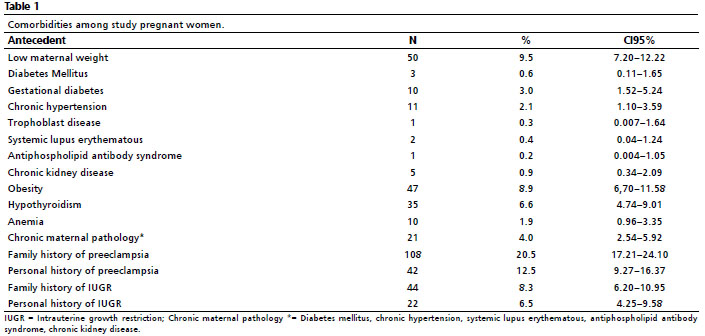






 Ler em português
Ler em português