ABSTRACT
OBJECTIVES: to analyze abortions provided by law (APL) carried out in Brazil between 2010 and 2019 regarding the need for travel of users, as well as the expenditure of time and money on these trips.
METHODS: descriptive study of records of outpatient care and hospitalizations for APL between 2010 and 2019. The municipal provision and the inter-municipal flows for the realization of the APL, the availability of public transportation for this travel, as well as its cost and time, were identified.
RESULTS: 2.6% of Brazilian municipalities had a sustained provision of APL between 2010 and 2019. Of the 15,889 APL performed, 14.8% occurred in municipalities other than those where the user lived. The smaller the population size of the municipality of residence, the higher the percentage of the need for travel. Of these inter-municipal trips, 16.0% had regular round-trip links by public transport. The total travel time ranged from 26 minutes to 4 and a half days, and the cost from R$2.70 to R$1,218.06; the highest medians were among residents of the Midwest region.
CONCLUSIONS: the concentration of services, the deficiency of inter-municipal public transport, and the expenditure on travel to access the APL are barriers to users that need the health service, demanding public policies to overcome them.
Keywords:
Health services accessibility, Legal abortion. Equity in access to health services, Reproductive health services
RESUMO
OBJETIVOS: analisar as restrições aos abortos previstos em lei (APL) realizados no Brasil entre 2010 e 2019 quanto à necessidade de deslocamento das usuárias, bem como quanto ao dispêndio de tempo e dinheiro nessas viagens.
MÉTODOS: estudo descritivo dos registros de atendimentos ambulatoriais e internações para APL entre 2010 e 2019. Foram identificados a oferta municipal e os fluxos intermunicipais para realização dos APL, a disponibilidade de transporte coletivo para esse deslocamento, bem como seu custo e tempo.
RESULTADOS: 2,6% dos municípios brasileiros tiveram oferta sustentada de APL entre 2010 e 2019. Dos 15.889 APL realizados, 14,8% se deram em municípios diferentes daqueles de residência da usuária. Quanto menor o porte populacional do município de residência, maior o percentual com necessidade de viajar. Desses deslocamentos intermunicipais, 16,0% tinham ligações regulares de ida e retorno em transporte público. O tempo de viagem total variou de 26 minutos a quatro dias e meio, e o custo de R$ 2,70 a R$ 1.218,06; as maiores medianas estiveram entre as residentes da região Centro-Oeste.
CONCLUSÕES: a concentração de serviços, a deficiência de transporte público intermunicipal, bem como o dispêndio com a viagem para acesso ao APL são barreiras às usuárias que precisam do serviço de saúde, demandando políticas públicas para sua superação.
Palavras-chave:
Acesso aos serviços de saúde, Aborto legal, Equidade no acesso aos serviços de saúde, Serviços de saúde reprodutiva
IntroductionIt is estimated that 55.7 million abortions occurred annually in the world between 2010 and 2014, with more than 6.4 million in Latin America alone. Two of its sub-regions, South America and the Caribbean, had the highest abortion incidence rates in the world,
1 although this is illegal in most of these countries.
2 There is diversity in legislation in these sub-regions, ranging from countries where abortion is legal and without restrictions in the first trimester, as in Cuba, Uruguay, and Argentina, and others where it is totally prohibited, such as in the Dominican Republic and Suriname. Nevertheless, in most countries of the sub-regions, abortion is allowed only in exceptional situations. This last category includes Brazil, the largest and most populous country in the group.
2 In Brazil, since the Penal Code of 1940, abortion is not punishable in pregnancies resulting from rape or to save the life of the pregnant woman, and, since the decision of the Federal Supreme Court in 2012, in cases of anencephalic fetuses.
3 In these situations, the service is provided by the country’s Unified Health System (SUS – Portuguese acronym). Access to health services depends on their availability. Regarding abortion, the little availability can lead to delay of the procedure or even make it impossible due to the legal limits of gestational time.
4 The location of services is also fundamental. The increased distance between the house and the health unit decreases access to the service.
4–6 However, the barriers are beyond the distance, as they involve the transport possibilities, the time required, and the costs
4. Thus, as distance does not comprise the diversity of the territory, travel time is used as an indicator of accessibility. The greater demand for time implies the need for logistical arrangements that compromise secrecy and entail greater cost.
4The costs for performing the abortion include the value of the procedure itself, transportation, food, and overnight stay of the user and companion, care costs for dependents and loss of earnings for days not worked, which increase according to the travel time.
4 In Brazilian case, the user does not pay for the procedure carried out by SUS. Moreover, travel, food, and overnight stays should also be made possible by the State when procedure needs to be performed in another municipality that does not compose the same Metropolitan Region and is more than 50 km away from the municipality of residence of the user.
7It is known that in the country, there are few facilities with effective provision of abortion provided by law: between 2013 and 2015, there were 37 facilities, mostly in state capitals.
8 The limited availability of the service in territory may indicate the need for travel for access to abortion provided by law. Nevertheless, there is no information about this travel nor cost and time spent on these trips for people who undergo the procedure.
Expenditure on terminations points to a possible barrier to access to abortion provided by law in the country, which may be insurmountable to some groups. The impossibility of access to legal abortion leads to worse mental health outcomes for pregnant women,
9 as well as other health complications, including those resulting from unsafe terminations of pregnancy.
10 Thus, the feasibility of abortion provided by law makes up access to sexual and reproductive health services, as well as contributes to the reduction of maternal mortality, crossing at least two of the Brazilian goals for achieving Good Health and Well-being, the third of Sustainable Development Goals.
11 Given this context and considering that the implications of travel may prevent people from accessing health services, the present study seeks to draw an overview of the procedures performed between 2010 and 2019, outlining the need for travel and the estimated time and money spent with transportation to undergo abortion provided by law in Brazil.
MethodsThis is a descriptive cross-sectional study of travels for abortions provided by law. The records of outpatient care and hospitalizations between January 2010 and December 2019 in Brazil with the main diagnosis: ICD O04, were included. – “Abortion for medical and legal reasons” of people of childbearing age (10 to 49 years) with “Post-abortion curettage” or “Post-abortion uterine emptying by Intrauterine Manual Vacuum Aspiration (MVA)” procedures registered in the Outpatient Information System (SIA – Portuguese acronym) or the Hospital Information System (SIH – Portuguese acronym). The inclusion of only these procedures was due to their compatibility with the ICD according to the Table of Procedures, Medicines and Orthotics, Prosthetics, and Special Materials of the SUS. The databases are publicly accessible and made available for transfer by the SUS Department of Informatics (DATASUS - Portuguese acronym) of the Ministry of Health.
The variables that indicate the municipality of residence and the municipality where abortions provided by law were performed. The municipalities were located in the digital network of Brazil with a political-administrative division in force in the 2010 Census made available by the Brazilian Institute of Geography and Statistics (IBGE – Portuguese acronym). The location points of municipalities are related to the headquarters district, according to the registration of localities of IBGE also in 2010.
The municipalities where the abortions provided by law were conducted were categorized as to the stability of provisions, such as occasional provision, sporadic provision, and sustained provision. Municipalities with occasional provision are those that performed one procedure throughout the period, those with sporadic provision are those that performed less than one procedure per year as an average of the period (2 to 9 in the period), and those with sustained provision are those that performed at least one procedure per year as an average of the period (10 or more in the period).
The travel flows were drawn for the procedures that were not performed in the municipalities of residence of the users. Each line represents the travel of at least one user. The Flow plugin of the Terraview 4.2.2 software was used to represent the flows. The final map was prepared in the Qgis 3.10.7 software. The Geodetic Reference System for the Americas (SIRGAS – Portuguese acronym) 2000 was adopted.
After identifying the inter-municipal flows for carrying out the abortions provided by law, routes with link availability via public transport, their cost, and travel time were identified. For this, the 2016 research “Road and Waterway Links”
12 of the Brazilian Institute of Geography and Statistics (IBGE) was used as a source of information.
The research “Road and Waterway Links” presents all the inter-municipal road and waterway links in public transport, whether formal or informal, existing in Brazil in 2016. In the research, inter-municipal transport is not considered to occur in the same population arrangement, groups of municipalities with strong population integration. The study details the travel time and cost of existing links. It includes all Brazilian municipalities and the links with the following characteristics: open to the general public through the payment of a fare; between the headquarters of municipalities; with a pre-fixed place of departure, arrival, and the route; and with vehicle departures on certain days and times.
12Links related to inter-municipal travels outside population arrangements were searched in the research “Road and Waterway Links”.
12 Thus, it was described the existence or not of the link in public transport to and from the place of residence and abortion provided by law, as well as the time and cost of travel when the link existed. The round trip values were added together, finding the total cost and travel time. When only one of the links was found, one-way or return, the total time and cost were estimated considering that the round trip would require the same time and cost, that is, they were estimated by doubling values of the link found. As for the values, in 2016, the minimum monthly wage in the country was R$880.00 or US$412.56 when corrected for purchasing power parity based on GDP
13, the same correction used in the rest of the manuscript.
Finally, the time and cost of transportation by population size were described according to the 2010 Population Census
14 under the categories: up to 5,000 inhabitants, from 5,001 to 10,000, from 10,001 to 20,000, from 20,001 to 50,000, from 50,001 to 100,000, from 100,001 to 500,000, and more than 500,000 inhabitants; and region of residence of the user: North, Northeast, Southeast, South, Midwest.
ResultsA total of 15,889 procedures were performed in Brazil in 627 municipalities. Of the municipalities that registered the provision of the procedure, 251 (40%) had an occasional provision, with only 1 procedure during the entire decade, 233 (37.2%) had a sporadic provision, with less than 1 procedure per year, and 143 (22.8%) had a sustained provision, performing at least 1 procedure per year in the average of the period. The latter group, corresponding to 2.6% of the 5,565 Brazilian municipalities, concentrated 92.8% of abortions provided by law that occurred in the country in that decade. All Federative Units and regions had at least one procedure registered, ranging from 1 in Amapá, in the North of the country, to 3,646 in São Paulo, in the Southeast (Figure 1).
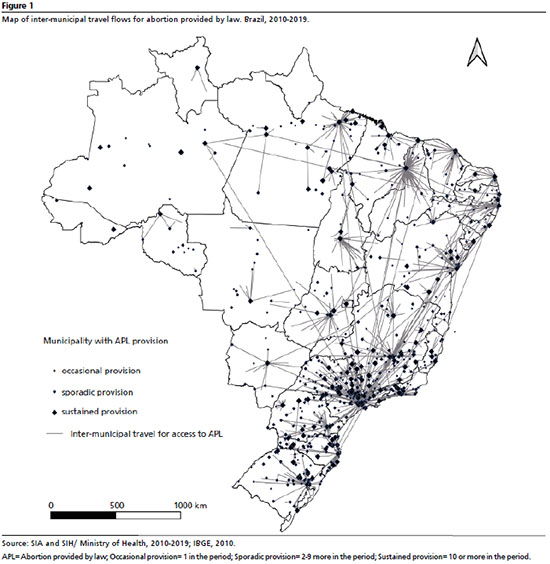
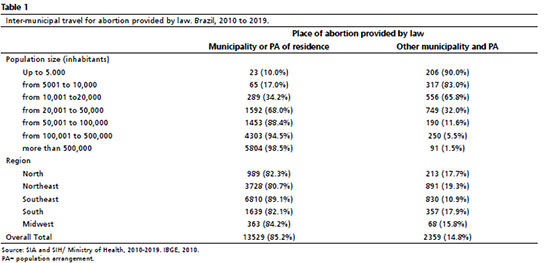
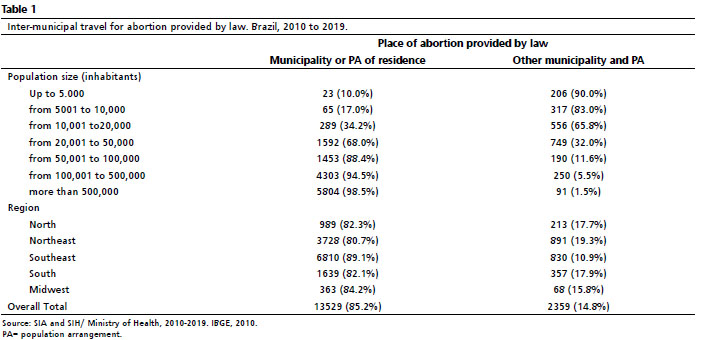
Although hospitalizations or care occurred in 627 (11.3%) of Brazilian municipalities, users who underwent the abortion provided by law procedure resided in 3,104 (55.7%) different municipalities. Of the total number of procedures, 11,721 (73.8%) were performed in the municipality of residence of the user and another 1,808 (11.4%) in different municipalities, but in the same population arrangement, totaling 13,529 procedures (Table 1). Another 2,218 (14.0%) procedures took place outside the municipality or population arrangement of the user’s residence but in the same Federative Unit, and 141 (0.9%) procedures took place in a Federative Unit different from that of the user’s residence; one of the records had no known municipality of residence. The travel flows are shown in Figure 1.
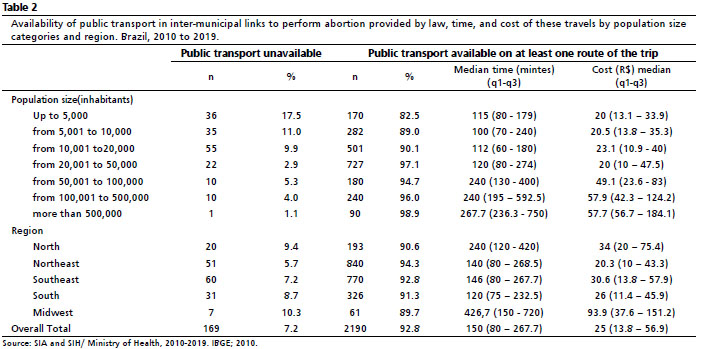
Of all 2,359 inter-municipal trips, 92.8% had public transport available in at least one of the trip routes (Table 2). However, round trips in transport open to the general public, between municipal headquarters, and with spatial and temporal regularity were present in only 16.0% of trips. Total travel time ranged from 26 minutes to 4 and a half days (6,444 minutes). The cost of the trip also has a wide range, from R$2.70 (US$1.27) to R$1,218.06 (US$571.05).
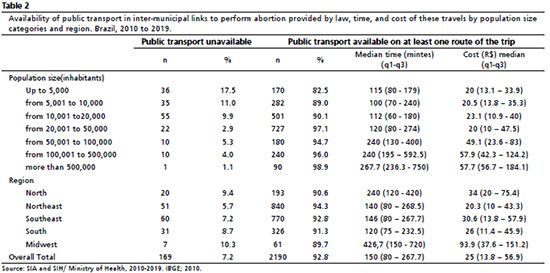
The percentage of people who needed inter-municipal transportation for abortions provided by law was higher among residents of smaller municipalities (Table 1), where the availability of inter-municipal public transport for this trip was lower (Table 2). The time and cost of trips to access the procedure were greater for those living in larger municipalities (Table 2). The travels made by residents of municipalities of up to 50,000 inhabitants had as their main destination (22.0%) Teresina, a capital in the Northeast of the country. Among the residents of municipalities with more than 50,000 inhabitants, the main destination (37.1%) was the city of São Paulo, a capital in the Southeast. Of inter-municipal trips of residents of municipalities between 100,001 and 500,000 inhabitants, 40.4% had São Paulo as their destination, and among residents of municipalities with more than 500,000 inhabitants, 74.7% had the same destination.
The region with the lowest need for travel was the Southeast (Table 1), where there was also a greater number of municipalities with the provision of abortion provided by law: 239. The lowest travel costs were in the Northeast region (Table 2), where 126 municipalities had abortions provided by law. The shortest travel times were in the South region (Table 2), where 145 municipalities provided the procedure. The North and Center-West regions had 71 and 43 municipalities with provision, respectively, and presented the highest expenses with travel. In the Midwest region, the median was more than 7 hours of round trip to the health facility with the provision of abortion provided by law, with a median cost of R$93.90 (US$44.00) (Table 2). The Center-West region was also the one with the lowest availability of public transport for trips (Table 2) and the one with the highest percentage of trips to the same municipality (47.1%), followed by the Northeast (46.8%), North (37.6%), Southeast (27.8%), and South (18.2%).
DiscussionBetween 2010 and 2019 there were an average of 1,589 abortions provided by law per year in Brazil, a country with almost 200 million inhabitants in 2010.
14 As a perspective, considering only one of the situations in which abortion is allowed in Brazil: at least 18,734 pregnancies were estimated to result from rape in the country in 2019.
15 That is, less than one in 11 pregnant women who could resort to abortion provided by law accessed it.
The abortions provided by law occurred mostly (92.8%) in the municipalities with the sustained provision of the procedure, a group of 143 municipalities that represent 2.6% of the total Brazilian municipalities, and another 484 municipalities had occasional or sporadic provision. Carrying out any abortion provided by law in the period, however, does not guarantee the permanent provision of the procedure, nor the provision for the three causes allowed in the country or at any gestational time since the services with the provision of the procedure establish their own limits of gestational time and causes served. Thus, the availability of the service varies depending on the cause and decreases with increasing gestational age.
8,15 Besides the potential delay in the procedure, the low availability of service and the consequent need for travel may prevent abortion due to gestational time, especially in pregnancies resulting from rape. Although the Penal Code of Brazil does not establish a limit gestational age for the non-punishability of abortion in these situations, the Ministry of Health presents in a technical standard the limit of 20 or 22 weeks.
16 Given that this standard is used as a reference for SUS services, few facilities perform an abortion in pregnancies resulting from rape with more than 22 weeks in the country.
15Although the procedures were concentrated in a small group of municipalities, most of abortions provided by law, 85.2%, occurred in residents of the same population arrangement, and 73.8% in residents of the same municipality. In 2016, when all hospitalizations in the country were analyzed, regardless of the reason for hospitalization, 67.3% had occurred in the municipalities of residence of users.
17 To this end, the high percentage of abortion provided by law in the municipality of residence of the user follows that found in hospitalizations as a whole due to population concentration and hospital resources in large cities.
18 Nevertheless, the small percentage of travels, even lower in cases of abortion provided by law, may point to non-access to services when unavailable in the municipality of residence of those who need them.
19 This hypothesis is corroborated by the finding that 74.7% of the abortions provided by law were carried out in residents of municipalities with more than 100,000 inhabitants. However, this group of municipalities concentrated only 54.7% of the Brazilian population,
14 which may indicate unequal access to the service.
The need for travel is a barrier to access to hospital care. In 2000, even distances of up to 20 km already decreased accessibility in Brazil.
19 Travel requires transportation, time, and financial resources,
4 which are not always available. Specifically regarding abortion, different countries point out that increasing the distance to the facility with the service provision reduces access to the safe procedure.
4–6 This factor leads to the search for other potentially dangerous ways to terminate pregnancy.
20 Distance is a more present barrier among young women, residents of rural areas, poor, non-white, and with more than 12 weeks of pregnancy.
4 Socially vulnerable are also those with fewer conditions to overcome the geographical barrier, especially non-whites and with low education.
5,21 The unavailability of transportation is in itself a possible barrier to access to health services. In the Brazilian case, 16.0% of the direct inter-municipal travel for abortion provided by law had round trips available in public transport by road or waterway, 76.8% of the travels had public transport available on one of the routes on the trip, and another 7.2% had none of the routes. The absence of a direct link in public transport by road or waterway makes it necessary to establish access alternatives. In this case, it would be imperative to use more than one public transport line or private or air transport, which can make the access of the poorest people more expensive and unfeasible, evidencing the need for sanitary transport provided by the State.
Among small municipalities, most people had to travel to access the abortion provided by law. The need for traveling among residents of larger municipalities was small. Nonetheless, when traveling was necessary, it required more time and money. These profiles reflect the exclusivity of abortion provision in services of higher technological density,
22 concentrating it in larger urban centers.
8 The need for travel among residents of larger municipalities, those that concentrate abortion provision, may be due to the search for specialized care. In the period analyzed, these travels were directed to São Paulo, the largest center that provides services of high technological density in the country.
23The travel time in the Center-West region was the longest among regions, pointing out the low capillarity of abortion provided by law service. The concentration of these services follows that of other procedures that require hospitalization in the region, which are mostly in the state capitals, without secondary health care centers, which, although with less intensity, is repeated in the northern region of the country.
23 The fastest inter-municipal travels were 20 minutes, while others took days. The increase in travel time entails greater logistical implications, with the need for arrangements for daily tasks, which commonly include care for dependents, work, and school, generating greater difficulty in maintaining confidentiality about the procedure and potential financial loss, depending on the employment relationship.
4Besides these expenses, direct costs are a burden for pregnant women who need to travel to access abortion, which includes transportation, accommodation, and meals for themselves and often for a companion.
4 In Brazil, SUS can bear these costs.
7 However, the amounts paid are R$3.70 (US$1.73) for every 27 nautical miles in river transport, R$4.95 (US$2.32) for every 50 km in land transport, or R$181.50 (US$85.09) for every 200 miles in air transport; as well as a daily rate of R$8.40 (US$3.94) for food or R$24.75 (US$11.60) for food and overnight accommodation.
24 These resources are subject to high and medium complexity financial limits and, when paid in the form of refund to the user, do not cover expenses.
25 This way, direct costs can continue configuring as a barrier to accessing the service.
As for the amounts spent exclusively on traveling, there was a variation of 0.3% to 138.4% of monthly minimum wage, that is, the amount related to six weeks of work (264 hours), in 2016 values, in Brazil may have been spent on transportation of a person. Thus, even though health care is free in the country, the financial expenditure on travel can be prohibitive to access when the State does not guarantee transport.
Besides the costs already mentioned, the losses arising from not obtaining access can also be considered. People who do not achieve the abortion provided by law are more likely to have mental health problems, with symptoms of anxiety, low self-esteem, and dissatisfaction with their own lives in the short term,
9 as well as being more likely to present life-threatening health events,
10 as well as the risk of terminating a pregnancy in an unsafe way, which can lead to death.
10,20Brazilian policy opts for the provision of abortion provided by law only in general hospitals, maternities, emergency rooms, emergency units, and emergency services.
22 However, the procedure could be safely provided in primary care until at least the 12th week of pregnancy
26,27 and via telehealth until the 10th week.
15,28 The capillarization of the provision through primary care and telehealth would reduce the need for travel, expanding access to the service and reserving the travels and beds only for situations in which there is in fact a need for hospital care for pregnancy termination.
Among the limitations of this study is the use of databases of information systems that aim to finance services by SUS, which does not include procedures performed in private services with direct payment or by health plans. In addition, as there is a limit of resources related to medium and high complexity to be paid to states and municipalities, there is a risk of underreporting of production that exceeds this limit. Likewise, there may be underreporting of production that diverges from quantitative agreements of procedures and flows in the Health Regions.Still, the databases used are national, with records of outpatient care and hospitalizations financed by SUS, whether in the public or private network.
29,30 Still regarding information systems, the diversity of contexts in which they are fed can weaken uniformity and quality. To minimize these problems, all facilities follow the same national regulations, and both systems have automatic validation mechanisms, blocking inconsistencies.
29,30 Including only the records with the main diagnosis “Abortion for medical and legal reasons” and those compatible procedures is appropriate to the systems’ regulations. Still, it may have excluded true records, especially of cases of risk to the pregnant woman’s life and fetal anencephaly. In addition, exclusively medical abortions are also not included in the records since they are not included as procedures in the SUS Table of Procedures, Medicines and Orthotics, Prosthetics, and Special Materials. These are weaknesses in the records used and may have underestimated the number of procedures performed in the country.
Concerning the travel time and cost information, the data used refer to 2016, and it is possible that the links found were not constant from 2010 to 2019. Even so, the use of data from the IBGE 2016 survey “Road and Waterway Links” is justified as the information of a straight-line distance or an automobile travel does not comprise the complexity and diversity of Brazilian contexts, with different reliefs, roads, or waterway qualities and available transport modalities.
The present study found a concentration of the provision of abortion provided by law in some municipalities of the country, little availability of round trip public transportation between the municipalities of residence and carrying out the procedure, as well as costs and travel times that reached prohibitive values considering the social reality of the country. Abortion, in situations provided by law, is a health service. It should be universally accessible, but the demand for time and money for travel can make it difficult or prevent part of those who need access to the service. It is understood, therefore, that restricting the provision of legal abortion to facilities of greater complexity and its concentration in large urban centers compromises the preservation of the dignity, life, and health of girls, women, and other potential pregnant women in Brazil.
AcknowledgmentsWe thank the
Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) for the financial support (Finance Code 001).
References1. Ganatra B, Gerdts C, Rossier C, Johnson BR Jr, Tunçalp Ö, Assifi A,
et al. Global, regional, and subregional classification of abortions by safety, 2010–14: estimates from a Bayesian hierarchical model. Lancet. 2017; 390 (10110): 2372-81.
2. Center for Reproductive Rights. The world’s abortion laws 2021. New York: Center for Reproductive Rights; 2021. [access in 2021 abr 20]. Available from:
https://reproductiverights.org/maps/worlds-abortion-laws/3. Brasil. Supremo Tribunal Federal. Arguição de Descumprimento de Preceito Fundamental 54. Distrito Federal. Relator Ministro Marco Aurélio. Julgado em 12/04/2012. Brasília (DF): Diário da Justiça; 2012. [access in 2021 abr 20]. Available from:
https://www.stf.jus.br/arquivo/cms/processoAudienciaPublicaAdpf54/anexo/adpf54audiencia.pdf4. Barr-Walker J, Jayaweera RT, Ramirez AM, Gerdts C. Experiences of women who travel for abortion: A mixed methods systematic review. Withers MH, organizador. PLoS ONE. 2019; 14 (4): e0209991.
5. Friedman J, Saavedra-Avendaño B, Schiavon R, Alexander L, Sanhueza P, Rios-Polanco R,
et al. Quantifying disparities in access to public-sector abortion based on legislative differences within the Mexico City Metropolitan Area. Contraception. 2019; 99 (3): 160-4.
6. Brown BP, Hebert LE, Gilliam M, Kaestner R. Distance to an Abortion Provider and Its Association with the Abortion Rate: A Multistate Longitudinal Analysis. Perspect Sex Repro H. 2020; 52 (4): 227-34.
7. Ministério da Saúde (BR). Portaria N
o 55, de 24 de Fevereiro de 1999. Dispõe sobre a rotina do Tratamento Fora de Domicílio no Sistema Único de Saúde - SUS, com inclusão dos procedimentos específicos na tabela de procedimentos do Sistema de Informações Ambulatoriais do SIA/SUS e dá outras providências. Brasília (DF): DOU de 1 de março de 1999. [access in 2021 abr 20]. Available from:
https://bvsms.saude.gov.br/bvs/saudelegis/sas/1999/prt0055_24_02_1999.html#:~:text=Disp%C3%B5e%20sobre%20a%20rotina%20do,SUS%20e%20d%C3%A1%20outras%20provid%C3%AAncias.8. Madeiro AP, Diniz D. Serviços de aborto legal no Brasil- um estudo nacional. Ciênc Saúde Colet. 2016; 21: 563-72.
9. Biggs MA, Upadhyay UD, McCulloch CE, Foster DG. Women’s Mental Health and Well-being 5 Years After Receiving or Being Denied an Abortion: A Prospective, Longitudinal Cohort Study. JAMA Psychiatry. 2017; 74 (2): 169.
10. Gerdts C, Dobkin L, Foster DG, Schwarz EB. Side Effects, Physical Health Consequences, and Mortality Associated with Abortion and Birth after an Unwanted Pregnancy. Women’s Health Issues. 2016; 26 (1): 55-9.
11. United Nations. Transforming our world: the 2030 Agenda for Sustainable Development; 2015. [access in 2021 abr 20]. Available from:
https://sustainabledevelopment.un.org/content/documents/21252030%20Agenda%20for%20Sustainable%20Development%20web.pdf12. Instituto Brasileiro de Geografia e Estatística (IBGE). Ligações rodoviárias e hidroviárias: 2016. Rio de Janeiro (RJ): IBGE; 2017. [access in 2021 abr 20]. Available from:
https://www.ibge.gov.br/geociencias/organizacao-do-territorio/redes-e-fluxos-geograficos/15794-rodoviarias-e-hidroviarias.html?=&t=acesso-ao-produto13. World Bank. Databank. Purchasing power parities (PPP) (US$=1), 2016. 2020. [access in 2021 abr 20]. Available from:
https://databank.worldbank.org/embed/ICP-Annual-PPPs/id/8b9dca71?inf=n14. Instituto Brasileiro de Geografia e Estatística (IBGE). Censo demográfico 2010. Características da população e dos domicílios: resultados do universo. Rio de Janeiro (RJ): IBGE; 2011. [access in 2021 abr 20]. Available from:
https://biblioteca.ibge.gov.br/visualizacao/periodicos/93/cd_2010_caracteristicas_populacao_domicilios.pdf15. Rosas CF, Paro HBMS. Serviços de atenção ao aborto previsto em lei: desafios e agenda no Brasil. Cfemea/ SPW; 2021. [access in 2021 abr 20]. Available from:
https://www.cfemea.org.br/index.php/pt/artigos-e-textos/4888-servico-de-atencao-ao-aborto-previsto-em-lei-desafios-e-agenda-no-brasil16. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Prevenção e tratamento dos agravos resultantes da violência sexual contra mulheres e adolescentes: norma técnica. 3
rd ed. Brasília (DF): Ministério da Saúde; 2012. [access in 2021 abr 20]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/prevencao_agravo_violencia_sexual_mulheres_3ed.pdf17. Xavier DR, Oliveira RAD, Barcellos C, Saldanha RF, Ramalho WM, Laguardia J,
et al. As Regiões de Saúde no Brasil segundo internações: método para apoio na regionalização de saúde. Cad Saúde Pública. 2019; 35 (Suppl. 2): e00076118.
18. Solla J, Chioro A. Atenção Ambulatorial Especializada. In: Políticas e sistema de saúde no Brasil; 2008. p. 627-64.
19. Oliveira EXG, Travassos C, Carvalho MS. Acesso à internação hospitalar nos municípios brasileiros em 2000: territórios do Sistema Único de Saúde. Cad Saúde Pública. 2004; 20: S298-309.
20. Ralph L, Foster DG, Raifman S, Biggs MA, Samari G, Upadhyay U,
et al. Prevalence of Self-Managed Abortion Among Women of Reproductive Age in the United States. JAMA Netw Open. 2020; 3 (12): e2029245.
21. Venator J, Fletcher J. Undue Burden Beyond Texas: An Analysis of Abortion Clinic Closures, Births, And Abortions in Wisconsin. Cambridge, MA: National Bureau of Economic Research; 2019 p. w26362. [access in 2021 abr 20]. Available from:
https://www.nber.org/system/files/working_papers/w26362/w26362.pdf22. Ministério da Saúde (BR). Portaria n
o 485, de 1
o de abril de 2014. Redefine o funcionamento do Serviço de Atenção às Pessoas em Situação de Violência Sexual no âmbito do Sistema Único de Saúde (SUS). Brasília (DF): DOU de 2 de abril de 2014. [access in 2021 abr 20]. Available from:
https://bvsms.saude.gov.br/bvs/saudelegis/gm/2014/prt0485_01_04_2014.html23. Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa Regiões de Influência das Cidades – informações de deslocamentos para serviços de saúde. Rio de Janeiro (RJ): IBGE; 2020. [access in 2021 abr 20]. Available from:
https://biblioteca.ibge.gov.br/visualizacao/livros/liv101715_notas_tecnicas.pdf24. Ministério da Saúde (BR). Gabinete do Ministro. Portaria n
o 2.848, de 6 de Novembro de 2007. Publica a Tabela de Procedimentos, Medicamentos, Órteses, Próteses e Materiais Especiais - OPM do Sistema Único de Saúde. Brasília (DF): DOU de 6 de novembro de 2007. [access in 2021 abr 20]. Available from:
https://bvsms.saude.gov.br/bvs/saudelegis/gm/2007/prt2848_06_11_2007.html25. Barbosa HHMM, Santos ALM, Cruz RAP, Borge RGL, Rodrigues Neto TS. Perfil dos pacientes atendidos pelo programa Tratamento Fora de Domicílio no Município de Belém, Estado do Pará, Brasil. Rev Pan-Amaz Saúde. 2010; 1 (3): 43-7.
26. Zhou J, Blaylock R, Harris M. Systematic review of early abortion services in low- and middle-income country primary care: potential for reverse innovation and application in the UK context. Global Health. 2020; 16 (1): 91.
27. World Health Organization (WHO). Safe abortion: technical and policy guidance for health systems. 2
a ed. Geneva: WHO; 2012. [access in 2021 abr 20]. Available from:
https://apps.who.int/iris/bitstream/handle/10665/173586/WHO_RHR_15.04_eng.pdf28. Endler M, Lavelanet A, Cleeve A, Ganatra B, Gomperts R, Gemzell-Danielsson K. Telemedicine for medical abortion: a systematic review. BJOG. 2019; 126 (9): 1094-102.
29. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Regulação, Avaliação e Controle. Coordenação Geral de Sistemas de Informação. SIA – Sistema de Informação Ambulatorial do SUS: Manual de Operação do Sistema. Brasília (DF): Ministério da Saúde; 2012. [access in 2021 abr 20]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/manual_tecnico_sistema_informacao_hospitalar_sus.pdf30. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Regulação, Avaliação e Controle. Coordenação Geral de Sistemas de Informação. SIH – Sistema de Informação Hospitalar do SUS: Manual Técnico Operacional do Sistema. Brasília (DF): Ministério da Saúde; 2017. [access in 2021 abr 20]. Available from:
http://sihd.datasus.gov.br/documentos/documentos_sihd2.phpReceived on August 27, 2021
Final version presented on February 28, 2022
Approved on June 7, 2022
Author’s contribution: Jacobs MG and Boing AC conceived the paper. Jacobs MG wrote the first version of the manuscript. Both authors worked on subsequent versions, approved the final version of the article and declared no conflict of the interest.


 ; Alexandra Crispim Boing2
; Alexandra Crispim Boing2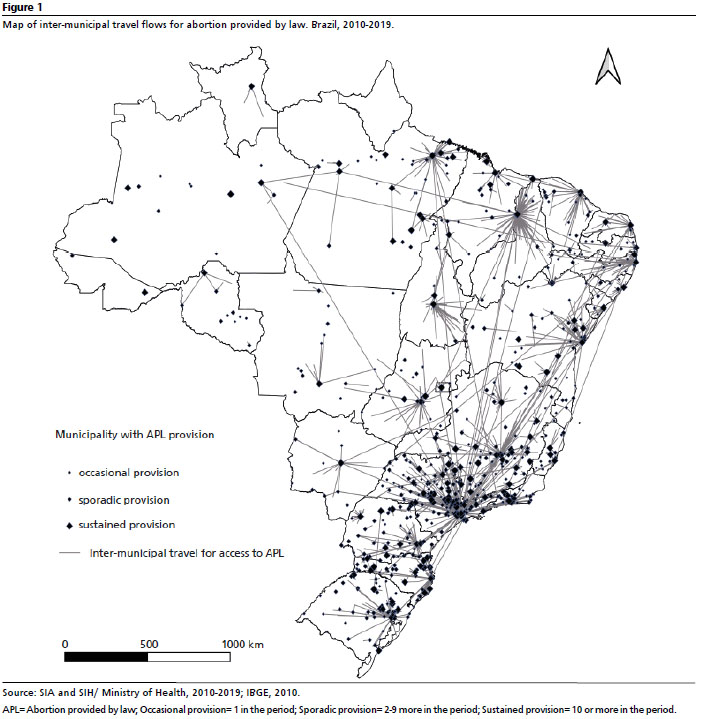






 Ler em português
Ler em português