ABSTRACT
OBJECTIVES: to describe the motor development, in the first two years of life, of children with evidence of congenital Zika virus syndrome (CZS) at birth and of children exposed to the Zika virus (ZIKV) during pregnancy, but without evidence of CZS.
METHODS: systematic review, according to the recommendations of the Preferred Reporting Items for Systematic Reviews (PRISMA). The search took place in the VHL/LILACS interface and BIREME/PubMed interface databases until March 2020. Two researchers analyzed the quality of the studies using the Johanna Briggs Institute methodology.
RESULTS: 21 articles were selected. Children with CZS have severe impairment of motor functions and a high prevalence of spastic cerebral palsy. At two years of life, most reached only early levels of motor development; with impaired vision, hearing, language, cognition, behavior, and social interaction. On the other hand, children exposed to ZIKV, but without evidence of CZS, are at lower risk, about 20% have late manifestations of delay and/or neurodevelopmental disorder. Variables associated with greater motor impairment are early maternal infection, preterm birth, lower head circumference, abnormal imaging, use of anticonvulsant, increasing age, arthrogryposis, epilepsy, deficits in vision, language, cognition, and lower income.
CONCLUSION: Most children with CZS show severe motor impairment; a small part of those exposed to ZIKV, without evidence of the syndrome at birth, have alteration in neurodevelopment. Those children should be followed in the long-term, since some manifestations may occur belatedly.
Keywords:
Congenital zika syndrome, Microcephaly, Motor development
RESUMO
OBJETIVOS: analisar o desenvolvimento motor, nos dois primeiros anos de vida, de crianças com evidências da síndrome congênita pelo Zika vírus (SCZ) ao nascimento e de crianças expostas ao Zika vírus (ZIKV) durante a gestação, mas sem evidências da SCZ.
MÉTODOS: revisão sistemática, segundo as recomendações da Preferred Reporting Items for Systematic Reviews (PRISMA). A busca ocorreu nas bases BVS/interface LILACS e BIREME/interface PubMed até março de 2020. Duas pesquisadoras analisaram a qualidade dos estudos pela metodologia do Johanna Briggs Institute.
RESULTADOS: entre 184 publicações, selecionou-se 21 artigos. Crianças com a SCZ apresentam grave comprometimento das funções motoras e alta prevalência de paralisia cerebral espástica. Aos dois anos de vida, a maior parte atingiu apenas níveis iniciais do desenvolvimento motor; com comprometimento da visão, audição, linguagem, cognição, comportamento e interação social. Já as crianças expostas ao ZIKV, mas sem evidências da SCZ, estão em menor risco, cerca de 20% apresentam manifestações tardias de atraso e/ou anormalidade do neurodesenvolvimento. Variáveis associadas a maior comprometimento motor são: infecção materna precoce, nascimento pré-termo, menor perímetro cefálico, exame de imagem anormal, uso de anticonvulsivante, aumento da idade, artrogripose, epilepsia, déficits da visão, linguagem, cognição, e menor renda.
CONCLUSÃO: a maioria das crianças com SCZ apresenta grave comprometimento motor; pequena parte das expostas ao ZIKV, sem evidências da síndrome ao nascimento, tem alteração no neurodesenvolvimento. Estas crianças devem ser acompanhadas por longo prazo, pois algumas manifestações podem ser tardias.
Palavras-chave:
Síndrome congênita de Zika, Microcefalia, Desenvolvimento motor
IntroductionIn Brazil, the spread of Zika virus (ZIKV) through
Aedes aegypti mosquito was first detected in the Northeast region, and it coincided with the sudden increase of births of children with microcephaly.
1,2 The correlation of the increase of the number of microcephaly cases and maternal infection by ZIKV was proven by laboratory exams.
3,4 Initially, microcephaly was defined as the cerebral malformation most frequently related to congenital infection by ZIKV, however, it is already known that it does not occur in every case.
5Congenital infection by ZIKV results in a complex clinical condition denominated congenital zika virus syndrome (CZS). CZS is characterized by diverse clinical manifestations, and among the most prevalent cerebral malformations, are corpus callosum abnormalities, brain volume loss, calcifications, ventriculomegaly, cortical malformation, microcephaly (present in 55.6% to 77.8% of cases, at birth) and osteomuscular deformities.
6 Since microcephaly may be present or not, it is not the determinant element for diagnosis.
5 With regard to clinical manifestations, we highlight the impairment of motor, linguistic and cognitive functions, epilepsy, hearing and visual loss, irritability, hypertonia, dyskinesia and hyperreflexia.
5,7-9Between 2015 and 2020, 3,564 cases of CZS were confirmed, mostly in the Northeast region (61.9%). Of the confirmed cases, 60.6% received specialized care,
10 and since the syndrome’s clinical condition is severe, complex and lead to longstanding repercussions, the proportion of children without specialized care (39.4%) is concerning.
Greater impairments in motor development are frequent in children with evidence of CZS at birth and among those with lower head circumference and severe cortical malformations.
11 Nevertheless, children with congenital infection by ZIKV, but without microcephaly and/or cerebral malformations at birth are also at risk and should have their development monitored.
8Motor development is a continuous process of changes in movement across life, and comes from the complex interaction between the neural and musculoskeletal systems, including cognitive and perceptive processes. It is affected by many variables, including individual aspects such as age, sex, nutrition and diseases, socioeconomic status, culture, environment factors and developed tasks. The psychometric tools of screening and assessment of motor development identified children at risk by means of the analysis of motor behaviors, postural control and functional skills.
12,13 Data quantification is an important resource to track delays, to the referral to early intervention and to help planning interventions.
There is still much to be done in regard to strengthening healthcare actions for the population to receive guidelines on prevention from ZIKV infection, prevention from vertical transmission, besides prenatal care and postpartum care. Preventive measures, early diagnosis of delay or atypical motor development, performed by means of specific screening tools and the referral to rehabilitation services mitigate the impact of the disorder in children’s health.
In view of the above, the aim of this review is to analyze motor development in the two first years of life in children with CZS evidence at birth and children exposed to ZIKV during pregnancy, but without CZS evidence at birth.
MethodsSystematic review registered at the database of prospectively registered systematic reviews (PROSPERO, number CRD42020208262), developed according guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
14 Searches in the databases: BVS/interface LILACS, BIREME/interface PubMed and manual search in the reference lists of selected articles. A date filter was used to select articles published after 2015, when occurred the onset of ZIKV epidemic in Brazil, until March 2020. We used combinations of descriptors controlled in DeCS/BVS: infant development AND Zika virus; developmental disorders AND Zika virus. The combinations of descriptors of MeSH/PubMed were:psychomotor performance AND Zika virus; motor development AND Zika virus; developmental disabilities AND Zika virus. Descriptors were combined by means of AND Boolean operator,
We searched for original studies, published in the aforementioned databases and that allowed to answer the following research question: How is the motor development in the first two years of life, of children with evidence of CZS at birth and children exposed to ZIKV during pregnancy, but without scientific evidence of CZS at birth? Thus, the studied outcome was the motor development of these children in the first two years of life.
After search, duplicate titles were excluded and exclusion and inclusion criteria were applied to the others. Inclusion criteria were: 1) observational studies aiming in the description of motor development of children with CZS and/or children exposed to ZIKV during pregnancy; 2) articles that included in the sample, children with CZS manifestations (for example: laboratory evidence of congenital infection by ZIKV accompanied by microcephaly and/or other characteristic cerebral malformations and clinical manifestations of ZIKV infection); 3) articles that included in the sample, children with laboratory evidence of congenital infection by ZIKV, but without evidence of CZS at birth); 4) studies that used validated and standardized screening or assessment tools for children motor development; 5) publications quoted as reference in selected article, when met inclusion criteria. The exclusion criteria were: 1) description of social, preventive, epidemiological and clinical aspects of ZIKV infection and CZS; 2) focus on health surveillance, protocols of intervention and treatment of children with CZS; 3) literature reviews, editorials and study protocols; 4) studies on parenting, health and wellbeing of caregivers; 5) description of clinical manifestations, malformations, hearing, language, visual and cognitive development and studies that did not use standard tools to assess development; 6) associations between
Guillain-Barré syndrome and ZIKV; 7) studies of low methodological quality (percentage under 50% in the evaluation checklist).
The entire process of search and selection was conducted by two independent researchers. The critical evaluation of quality of studies followed the methodology of Johanna Briggs Institute (JBI).
15 Four tools were used (checklists) according to study design: checklist for case studies (eight items), checklist for case series (ten items), checklist for analytical cross-sectional studies (eight items), checklist for cohort studies (11 items). For each item, there are four options: yes, no, not clear, not applicable. We calculated the percentage of “yes” answers for each study, the “not applicable” answer was not calculated. Studies with a percentage under 50%, with risk of bias classified as high
16 were excluded.
For qualitative synthesis, authors extracted data from articles by means of a form in which they filled the following information: authors, year of publication, country/state of origin if children, study type, characteristics of sample (sample size, age, CZS diagnosis or exposition to ZIKV during pregnancy), assessment tools for motor development and main results related to children motor development.
Results178 titles were located bymeans of database search and five titles by manual search. After removing duplicates, 130 titles subject to screening remained. Of these, 107 were discarded, for meeting exclusion criteria. 23 articles then remained to be submitted for evaluation of methodological quality. Two articles were excluded for presenting scores under 50% in the Johanna Briggs Institute tool. In the end of selection, 21 articles were included for meeting inclusion criteria and having adequate methodological quality, as detailed in the flowchart (Figure 1).
With regard to methodological quality evaluation, the score varied between 50% and 100%, with a mean of 82.8%, revealing good general quality. The most frequently found methodological problem in included articles was the absence of description or little clarity in the presentation of sociodemographical characteristics of participants.
8,9,17-27Studies selected were published between 2016 and March 2020, twenty conducted with Brazilian population and one with Colombian population.
26 Surveys conducted in Brazil included predominantly children living in the Northeast region, six studies with sample of children from Bahia state,
17,19,24,28-30 four from Pernambuco state,
18,21,23,31 three from Paraíba state
11,20,22 and two from Rio Grande do Norte state
20,23; five were conducted in the South region, four in Rio de Janeiro state
8,9,25,27 and one in Minas Gerais
9; two in the Midwest region, one in Mato Grosso
34 and one in Mato Grosso do Sul.
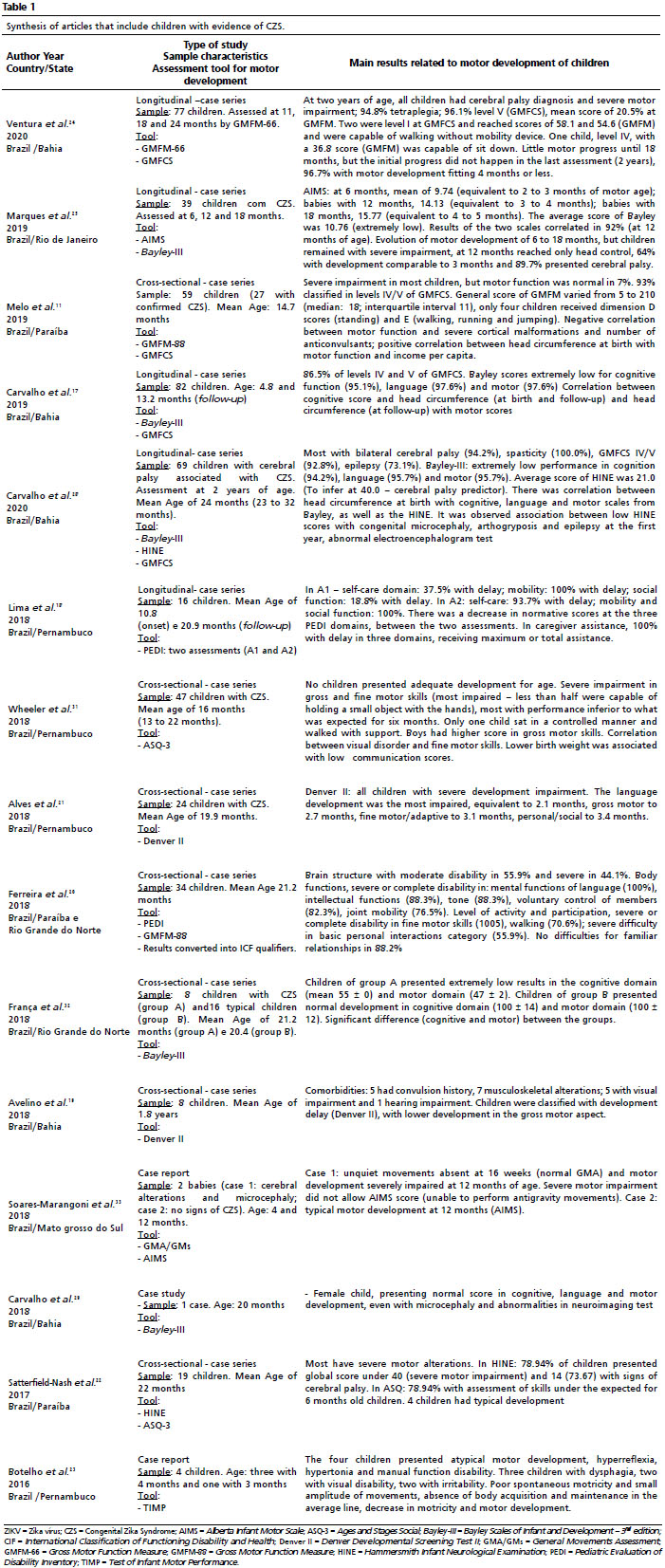
33Fifteen studies assessed children with CZS
11,17-25,28,29,31-33 (Table 1), three articles
26,30,34 assessed children exposed to ZIKV during pregnancy, but without confirmation or evidence of CZS at birth (Table 2) and three articles
8,9,27 assessed both children with CZS and children exposed to ZIKV, but without diagnosis of CZS at birth (Table 3). All studies included children of both genders, aged up to 32 months.
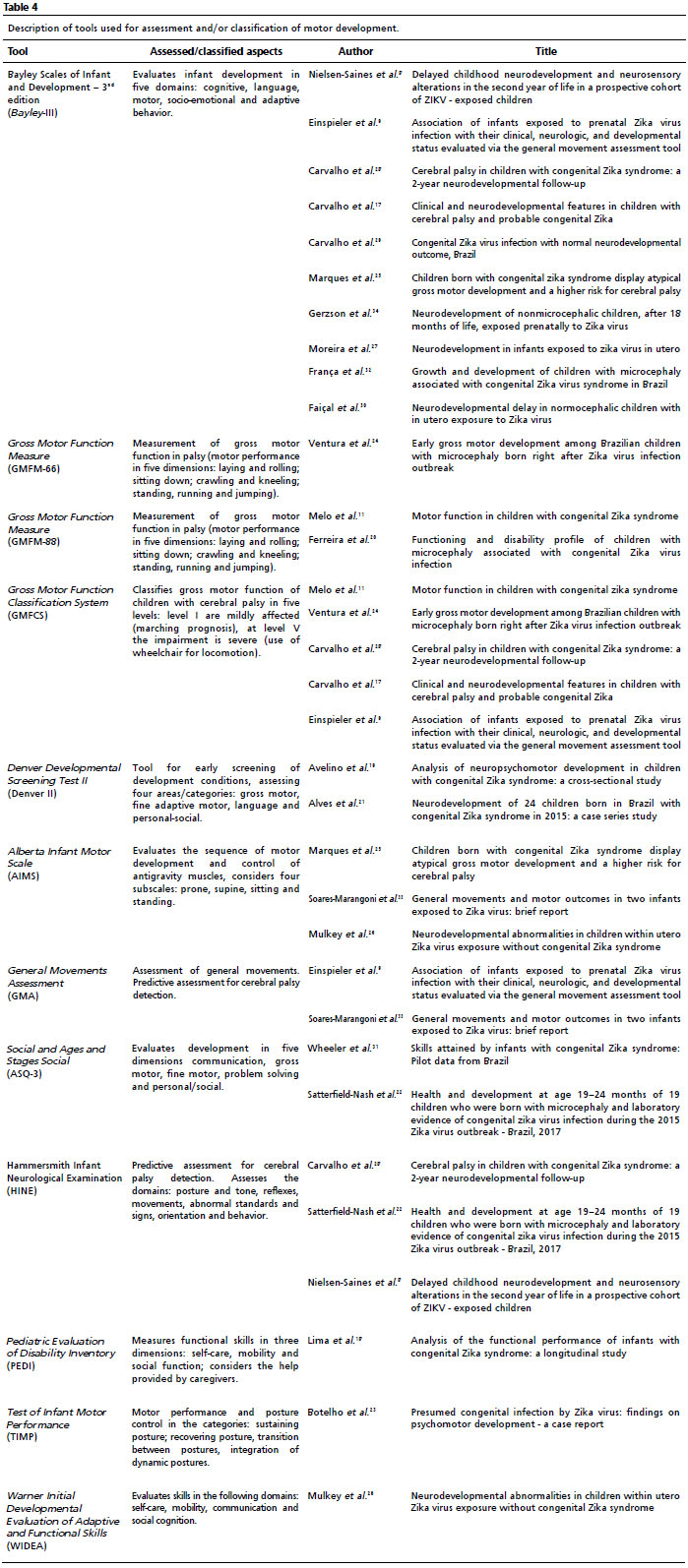
Tools used for assessment and/or classification of motor development were: Bayley-III scale, Gross Motor Function Measure (GMFM) and Gross Motor Function Classification System (GMFCS), Alberta Infant Motor Scale (AIMS), Denver Developmental Screening Test II (Denver II), Hammersmith Infant Neurological Examination (HINE), General Movements Assessment (GMA), Ages and Stages Social (ASQ-3), Warner Initial Developmental Evaluation of Adaptive and Functional Skills (WIDEA), Pediatric Evaluation of Disability Inventory (PEDI); Test of Infant Motor Performance (TIMP). Besides motor and/or functional assessment, the measured construct includes aspects related to development of socio-emotional, cognitive, language, adaptive behavior, personal-social and self-care order, as detailed in Table 4. The GMFM, GMFCS, AIMS, GMA, HINE and TIMP measure and/or classify exclusively aspects of motor development. HINE and GMA have excellent capability of predict risk of cerebral palsy.
35Studies that included children with CZS evidenceIn the 15 studies that assessed children with CZS evidence, authors highlighted that the inclusion criteria in thesample were mainly laboratory exams that verified ZIKV congenital infection, microcephaly and/or cerebral congenital manifestations and clinical manifestations typical of ZIKV infection. Children were aged up to 32 months, the study
29 with the smaller sample described a single case and that with the greatest sample included 82 children.
17 The total of assessed children was 487, but the methodological and authorial similarity indicates that at least 2 studies used part of the same sample group.
17,28 Five studies had prospective longitudinal model.
17,18,24,25,28 Five surveys used Bayley-III scale,
17,25,28,29,32 the authors highlighted the high proportion of children with extremely low mean scores in the cognitive, motor and language domains. Studies that included more than one development assessment tool – AIMS and Bayley-III,
25 Bayley-III and HINE,
28 HINE and ASQ-3,
22 AIMS and GMA/GMs
33 - concluded that results were similar and/or correlated to the associated use of scales confirmed low motor development and evolution of children.
Among the main results, we highlight high frequency of cerebral palsy, severe global motor development, bilateral spasticity (quadriplegia), most children were classified in levels IV or V of GMFCS,
11,17,21,22,24,25,28 even at two years old, reached only initial levels of motor control, which are the control of the had in prone position and being able to sit with support. Circa 73.67% to 100% of the sample presented signs of cerebral palsy and spasticity;
22,24,25,28 86.5% to 92.8% were classified in levels IV and V of GMFCS.
11,17,28 On the other hand, 7% to 21% had typical development,
11,22 two children were classified in level I and were capable of walking without auxiliary device and one child, level IV, was able to sit down.
24 There is also the report of a child of twenty months of life with congenital microcephaly and abnormalities at the neuroimaging test, but with normal scores in the cognitive, motor and language domains, measured by Bayley-III scale.
29An evaluation with 34 children was converted in qualifiers of the International Classification of Functioning, Disability and Health (ICF) and demonstrated high proportion of children with severe or complete disorder in intellectual and language functions, muscle tone, joint mobility, voluntary movement control, fine motor skills and walking.
20 A study with PEDI inventory highlighted severe functional impairment, resulting in need for maximum or total assistance from caregivers, in the domains of self-care, mobility and social function.
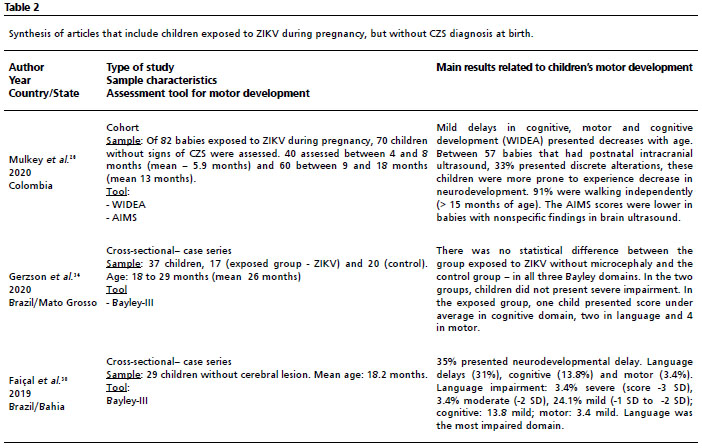
18Studies that included children exposed to ZIKV during pregnancy, but without evidence of CZS at birthThree articles included children exposed to ZIKV during gestation, however, without CZS diagnosis at birth.
26,30,34 128 children were assessed, aged between four to 29 months. One study had longitudinal follow up and used AIMS and WIDEA to evaluate development,
26 two cross-sectional studies used Bayley-III scale.
30,34Most children exposed to ZIKV in pregnancy that were born without microcephaly or alterations in brain imaging tests did not show delay, 91% were walking without support at 15 months of age. However, 33% of children in the follow up presented ultrasound with discrete alterations and were more subject to delays in the first 18 months of live.
26 A study
34 that compared 17 children exposed to ZIKV and without microcephaly with 20 non-exposed children, did not show difference between the groups. In the exposed group, one child showed a score under mean average in the cognitive domain, two in language and four in motor function.
34 Among 29 exposed children without cephalic lesion, 31% of language delay was identified, as well as 14% in cognition and 3% in motor function.
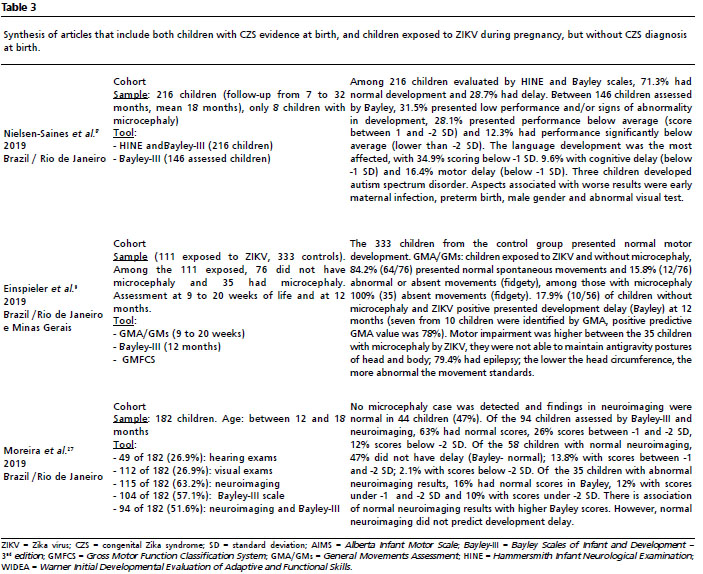
30Studies that included both children with CZS evidence at birth and exposed children without CZS evidenceThree studies followed the development of both children exposed to ZIKV in pregnancy and with evidence of CZS (microcephaly and/or specific alteration in imaging tests), and those exposed, but without CZS evidence.
8,9,27 The methodological and authorial similarity indicates that these studies used part of the same sample group. Bayley-III scale was used in the three cohorts, one survey included HINE scale
8 and another, the GMA/Gms and GMFCS.
9A follow-up study included 216 children exposed to ZIKV, 8 with microcephaly, at two years 71.3% had normal development and 28.7%, delay. Language development was the most affected, followed by motor and cognitive.
8 A follow-up study until 12 months of age, of 444 children (111 exposed, 56 without microcephaly and ZIKV positive, 35 with microcephaly, 333 controls) indicated that 84.2% of children without microcephaly presented normal spontaneous movements and 15.8%, abnormal or absent movements. Every child with microcephaly presented abnormal or absent movements, bilateral spasticity and difficulty in maintaining postures against gravity. Ten children without microcephaly presented development delay (Bayley-III) at 12 months, of these, seven were identified by GMA/GMs at three months, reassuring the importance of this tool for early screening and detection of neurological disorders that lead to motor impairment.
9Besides motor delay, children exposed to ZIKV are subject to delay in language and cognitive functions, visual and hearing impairments.
27 Among postural alterations present in children exposed to ZIKV, and more frequent in those with microcephaly, we highlight: head out of average line, postural asymmetry, neck and or/thorax hyperextension, limbs in extension, fingers in extension and abduction, lack of variety of movements and postures.
9DiscussionThe systematic review demonstrated that children with congenital ZIKV infection, mainly those with CZS evidence at birth, presented severe motor impairment and minor evolution across the years. Even at two years of life, most of them achieved only the initial levels of gross motor development. The major difficulty is to assume high postures that demand control against gravity, since motor coordination and head and body control are little developed or absent. The most impaired motor functions include activities in the sitting, standing and walking postures
9,21,24,25,31 and the motor repertory is poor.
8,18,21,23,28 There is high prevalence of cerebral palsy with bilateral spasticity, epilepsy, persistence of primitive reflexes, poor balance reactions, extension spasms and neuromusculoskeletal deformities and abnormal posturing.
8,11,22,24,25,28Among frequent neuromusculoskeletal disorders in children with CZA are: spasticity, hyperreflexia, spasms, clonus,
17,21,24,28,31 persistence of primitive reflexes, dyskinesia, absent or abnormal posture reactions,
9,18,21,23,25,28 musculoskeletal deformities,
9,17,19,28,31 hip dislocation,
18 epilepsy/convulsions
9,11,17-19,21,22,24,25,28,31 and growth impairment.
32 The broad involvement of several body structures reverberates in posture and atypical and poorly-varied movements, asymmetry and severe motor impairment. Motor alterations and epilepsy are among the most common disorders in children with CZS and need to be early identified so that they can meet the criteria of clinical assessment, followed by early referral to intervention strategies.
7The disorders are extensive and complexand involve several functions, such as cognitive, speech and language,
8,21,22,26,28,31, hearing,
8,17-19,21,22,25,28,32 visual
8,18,19,21-23,31,33 social
18,21,22,26,31 cognition/learning,
8,17,20,26,28,31,32 emotional,
22 behavioral (irritability)
23, deglutition/feeding
18,24, breathing
18,22,23 and sleep.
22,31 We highlight that both gross and fine motor development are strongly related to cognitive and language disorders.
36Motor disabilities bring severe consequences such as: dysphagia, structured musculoskeletal deformities, poor sensorial, emotional and environmental exploration, with consequent impairment in the other areas of neurodevelopment. Limitations on basic functions such as eating and self-hygiene imply permanent need for care and assistance.
31With regard to follow-up across time, the motor development of children with CZS presented decline with the increase of age,
18,26 or even with small progress, the impairment remained severe.
24,25 Analyses demonstrated association of motor development with cortical malformations or administration of anticonvulsant drugs,
9,11,27 congenital microcephaly,arthrogryposis, epilespy and abnormal imaging test.
26,28 Lower head circumference is associated with greater impairment of motor,
9,11,17,28 cognitive
9,17,27,28 and low income
per capita.
11 Greater impairment in development is associated with early maternal infection, preterm birth and abnormal eye exam.
8 Association between visual disorder and higher impairment of fine motor skills; low birthweight is associated with lower communication scores
31 In regard of the relationship of the children’s gender and severity of neuropsychomotor impairment, two studies
8,31 bring diverging results. Nielsen-Saines
et al.
8 highlight that the development was more affected in male children, while Wheeler
et al.
31 described how boys presented better gross motor skills. These findings reinforce the importance of further analyses that investigate risks related to gender.
Children that were born without microcephaly and normal neuroimaging (or subtle alterations) may evolve with delays in development and should be followed in the long-term, since impairment manifestations may occur late. Although a high proportion of babies exposed to ZIKV without microcephaly develop normally, 15.8%
9 to 33%
26 will have atypical development.
A positive aspect highlighted by one study,
8 is the fact that children with lower neurological impairment, which suffered negative effects of virus exposition at the first months of life may have normal performance in late assessments. Two children who had microcephaly at birth reached normal head circumference and development at the second year of life. On the other hand, three children, without microcephaly, developed autism spectrum disorder.
8 One child, with normal head circumference at birth, developed secondary microcephaly and presented abnormal standards in movements.
9Studies pointed the association between births of neonates with microcephaly by ZIKV and bad life conditions, evidencing that socioeconomic factors also played a role in ZIKV epidemic in Brazil and may have contributed to a higher distribution of cases in economically vulnerable areas in the Northeast of the country.
37,38 Low income families with many family members have greater chance of having a child with ZIKV congenital infection, on the other hand, higher maternal schooling seem to be a protective factor. There is also consistent relation between the delay in language, motor and cognitive development and unfavorable socioeconomic indicators.
39The severe motor impairment in children with CZS is certainly a public health problem and higher care should be provided to families in situation of socioeconomic vulnerability. Considering that neurodevelopmental disorders are permanent and tend to get worse across time, demanding permanent care, high financial costs and overloading families even more.
Even in face of this challenging scenario, we highlight positive aspects. Challenges are encouraging scientific research in Brazil, valorizing competence and effort from Brazilian researchers, and strengthening relationships and international scientific partnerships, allowing the achievement of social rights and expanding knowledge related to assessment and healthcare for people with disabilities. It should be also considered the possibility of a higher visibility and opportunity to expand prevention and rehabilitation strategies to people who have other neurodevelopmental disorders.
As limitations related to results of this review, we mention the heterogeneity of definition of criteria for sample composition, mainly concerning evidence of ZIKV congenital infection and definition of CZS evidence. There is little information on results of clinical, laboratory and/or image tests; and risk of problems in medical records registries. The main parameter for CZS definition in children with congenital ZIKV infection was the presence of microcephaly and/or other cerebral malformations (among them, intracranial calcifications, ventriculomegaly, and cerebral atrophy). However, it is known that microcephaly might not be the best parameter to detect children affected by CZS, since it may not be present at birth, nor follow other findings that evidence CZS, or have further onset.
6 Accordingly, there is lack of standardization in terminology and protocols for CZS diagnosis. It should be also considered that parameters to identify babies with suspected microcephaly and protocols to assess CZS have been modified by the World Health Organization.
5It should be also considered that even screening, assessment and classification tools for development have been translated, adapted and validated for use in the study population, and they were developed and standardized mainly in the United States and Canada, countries in which the normative sample was established. A systematic review demonstrated limitedvalidity of these tests in different cultures than those in which the normative sample was established.
13 Moreover, there still exists little or no description at all about the expertise of researchers for the application of tools and about the standardization of assessment and interpretation of results.
Considering the impact of the ZIKV epidemic and its repercussions in the development of children affected by CZS and lives of families, it draws attention to the fact that we were not capable of finding more studies aiming at the assessment of motor development of the affected population. We question whether it occurred because of the fact of being an epidemiological event that affected a specific demographic area (South America, Brazil).
As final considerations, children with CZS present severe impairment in motor functions, even at two years of life, and most children only were able to reach the initial stages of gross motor development. There was high prevalenceof bilateral spastic cerebral palsy, with higher proportion of children classified at levels IV and V of GMFCS, impairment of other functional areas such as sight, hearing, language, cognition, behavior and social interaction. On the other hand, children exposed to ZIKV, but without CZS evidence at birth, are at lower risk, 15.5% to 33% develop with delay and/or abnormality of neurodevelopment, impairing mainly language functions. Finally, the results of this review evidenced that children exposed to ZIKV, with or without CZS, should have their global development monitored in the long-term, since some manifestations may have late onset.
Children should have their psychomotor development assessed across the years, preferably with standardized tests, and those with suspected delay or neurodevelopmental abnormality should be referred to early intervention with a specialized team. The approach should be early and multiprofessional, comprising biopsychosocial aspects, with strategies of prevention for new cases and mitigation of harms. We highlight the importance of implementing criteria for terminology and early diagnosis for both congenital infection and CZS, besides further longitudinal studies and implementation of intervention strategies aiming for better functionality and social participation of the affected population. It is also necessary to include families in the social and healthcare programs, since the demands required by children affected by CZS are broad and longstanding.
References1. Oliveira WK, França GVA, Carmo EH, Duncan BB, Souza Kuchenbecker R, Schmidt MI. Infection-related microcephaly after the 2015 and 2016 Zika virus outbreaks in Brazil: a surveillance-based analysis. Lancet. 2017; 390 (10097): 861-70.
2. Marinho F, Araujo VE, Porto DL, Ferreira HL, Coelho MR, Lecca RC,
et al. Microcephaly in Brazil: prevalence and characterization of cases from the Information System on Live Births (Sinasc), 2000-2015. Epidemiol Serv Saúde. 2016; 25 (4): 701-12.
3. Araújo TVB, Rodrigues LC, Alencar Ximenes RA, Barros Miranda-Filho D, Montarroyos UR, Melo APL,
et al. Association between Zika virus infection and microcephaly in Brazil, January to May, 2016: preliminary report of a case-control study. Lancet Infect Diseases. 2016; 16 (12): 1356-63.
4. Brady OJ, Osgood-Zimmerman A, Kassebaum NJ, Ray SE, Araujo VEM, Nobrega AA,
et al. The association between Zika virus infection and microcephaly in Brazil 2015-2017: An observational analysis of over 4 million births. PLoS Med. 2019; 16 (3): e1002755.
5. Teixeira GA, Dantas DNA, Carvalho GAFL, Silva AN, Lira ALBC, Enders BC. Análise do conceito síndrome congênita pelo Zika vírus. Ciênc Saúde Colet. 2020; 25 (2): 567-74.
6. Sanz Cortes M, Rivera AM, Yepez M, Guimaraes CV, Diaz Yunes I, Zarutskie A,
et al. Clinical assessment and brain findings in a cohort of mothers, fetuses and infants infected with ZIKA virus. Am J Obstetr Gynecol. 2018; 218 (4): 440 e1- e36.
7. Pessoa A, Linden VV, Yeargin-Allsopp M, Carvalho MD, Ribeiro E, Braun KV,
et al. Motor abnormalities and epilepsy in infants and children with evidence of congenital Zika virus infection.
Pediatrics. 2018; 141 (2): 167-79.
8. Nielsen-Saines K, Brasil P, Kerin T, Vasconcelos Z, Gabaglia CR, Damasceno L,
et al. Delayed childhood neurodevelopment and neurosensory alterations in the second year of life in a prospective cohort of ZIKV-exposed children. Nat Med. 2019; 25 (8): 1213-7.
9. Einspieler C, Utsch F, Brasil P, Panvequio Aizawa CY, Peyton C, Hydee Hasue R,
et al. Association of Infants Exposed to Prenatal Zika Virus Infection With Their Clinical, Neurologic, and Developmental Status Evaluated via the General Movement Assessment Tool. JAMA Netw Open. 2019; 2 (1): e187235.
10. Ministério da Saúde (BR). Situação epidemiológica da síndrome congênita associada à infecção pelo vírus Zika em 2020 até a SE 45. Brasília (DF): Ministério da Saúde 2020 Nov; 51 (47): 1-18. [access in 2020 dez 1]. Availble from:
https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/edicoes/2020/boletim_epidemiologico_svs_47.pdf11. Melo A, Gama GL, Silva Júnior RA, Assunção PL, Tavares JS, Silva MB,
et al. Motor function in children with congenital Zika syndrome. Dev Med Child Neurol. 2020; 62 (2): 221-6.
12. Haywood KM, Getchell N. Desenvolvimento motor ao longo da vida. 6
a ed. Porto Alegre: Artmed; 2016.
13. Mendonça B, Sargent B, Fetters L. Cross-cultural validity of standardized motor development screening and assessment tools: a systematic review. Dev Med Child Neurol. 2016; 58 (12): 1213-22.
14. Galvão TF, Pansani, TSA, Harrad, D. Principais itens para relatar Revisões sistemáticas e Meta-análises: A recomendação PRISMA. Epidemiol Serv Saúde. 2015; 24 (2): 335-42.
15. Apóstolo JLA. Síntese da evidência no contexto da translação da ciência. Coimbra, Portugal: Escola Superior de Enfermagem de Coimbra; 2017.
16. Almeida GM, Oliveira KHD, Monteiro JS, Medeiros MAT, Recine EGIG. Educational training of nutritionists in Public Health Nutrition: A systematic review. Rev Nutr. 2018; 31 (1): 97-117.
17. Carvalho A, Brites C, Mochida G, Ventura P, Fernandes A, Lage ML,
et al. Clinical and neurodevelopmental features in children with cerebral palsy and probable congenital zika. Brain Dev. 2019; 41 (7): 587-94.
18. Lima DLP, Correia MLGCD, Monteiro MG, Ferraz KM, Wiesiolek CC. Análise do desempenho funcional de lactentes com síndrome congênita do zika: estudo longitudinal. Fisioter Pesq. 2019; 26 (2): 145-50.
19. Avelino MOA, Ferraz PCS. Análise do desenvolvimento neuropsicomotor em crianças com síndrome pószika vírus: um estudo transversal. Rev Pesq Fisioter. 2018; 8 (2): 147-54.
20. Ferreira HNC, Schiariti V, Regalado ICR, Sousa KG, Pereira SA, Fechine C,
et al. Functioning and Disability Profile of Children with Microcephaly Associated with Congenital Zika Virus Infection. Int J Environ Res Public Health. 2018 May; 15 (6): 1107.
21. Alves LA, Paredes EC, Silva GC, Mello JG, GJ Alves. Neurodevelopment of 24 children born in Brazil with congenital Zika syndrome in 2015: A case series study. BMJ Open. 2018; 8 (7): e021304.
22. Satterfield-Nash A, Kotzky K, Allen J, Bertolli J, Moore CA, Pereira IO,
et al. Health and Development at Age 19-24 Months of 19 Children Who Were Born with Microcephaly and Laboratory Evidence of Congenital Zika Virus Infection During the 2015 Zika Virus Outbreak - Brazil, 2017. MMWR Morb Mortal Wkly Rep. 2017; 66 (49): 1347-51.
23. Botelho ACG, Neri LV, Silva MQF, Lima TT, Santos KG, Cunha RMA,
et al. Presumed congenital infection by Zika virus: findings on psychomotor development - a case report. Rev bras saúde matern infant. 2016;16 (Supl. 1): 39-44.
24. Ventura PA, Lage M-LC, Carvalho AL, Fernandes AS, Taguchi TB, Nascimento-Carvalho CM. Early Gross Motor Development Among Brazilian Children with Microcephaly Born Right After Zika Virus Infection Outbreak. J Dev Behav Pediatr. 2020; 41 (2): 134-40.
25. Marques FJP, Teixeira MCS, Barra RR, Lima FM, Dias BLS, Pupe C,
et al. Children Born With Congenital Zika Syndrome Display Atypical Gross Motor Development and a Higher Risk for Cerebral Palsy. J Child Neurol. 2019; 34 (2): 81-5.
26. Mulkey SB, Arroyave-Wessel M, Peyton C, Bulas DI, Fourzali Y, Jiang J,
et al. Neurodevelopmental Abnormalities in Children With In Utero Zika Virus Exposure Without Congenital Zika Syndrome. JAMA Pediatr. 2020; 174 (3): 269-76.
27. Lopes Moreira ME, Nielsen-Saines K, Brasil P, Kerin T, Damasceno L, Pone M,
et al. Neurodevelopment in Infants Exposed to Zika Virus In Utero. N Engl J Med. 2018; 379 (24): 2377-9.
28. Carvalho AL, Ventura P, Taguchi T, Brandi I, Brites C, Lucena R. Cerebral Palsy in Children With Congenital Zika Syndrome: A 2-Year Neurodevelopmental Follow-up. J Child Neurol. 2020; 35 (3): 202-7.
29. Carvalho AL, Brites C, Taguchi TB, Pinho SF, Campos G, Lucena R. Congenital Zika virus infection with normal neurodevelopmental outcome, Brazil. Emerg Infect Dis. 2018; 24 (11): 2128-30.
30. Faiçal AV, Oliveira JC, Oliveira JVV, Almeida BL, Agra IA, Alcantara LCJ,
et al. Neurodevelopmental delay in normocephalic children with in utero exposure to Zika virus. BMJ paediatrics open. 2019; 3 (1): e000486.
31. Wheeler AC, Ventura CV, Ridenour T, Toth D, Nobrega LL, Dantas LCSS,
et al. Skills attained by infants with congenital Zika syndrome: Pilot data from Brazil. PLoS One. 2018 Jul; 13 (7): e0201495.
32. França TLB, Medeiros WR, Souza NL, Longo E, Pereira SA, França TBO,
et al. Growth and Development of Children with Microcephaly Associated with Congenital Zika Virus Syndrome in Brazil. Int J Environ Res Public Health. 2018 Sep; 15 (9): 1990.
33. Soares-Marangoni DA, Tedesco NM, Nascimento AL, Almeida PR, Santos Pereira CND. General movements and motor outcomes in two infants exposed to Zika virus: brief report. Dev Neurorehabil. 2019 Jan; 22 (1): 71-4.
34. Gerzson LR, Almeida CS, Silva JHD, Feitosa MMA, Oliveira LN, Schuler-Faccini L. Neurodevelopment of Nonmicrocephalic Children, After 18 Months of Life, Exposed Prenatally to Zika Virus. J Child Neurol. 2020; 35 (4): 278-82.
35. Novak I, Morgan C, Adde L, Blackman J, Boyd RN, Brunstrom-Hernandez J,
et al. Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy: Advances in Diagnosis and Treatment. JAMA Pediatr. 2017; 171 (9): 897-907.
36. Houwen S, Visser L, Van der Putten A, Vlaskamp C. The interrelationships between motor, cognitive, and language development in children with and without intellectual and developmental disabilities. Res Dev Disabil. 2016; 53-54: 19-31.
37. Souza WV, Albuquerque M, Vazquez E, Bezerra LCA, Mendes A, Lyra TM,
et al. Microcephaly epidemic related to the Zika virus and living conditions in Recife, Northeast Brazil. BMC Public Health. 2018 Jan; 18 (1): 130.
38. Campos MC, Dombrowski JG, Phelan J, Marinho CRF, Hibberd M, Clark TG,
et al. Zika might not be acting alone: Using an ecological study approach to investigate potential co-acting risk factors for an unusual pattern of microcephaly in Brazil. PLoS One. 2018 Aug; 13 (8): e0201452.
39. Power GM, Francis SC, Sanchez Clemente N, Vasconcelos Z, Brasil P, Nielsen-Saines K,
et al. Examining the Association of Socioeconomic Position with Microcephaly and Delayed Childhood Neurodevelopment among Children with Prenatal Zika Virus Exposure. Viruses. 2020 Nov; 12 (11): 1342.
Received on May 3, 2021
Final version presented on May 10, 2022
Approved on September 2, 2022
Author’s contribution: Ribeiro MFM and Queiróz KBP participated in the conceptualization and study design, performed the search, selection and synthesis of articles. Ribeiro MFM and Prudente COM contributed to the data synthesis and final reviews of the manuscript.
The authors approved the final version of the manuscript and declare no conflict of interest.


 ; Karla Beatriz Presto de Queiróz2
; Karla Beatriz Presto de Queiróz2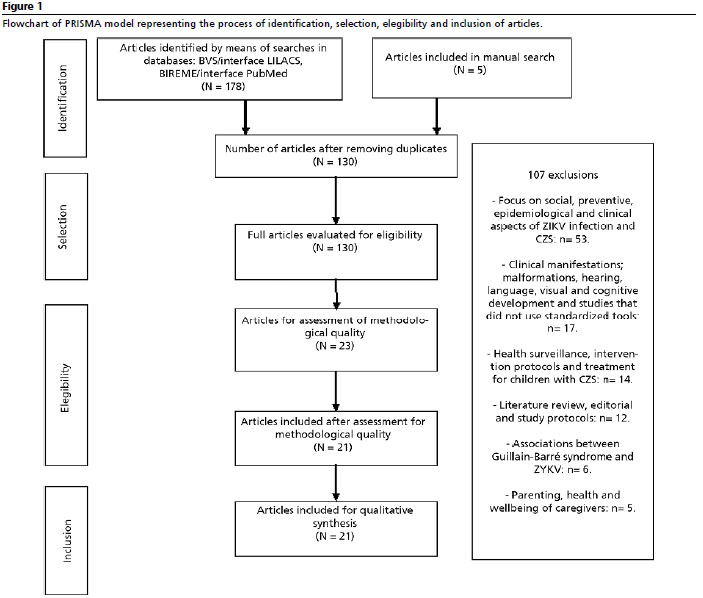






 Ler em português
Ler em português