ABSTRACT
OBJECTIVES: to estimate the prevalence of overweight/obesity and analyze the associated factors in pregnant women assisted by family health teams.
METHODS: epidemiological observational study of populational, cross-sectional, and analytical base carried out with pregnant women at the Estratégia de Saúde da Família (Family Health Strategy) in the city of Montes Claros, Minas Gerais State, Brazil, between October 2018 and November 2019. Socioeconomic and demographic, obstetric characteristics, social and family support, emotional aspects and comorbidities. The presence of overweight/obesity was estimated by the initial Body Mass Index (up to the 13th gestational week) acquired from the pregnant woman's health booklet. Hierarchized Poisson regression with robust variance was carried out.
RESULTS: a total of 1,279 pregnant women participated in this study. The prevalence of overweight/obesity was 45.3% and was associated with the following factors: having a partner (PR=1.52; CI95% =1.24-1.86), higher family income (PR=1.23; CI95% =1.04-1.46), presence of previous pregnancies (PR=1.65; CI95% =1.39-1.95%), higher age group (PR=2.26; CI95% =1.70-3.01), gestational diabetes mellitus (PR=1.43; CI95% =1.21-1.69) and systemic arterial hypertension (PR=1.29; CI95% =1.04-1.61).
CONCLUSION: there was a high prevalence of overweight/obesity in the evaluated pregnant women and its association with sociodemographic and obstetric factors and chronic comorbidities. There is a necessity for monitoring and carrying out nutritional education in prenatal care provided by family health teams, with emphasis on strengthening multidisciplinary care.
Keywords:
Pregnant women, Nutritional status, Overweight, Obesity, Primary health care
RESUMO
OBJETIVOS: estimar a prevalência de sobrepeso/obesidade e analisar os fatores associados em gestantes assistidas por equipes de saúde da família.
MÉTODOS: estudo epidemiológico observacional de base populacional, transversal e analítico, realizado com gestantes da Estratégia de Saúde da Família em Montes Claros, MG, Brasil, entre outubro de 2018 a novembro de 2019. Avaliaram-se características socioeconômicas e demográficas, obstétricas, apoio social e familiar, aspectos emocionais e comorbidades. A presença de sobrepeso/obesidade foi estimada pelo Índice de Massa Corporal inicial (até 13ª semana gestacional) adquirido da caderneta da gestante. Foi realizada regressão de Poisson hierarquizada com variância robusta.
RESULTADOS: participaram deste estudo 1.279 gestantes. A prevalência do sobrepeso/obesidade foi de 45,3% e esteve associada aos fatores: ter companheiro(a) (RP=1,52; IC95%=1,24-1,86), maior renda familiar (RP=1,23; IC95%=1,04-1,46), presença de gestações anteriores (RP=1,65; IC95%=1,39-1,95%), maior faixa etária (RP=2,26; IC 95%=1,70-3,01), diabetes mellitus gestacional (RP=1,43; IC95%=1,21-1,69) e hipertensão arterial sistêmica (RP=1,29; IC95%=1,04-1,61).
CONCLUSÃO: verificou-se alta prevalência de sobrepeso/obesidade nas gestantes avaliadas e sua associação com fatores sociodemográficos, obstétricos e comorbidades crônicas. Há necessidade de monitoramento e de realização da educação nutricional no cuidado pré-natal prestado pelas equipes de saúde da família, com ênfase no fortalecimento do cuidado multiprofissional.
Palavras-chave:
Gestantes, Estado nutricional, Sobrepeso, Obesidade, Atenção primária à saúde
IntroductionThe increasing prevalence of overweight and obesity over the last decades has resulted in a higher frequency of obese people in all age groups, including in early and/or during pregnancy. Pregnancy is characterized by metabolic and physiological changes that imply an increase in the women's nutritional and energy needs. Pre-gestational maternal obesity and excessive gestational weight gain have been considered serious public health problems in Brazil and worldwide. In the scope of Primary Health Care (PHC), during prenatal care, information regarding weight and height allows the team to evaluate the evolution of weight gain and to carry out specific interventions for each case. It is necessary to guide and encourage pregnant women to adopt eating and self-care behaviors in relation to adequate nutritional status.
1,2Overweight/obesity is becoming increasingly prevalent and has generated impacts in the public health systems.
2,3 High prevalences of overweight/obesity in pregnancy have been observed in the international scenario, between 42.3% and 50.7%,
4-6 and at national level in the range of 38.3% to 70.0%.
1,2,7 These values can be influenced by lifestyle factors such as sedentary lifestyle, low quality diet,
2,8 sociocultural aspects,
9 lack of social support
10 and presence of depressive symptoms.
11This condition in the gestational period increases the chances of complications for the woman, such as gestational diabetes mellitus, hypertensive syndromes in pregnancy,
12 pre-eclampsia, eclampsia, increased weight retention after cesarean section and increased risk of future obesity.
13 There are also risks for the conceptus, such as fetal macrosomia, large for gestational age (LGA) newborn,
12,13 cardiac ruptures, neural tube defects and fetal death.
3,12The gestational period should be monitored in prenatal care in a systematic and multiprofessional manner,
13 in the PHC setting.
13,14 PHC professionals should perform early diagnosis on overweight and establish care to control weight gain in assisting pregnant women, aiming to prevent overweight and obesity, as well as unfavorable maternal and neonatal outcomes.
8,14,15It is necessary to understand the determinants of overweight/obesity in pregnant women to establish early interventions aiming to ensure maternal and child health,
15 especially from the prenatal care offered by the Family Health Strategy (FHS) teams.Considering the possibilities of maternal-fetal complications and the regional/cultural differences that involve women in the pregnancy period, this study aimed to estimate the prevalence of overweight/obesity and analyze the associated factors in pregnant women assisted by the Family Health teams.
MethodsThis is a population-based observational epidemiological survey with a cross-sectional and analytical design. Cross-sectional data from the baseline of a large study entitled "
Estudo ALGE - Avaliação das condições de saúde das gestantes de Montes Claros - MG: estudo longitudinal" (ALGE Study - Evaluation of the health conditions of pregnant women in Montes Claros - MG: longitudinal study) was used. This study only dealt with a cross-sectional analysis of the baseline of the ALGE Study, in which several pregnant women had health and disease conditions assisted by the FHS teams in the city of Montes Claros addressed: sociodemographic and economic profile, religiosity, gynecological-obstetric characteristics, self-reported complaints and pathologies, alcohol and illicit drug use, lifestyle habits, immunization and supplementation, emotional and mental health aspects, social and family support, sexuality, body image and violence.
The city of Montes Claros, the setting for the study is considered a reference center in the service, commerce, education and health sectors in the north of Minas Gerais (MG) - Brazil and has an estimated population of 417,478 inhabitants. The local FHS services were implemented in the 1990s and are currently organized into 15 centers. These centers had a total of 135 family health teams at the time of the investigation (2018-2019), covering 100% of the population.
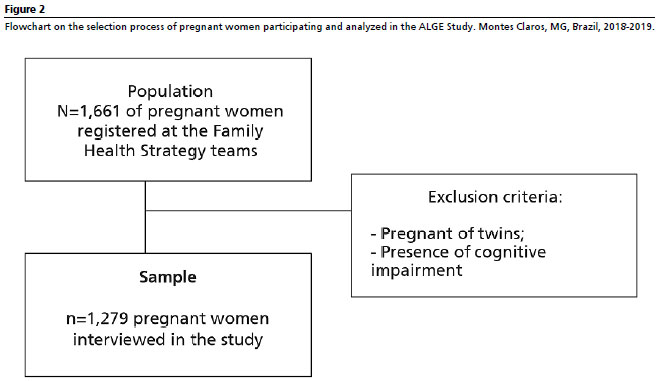
The study population was consisted of 1,661 pregnant women registered with the FHS teams in the urban area of Montes Claros in 2018. Only pregnant women linked to family health teams were included in the investigation. Those who were at any gestational age, registered in these teams, were invited to participate. Women who were pregnant with twins and those with cognitive impairment, as informed by the family member and/or the FHS team, were not included in the survey.
Pregnant women were classified by the nurse and/or physician from the FHS unit and when they were at a high or very high risk, they were referred to referral services of the local public network, where they were assisyed by a gynecologist-obstetrician. In this case, the FHS team continues to monitor pregnant woman.
The sample size was established to estimate population parameters with a prevalence of 50% (to maximize the sample size and due to the original project contemplating several events), 95% confidence interval (CI95%) and precision level of 2.0%. Correction was made for a finite population (N=1,661 pregnant women) and an additional 20% was also established to compensate possible non-response and losses. The calculations showed the need of at least 1,180 pregnant women to participate. For the selection of the sample, all 15 FHS unit centers in the city were considered during the period of this research. The number of pregnant women selected in each center was proportional to their representativeness in relation to the total population of pregnant women registered. A total of 1,279 pregnant women (sample analyzed in this study) were interviewed in the cross-sectional stage of the ALGE Study.
Data collection was carried out from October 2018 to November 2019. Initially, contact was made by the managers of the PHC coordination in the city to raise awareness and authorize the research. After the consent, contact was made by the FHS teams and their health professionals were responsible for the pregnant women's prenatal care and to clarify about the research. Afterwards, the initial contact was made between the interviewer teams and the pregnant women to raise awareness about the research in which the invitation to participate was made and the scheduling of the interview as well. The interview was conducted at a place and time determined by the participants, individually face-to-face, with an average of one hour duration.
A previously trained multiprofessional health team and undergraduate students participated of the interview. A pilot study was previously conducted to verify the instrument and the data collection strategy with the pregnant women registered at FHS health unit (who were not included in the study analyses), in order to standardize the research procedures.
The instrument used for data collection was a structured questionnaire applied during the interview, with questions elaborated by the authors of this study and containing validated instruments, as well as the verification of data from the pregnant woman's health booklet. The following variables were analyzed:
1)
Socioeconomic and demographic characteristics: age group (up to 20 years old, 21 to 30 and over 30), self-declared skin color (white/mixed, black, yellow), schooling (higher education/post-graduate, elementary/high school), marital status (with partner/without partner), occupation (housewife/informal work/none, paid work/self-employed), family income (above one minimum wage, up to one minimum wage) and beneficiary of the
ProgramaBolsa Família (Family Welfare program) (no/yes).
2)
Obstetric characteristics: previous pregnancies (none, one and two or more pregnancies), gestational age at the beginning of prenatal care (≤14 weeks, >14 weeks) information obtained through the pregnant woman's health booklet registrations.
3)
Social and family support: Social support (high/low) and family APGAR (functional/dysfunctional family) were assessed. To verify the presence and absence of social support, the validated Medical Outcome Study (MOS) scale was used.
16 The instrument consists of 19 items, which comprise five functional dimensions: social support, affective, emotional, positive social interaction and information. Each item has response options from 1 to 5 on a likert type scale. The closer the final score is to 100, the better the social support perceived.
16As for family APGAR, the validated Family APGAR instrument was used, which measures the degree of satisfaction through the fulfillment of basic parameters of family function defined by the acronym APGAR: A - Adaptation; P - Participation; G - Growth; A - Affection; R - Resolution. The items have three possible answers ranging from zero to two points. The sum is from zero to ten points. The final classification was functional family (7-10) or dysfunctional family (<6).
174)
Emotional aspects: symptoms of depression (no symptoms/with symptoms) and anxiety (low level/high level). For depressive symptoms assessment, the Center for Epidemiologic Studies Depression Scale (CES-D)
18 validated in Brazil was used, composed of 20 items to assess the presence of depressed mood with frequency of the symptoms occurrence in the last week, using a score ranging from 0, "rarely" (less than one day) to 3, "for most of the day (5-7 days)". The score of the 4 positive items is inverted and adding to the score of others, totaling a final score ranging from 0 to 60. A score ≥22 for "severe depressive symptoms" was used as a cut-off point.
18Anxiety symptoms were measured using the validated instrument called Brazilian State-Trait Anxiety Inventory (STAI),
19 short version, with 12 statements in a likert type scale and options to respond from 1 to 4. The final score was obtained through the sum of the items, which can vary from 12 to 48 points. The cut-off point was the average of the total points, dichotomized into (≤28.4 and >28.4). Pregnant women with scores ≤28.4 were considered to have a "low level of anxiety", and those with scores >28.4 were considered to have a "high level of anxiety".
195)
Comorbidities: gestational diabetes mellitus (absent/present) and systemic arterial hypertension (absent/present), information obtained through the pregnant woman's prenatal booklet registrations.
The nutritional status of the pregnant women was assessed according to Body Mass Index (BMI = weight/height
2), by gestational week. For this purpose, the cut-off points established by Atalah
et al.
20 and recommended by the Ministry of Health
21 for the classification of maternal nutritional status into underweight, eutrophy, overweight and obesity were considered. Weight and height data were collected from the information obtained through the pregnant woman's health booklet registrations at the prenatal consultation up to the 13th gestational week.
In order to verify the factors associated with overweight/obesity in pregnant women, a hierarchical conceptual theoretical model (Figure 1) was developed, as described in a previous study,
22 with adaptations, and in a research with associations of overweight/obesity in pregnant women.
2,3 The variables that composed the socioeconomic and demographic, obstetric, social and family support/support characteristics, in addition to emotional aspects and comorbidities, were considered as independent variables divided into blocks in a theoretical model hypothesized for this study. In this model, it was hypothesized that the more unfavorable the socioeconomic and demographic conditions were,
9 the lower the prenatal care status (obstetric characteristics). In addition, the lower the social and family support
10 and the worse the emotional aspects and comorbidities were, the greater the chances of these pregnant women being overweight/obese.
3 In the theoretical model, the distal hierarchical level was composed of socioeconomic and demographic variables (skin color, schooling, marital status, occupation, income and
Programa Bolsa Família (Family Welfare program), the intermediate level by obstetric characteristics (previous pregnancies gestational age at the beginning of prenatal care) and the proximal level by age characteristics, social and family support, emotional aspects and comorbidities (age group, social support scale, family APGAR, depression, anxiety, gestational diabetes mellitus and systemic arterial hypertension). The response variable was the presence of overweight/obesity in pregnant women, categorized as yes or no.
Initially, descriptive analyzes of all variables investigated were performed using simple and relative frequencies. Next, bivariate analyses were performed between the dependent variable and each independent variable, adopting the Poisson regression model with robust variance. Crude and adjusted Prevalence Ratios (PR) were estimated with their respective CI95%. Variables with
p≤0.20 were selected for multiple analysis.
In the final model adjusted for each level, only the variables that obtained
p<0.05 remained after controlling the variables of the same block and for those that showed significance in hierarchically higher blocks. The Deviance test was used to assess the quality of the model fit. Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS), version 20.0, adopting the CI95%.
The study complied with the ethical principles of the
Conselho Nacional de Saúde (CNS) (National Health Council Resolution) No. 466/2012 was approved by the Research Ethics Committee of the
Universidade Estadual de Montes Claros through substantiated opinions nº 2,483,623/2018 and 3,724,531/2019 on November 25, 2019 (CAAE 80957817.5.0000.5146).
ResultsA total of 1,279 pregnant women participated in this study. The selection process of the participants evaluated is shown in Figure 2.
There was a predominance of pregnant women who self-reported as mixed, black and yellow skin color (88.9%), elementary/high school education (80.1%) and marital status with a partner (76.7%). Regarding obstetric characteristics, 87.6% of the participants had less than 14 weeks of gestation. The age group of 21 to 30 years old (48.7%) obtained the highest percentage. The other socioeconomic and demographic characteristics, social and family support, emotional aspects and comorbidities are described in Table 1.
The prevalence of overweight/obesity was 45.3% among the evaluated pregnant women. Figure 3 demonstrates the classification on nutritional status.
Table 1 also presents the results of the bivariate analysis between overweight/obesity and the independent variables evaluated. The variables that showed statistically significant associations with the outcome up to 20% were: age group, marital status, occupation, income, previous pregnancies, gestational age, anxiety, gestational diabetes mellitus and systemic arterial hypertension.
After adjusting the model, overweight/obesity was associated with distal, intermediate and proximal level factors. The outcome analyzed was more prevalent among pregnant women who reported having a partner (PR=1.52; CI95%=1.24-1.86), family income above one minimum wage (PR=1.23; CI95%=1.04-1.46), one (PR=1.29; CI95%=1.07-1.54%) and two (PR=1.65; CI95%=1.39-1.95%) previous pregnancies, aged 21-30 years old (PR=1.72; CI95%=1.30-2.27) and over 30 years old (PR=2.26; CI95%=1.70-3.01), who had gestational diabetes mellitus (PR=1.43; CI95%=1.21-1.69) and systemic arterial hypertension (PR=1.29; CI95%=1.04-1.61). The Deviance test indicated that the model had adequate goodness of fit (
p=0.650) (Table 2).
DiscussionIn this study, approximately half of the pregnant women analyzed were overweight/obese, an outcome that was associated with factors at the distal level (marital status and income), intermediate level (previous pregnancies) and proximal level (age group, gestational diabetes mellitus and systemic arterial hypertension).
The high prevalence of gestational overweight/obesity in this investigation corroborates international studies found in Saudi Arabia, where a prevalence of 42.3% was observed;
4 in China, 43.2%;
5 and in Indonesia, where 50.7%
6 of the participants had excessive weight during pregnancy. In Brazil, a prevalence of 46.2% was found in pregnant women using the FHS of Colombo (Paraná State),
8 while in a study carried out in São Paulo State more than 70% of those evaluated were classified as overweight or obese.
7 It should be considered that the differences in the prevalence of overweight/obesity in pregnant women may be related to the different methodological criteria used in the screening of this condition and also to ethnic, demographic, social, economic, behavioral and cultural specificities between regions and countries.
However, this finding reiterates the importance of screening and monitoring nutritional status in pregnancy during prenatal care at the FHS. This is because overweight/obesity is a relevant public health problem in Brazil
2 and worldwide,
3 as it favors the development of gestational complications, contributing to obesity in subsequent pregnancies, in addition to increasing the chances of occurrence of gestational diabetes mellitus, systemic arterial hypertension, preeclampsia and cesarean section,
23-25 as well as the risk for perinatal morbidity and mortality.
11,23Regarding the factors associated with overweight/obesity, the demographic characteristics marital status and family income, present at the distal level of the hierarchical model, were associated with the outcome studied. That being said, pregnant women in this study who lived with a partner had a higher prevalence of overweight/obesity. The opposite result was found in a previous study developed in the city of Horizonte, Ceará State, in which pregnant women without a partner were more likely to gain insufficient weight during pregnancy. This can be justified by the fact that marital status is an aspect to be taken into account, since the absence of a father figure can bring financial instability and constitute a risk factor for the pregnant woman's nutritional status.
26 On the other hand, it is suggested that having a partner during pregnancy can generate a comfort zone for the pregnant woman, which provides a relaxation in the pattern of behavior and unhealthy habits. Thus, the pregnant woman's nutritional status is put at risk.
The association between higher income and overweight/obesity registered in this study was similar to the result identified in a previous study with Brazilian pregnant women.
2 One hypothesis for this finding is that women with better economic status may have greater access to and consumption of food, especially processed and industrialized food, which leads to the development of overweight and obesity. On the other hand, a systematic review indicated a relation between living in high-poverty neighborhoods and gestational overweight.
15 This finding demonstrates that more epidemiological evidence is needed to elucidate the interrelationship between socioeconomic status, diet and obesity in pregnant women.
At the intermediate level, the presence of previous pregnancies was associated with the investigated event. This result was also found in pregnant women who used health units in Colombo (Paraná State).
8 One explanation for overweight in women with more previous pregnancies is that the body fat accumulated during the first pregnancy is not lost between pregnancies. This weight accumulation increases progressively with the number of children.
8Regarding the proximal level of the hierarchical model, the age group variable and aspects of comorbidities, such as gestational diabetes mellitus and hypertension, were associated with a higher prevalence of overweight/obesity. Thus, the age groups (21 to 30 years old and over 30) are women of childbearing age and showed statistically significant associations with gestational overweight/obesity. This finding is similar to the results found in a national study that indicated a high prevalence of overweight in women of childbearing age before pregnancy, with 24.9%, 36% and 45.7% of women in the age groups of 18-24, 25-34 and 35-44 years old, respectively.
27 A study conducted in Guarapuava, Paraná State found a similar situation, in which young adult pregnant women (20 to 34 years old) were overweight or obese before pregnancy and this finding was associated with low frequency at the health services, lack of physical activities and insufficient care with food.
28 In the context of public health, prenatal care within the FHS is a cost-effective strategy to control the prevalence of overweight/obesity among women of childbearing age, in order to reduce harm to the pregnant woman/child and mother/child binomial, with timely interventions on health promotion, prevention and treatment for gestational overweight.
8,14,29The comorbidities on gestational diabetes mellitus and systemic arterial hypertension, identified in this study as explanatory variables associated with overweight/obesity, were also found in 1,183 Portuguese pregnant women
12 and in 912 Polish pregnant women.
24 Previous studies conducted with Indian and Chinese women found that excessive weight gain during pregnancy was associated with gestational diabetes mellitus.
23,25 In Brazil, an investigation conducted by Ferreira et al.
7 in São Paulo found that there is a 7.5 times higher chance of gestational diabetes mellitus among participants classified as obese. Due to physiological changes in the pattern of glucose metabolism during pregnancy, glucose tolerance is reduced, amplifying further the risk of developing diabetes mellitus in pregnant women with high BMI, which demonstrates metabolic deficiency and favors adverse pregnancy outcomes.
12Regarding hypertension during pregnancy, a longitudinal cohort study with 1,441 pregnant women found that obese women had a 2.4 times higher risk of developing hypertension, even after controlling excessive weight gain.
30 Similarly, a study developed in Poland reported that the highest risk of hypertension was in pregnant women who were overweight during pregnancy, with pre-pregnancy BMI being the most likely factor to increase the likelihood of developing this type of hypertension.
24Finally, gestational overweight and obesity are independent risk factors for hypertensive syndromes
30 and gestational diabetes mellitus.
24 The impact of these two comorbidities in the gestational period results in pre-eclampsia and/or eclampsia, macrosomic babies, cesarean section, preterm delivery, in other words, there is a high risk of developing adverse maternal-fetal and infant health outcomes.
12,23Social/family support and emotional aspects were not associated with the event in the evaluated pregnant women. A possible explanation for the result found may be that the women evaluated in the present study have encountered difficulties in the perception of social support, who sometimes, for cultural reasons, do not understand that the husband needs to help with childcare, chores and other activities that are culturally related to women.Social support is a dynamic process of support promoted by family and friends, in order to make the pregnant woman feel cared for and supported in her necessities, which can contribute in providing the necessary comfort for her well-being.
10 With regard to emotional aspects, it should be noted that starting a pregnancy with a high BMI or having a high BMI in the first trimester favors excessive weight gain throughout pregnancy and this may be related to the occurrence of depressive symptoms.
11It is hoped that the results found can sensitize the PHC multiprofessional team about its role in prevention, monitoring and of overweight/obesity treatment, given the characteristics of universal access, longitudinal link and intersectoral approaches,
29 which can contribute to the pregnant woman's understanding the impact of overweight has on her health and the child's.
14 It is important to warn future pregnant women about the complications of starting a pregnancy with a high BMI, or having an increased BMI in the first trimester, as these characteristics favor excessive weight gain throughout pregnancy and can have negative repercussions for the pregnant woman and the baby.
11,24 Reproductive planning and preconception consultation provide identification of the risk of overweight/obesity prior to pregnancy and can predict excessive weight gain during prenatal care. Such planning can be carried out by FHS professionals, with a view to preventing obstetric and neonatal complications, promoting pregnant women's cardiovascular health and building better maternal and child health indicators.
2This study has some limitations to be recognized, such as the use of self-report and information from the pregnant woman's health booklet. Failures in BMI records hampered the data collection process, which should be considered in future studies on the subject. Despite this, this is a population-based study with a significant sample size, which strengthened the associations found. The analytical approach using a hierarchical model provided a better understanding of the determinants of the outcome investigated. For future investigations, we suggest the evaluation of gestational weight gain. Longitudinal studies are suggested to verify the causal relation between the associated factors and the overweight/obesity outcome, especially considering pre-gestational conditions and the pregnant woman's regional/cultural characteristics.
In summary, there was a significant prevalence of overweight/obesity in the evaluated pregnant women. The factors associated with this outcome were sociodemographic and related to health conditions: living with a partner, income above one minimum wage, presence of previous pregnancies, age between 21 and 30 years old and over 30, gestational diabetes mellitus and systemic arterial hypertension. Especially in the context of the FHS, the results found in this study highlight the importance of monitoring nutritional status during pregnancy. The presence of overweight/obesity in the gestational period may be a reflection of unsuccessful dietary counseling, lack of follow-up, as well as individual factors. In this sense, early interventions are recommended to prevent complications for both the pregnant woman and the newborn, since the researched event is considered a public health problem due to its negative outcomes for maternal and child health. Given this context, it is necessary to outline new strategies, including early interventions, awareness of the importance of adequate gestational nutritional status and nutritional education for pregnant women along with the FHS teams' support.
References1. Campos CAS, Malta MB, Neves PAR, Lourenço BH, Castro MC, Cardoso MA. Gestational weight gain, nutritional status and blood pressure in pregnant women. Rev Saúde Pública. 2019; 53: 57.
2. Monteschio LVC, Marcon SS, Arruda GO, Teston EF, Nass EMA, Costa JRB, et al. Excessive gestational weight gain in the Brazilian Unified Health System. Acta Paul Enferm. 2021; 34: eAPE001105.
3. Chen C, Xu X, Yan Y. Estimated global overweight and obesity burden in pregnant women based on panel data model. PLoS One. 2018 Aug; 13 (8): e0202183.
4. Fayed A, Wahabi HA, Esmaeil S, Elkouny R, Elmorshedy H, Bakhsh H. Independent effect of gestational weight gain and prepregnancy obesity on pregnancy outcomes among Saudi women: a sub-cohort analysis from Riyadh mother and baby cohort study (RAHMA). PloS One. 2022 Jan; 17 (1): e0262437.
5. Ma D, Szeto IMY, Yu K, Ning Y, Li W, Wang J, et al. Association between gestational weight gain according to prepregnancy body mass index and short postpartum weight retention in postpartum women. Clin Nutr. 2015 Apr; 34 (2): 291-5.
6. Soltani H, Lipoeto NI, Fair FJ, Kilner K, Yusrawati Y. Pre-pregnancy body mass index and gestational weight gain and their effects on pregnancy and birth outcomes: a cohort study in West Sumatra, Indonesia. BMC Women's Health. 2017 Nov; 17 (1): 102.
7. Ferreira LAP, Piccinato CA, Cordioli E, Zlotnik E. Pregestational body mass index, weight gain during pregnancy and perinatal outcome: a retrospective descriptive study. Einstein (São Paulo). 2020; 18: 1-6.
8. Manera F, Hofelmann DA. Overweight in pregnant women attending health centers in Colombo, Paraná, Brazil. DEMETRA. 2019 Set; 14: e36842.
9. Magalhães EI, Maia DS, Bonfim CF, Netto MP, Lamounier JA, Rocha DS. Prevalence and factors associated with excessive weight gain in pregnancy in health units in the southwest of Bahia. Rev Bras Epidemiol. 2015; 18 (4): 858-69.
10. Maranhão TA, Gomes KROS, José MN. Fatores que influenciam as relações familiares e sociais de jovens após a gestação. Cad Saúde Pública. 2014; 30 (5): 998-1008.
11. McDonald SD, Yu ZM, Van Blyderveen S, Schmidt L, Sword W, Vanstone M, et al. Prediction of excess pregnancy weight gain using psychological, physical, and social predictors: a validated model in a prospective cohort study. PLoS One. 2020 Jun; 15 (6): e0233774.
12. Bodnar LM, Hutcheon JA, Platt RW, Himes KP, Simhan HN, Abrams B. Should gestational weight gain recommendations be tailored by maternal characteristics?. Am J Epidemiol. 2011; 174 (2): 136-46.
13. Alves P, Malheiro MF, Gomes JC, Ferraz T, Montenegro N. Riscos da obesidade materna na gravidez: um estudo caso-controle em uma população obstétrica portuguesa. Rev Bras Ginecol Obstet. 2019; 41 (12): 682-7.
14. Sato APS, Fujimori E. Nutritional status and weight gain in pregnant women. Rev Latino-Am Enferm. 2012; 20 (3): 462-8.
15. Silva TPR, Viana TGF, Duarte CK, Inácio MLC, Velasquez-Melendez G, Pessoa MC, et al. Environmental factors associated with excessive gestational weight gain: a meta-analysis and systematic review. Ciênc Saúde Colet. 2023; 28 (1): 171-80.
16. Griep RH, Chor D, Faerstein E, Werneck GL, Lopes C. Validade de constructo de escala de apoio social do Medical Outcomes Study adaptada para o português no Estudo Pró-Saúde. Cad Saúde Pública. 2005; 21 (3): 703-14.
17. Smilkstein G. The family APGAR: a proposal for a family function test and its use by physicians. J Fam Pract. 1978; 6 (6): 1231-9.
18. Gonçalves B, Fagulha T. The portuguese version of the Center for Epidemiologic Studies Depression Scale (CES-D). Eur J Psychol Assess. 2004; 20 (4): 339-48.
19. Fioravanti-Bastos ACM, Cheniaux E, Landeira-Fernandez J. Development and validation of a short-form version of the Brazilian State-trait Anxiety Inventory. Psicol Reflex Crit. 2011; 24 (3): 485-94.
20. Atalah SE, Castillo LC, Castro SR, Aldea PA. Propuesta de um nuevo estándar de evaluación nutricional em embarazadas. Rev Méd Chile. 1997; 125 (12): 1429-36.
21. Ministério da Saúde (BR). Vigilância alimentar e nutricional - SISVAN: orientações básicas para a coleta, processamento, análise de dados e informação em serviços de saúde. Brasília (DF): Ministério da Saúde; 2004. [access in 2022 Fev 2]. Available from:
http://189.28.128.100/nutricao/docs/geral/orientacoes_basicas_sisvan.pdf22. Santos SFM, Costa ACC, Araújo RGPS, Silva LAT, Gama SGN, Fonseca VM. Factors associated with the adequacy of gestational weight gain among Brazilian teenagers. Ciênc Saúde Colet. 2022; 27 (7): 2629-42.
23. Bhavadharini B, Anjana RM, Deepa M, Jayashree G, Nrutya S, Shobana M, et al. Gestational Weight Gain and Pregnancy Outcomes in Relation to Body Mass Index in Asian Indian Women. Indian J Endocrinol Metab. 2017; 21 (4): 588-93.
24. Lewandowska M, Więckowska B, Sajdak S. Pre-pregnancy obesity, excessive gestational weight gain, and the risk of pregnancy-induced hypertension and gestational diabetes mellitus. J Clin Med. 2020 Jun; 9 (6): 1980.
25. Senbanjo OC, Akinlusi FM, Ottun TA. Early pregnancy body mass index, gestational weight gain and perinatal outcome in an obstetric population in Lagos, Nigeria. Pan Afr Med J. 2021; 39: 136.
26. Silva L, Alexandre M, Calvalcante AC, Arruda S, Sampaio R. Ganho de peso adequado versus inadequado e fatores socioeconômicos de gestantes acompanhadas na atenção básica. Rev Bras Saúde Matern Infant. 2019; 19 (1): 107-14.
27. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância de Doenças e Agravos não Transmissíveis e Promoção da Saúde. VIGITEL Brasil 2016: Vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico: Estimativas sobre frequência e distribuição sociodemográfica de fatores de risco e proteção para doenças crônicas nas capitais dos 26 estados brasileiros e no Distrito Federal em 2016. Brasília (DF): Ministério da Saúde; 2017. [access in 2022 Fev 2]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/vigitel_brasil_2016_fatores_risco.pdf28. Soares LG, Tomen KB, Paris MC, Lentsck MH, Soares LG, Abreu IS, et al. Gestação de alto risco e obesidade em um Município do Paraná. Braz J Dev. 2021; 7 (2): 11744-56.
29. Marques ES, Leite TH, Azeredo CM, Cunha DB, Verly Júnior E. Effective strategies for prevention, control, and treatment of obesity in primary health care setting for adolescents, adults, and elderly people: a protocol for systematic review and meta-analysis. Medicine (Baltimore). 2018 Jun; 97 (22): e10925.
30. Ruhstaller KE, Bastek JA, Thomas A, Mcelrath TF, Parry SI, Durnwald CP. The effect of early excessive weight gain on the development of hypertension in pregnancy. Am J Perinatol. 2016 Oct; 33 (12): 1205-10.
Received on October 6, 2022
Final version presented on June 27, 2023
Approved on July 6, 2023
Associated Editor: Melânia Amorim
Acknowledgements: We would like to thank the
Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) for the financial support on the PhD scholarship (code 001).
Authors’ contribution: David LS, Lima CA and Santos VM: conception and design of the study, supervision, logistics and data collection, drafting of the manuscript. Pena GG, Brito MFSF and Silva RRV: conception and design of the study, statistical analysis, data interpretation and critical review of the manuscript. Pinho L: guidance on all stages of the study, conception and design of the study, statistical analysis and interpretation of data, critical revision of the manuscript. All authors have approved the final version of the article and declare no conflict of interest.


 ; Cássio de Almeida Lima2
; Cássio de Almeida Lima2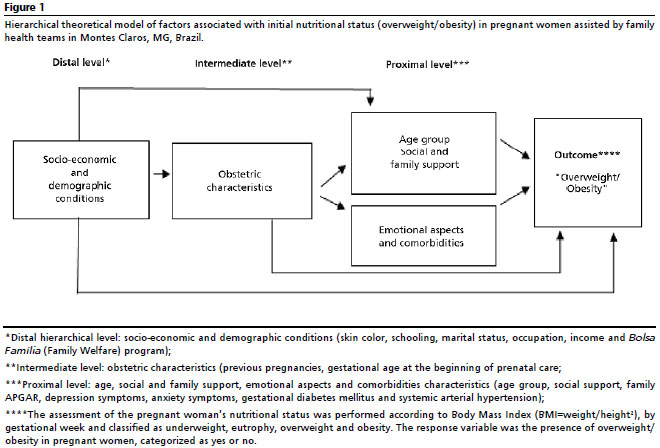









 Ler em português
Ler em português