ABSTRACT
OBJECTIVES: to analyze the nutritional status and temporal trend of the coverage of Brazilian adolescents monitored in the Food and Nutritional Surveillance System in the period 2008-2019.
METHODS: ecological study of temporal series with SISVAN data collected from 2008 to 2019 with 45,869.266 registration. Body mass index data were collected and the registration coverage of adolescents monitored by the system was calculated. The percentage of annual variation in coverage and nutritional status was estimated using Prais-Winsten regression, with a significance level of 5%.
RESULTS: an increase in the prevalence of obesity was observed between 2008 and 2019, during this period thinness remained stable in Brazil. National coverage evolved from 9.3% in 2008 to 19.6% in 2019, with an annual variation of 9% and a statistically significant increase trend. In Brazil, obesity in this age group increased between 2008 and 2019, with an annual variation of 8.7% (CI95% = 7.8-9.6).
CONCLUSION: modifications were observed in nutritional status suggest the occurrence of nutritional transition in the adolescents' population. The percentage of coverage available in the system has growth potential, however, the current scenario impacts on a possible insufficient analysis to support the elaboration and reorientation of public policies.
Keywords:
Food and nutritional surveillance, Public health care service coverage, Adolescents, Nutritional status
RESUMO
OBJETIVOS: analisar o estado nutricional e a tendência temporal da cobertura de adolescentes brasileiros acompanhados no Sistema de Vigilância Alimentar e Nutricional no período de 2008-2019.
MÉTODOS: estudo ecológico de séries temporais com dados do SISVAN coletados no período de 2008 a 2019 com 45.869.266 de registos. Foram coletados dados de índice de massa corporal e calculadas as coberturas dos registros dos adolescentes acompanhados pelo sistema. Estimou-se a percentagem da variação anual da cobertura e estado nutricional pela regressão de Prais-Winsten, com nível de significância de 5%.
RESULTADOS: observa-se crescimento da prevalência de obesidade entre 2008 a 2019, nesse período a magreza manteve-se estável no Brasil. A cobertura nacional evoluiu de 9,3% em 2008 para 19,6% em 2019, com variação anual de 9% e tendência de aumento estatisticamente significativa. No Brasil, a obesidade nessa faixa etária apresentou um aumento entre os anos de 2008 e 2019, com uma variação anual de 8,7% (IC95%= 7,8-9,6).
CONCLUSÃO: modificações observadas no estado nutricional sugerem a ocorrência da transição nutricional na população de adolescentes. O percentual de cobertura disponível no sistema tem potencial de crescimento, entretanto, o atual cenário impacta em possível análise insuficiente para subsidiar a elaboração e reorientação de políticas públicas.
Palavras-chave:
Vigilância alimentar e nutricional, Cobertura de serviços públicos de saúde, Adolescentes, Estado nutricional
IntroductionThe
Política Nacional de Alimentação e Nutrição (PNAN) (National Food and Nutrition Policy), in its third guideline, contemplates the
Vigilância Alimentar e Nutricional (VAN) (Food and Nutrition Surveillance), which is based on describing and predicting food and nutritional trends of the Brazilian population. This guideline highlights the
Sistema de Vigilância Alimentar e Nutricional (SISVAN) (Food and Nutrition Surveillance System) to monitor food consumption and nutritional status (NS) of users of the
Sistema Único de Saúde (SUS) (Public Health System) throughout their lives.
1In order to integrate information on weight status and food consumption, the online platform (SISVAN Web)
2 was created to store and compile data, identifying groups with higher nutritional risk, and benefits the planning on priority actions in the scope of care and management. In the life cycle, stratification is taken in consideration: preschool children (zero to four years old), school-age children (five to nine years old), adolescents (ten to 19 years old), adults (20-59 years old), elderly (60 years old and above), and pregnant women. SISVAN recommends the use of the body mass index (BMI) as a method to classify the nutritional status, for adolescents, indicators as height for age (H/A) and body mass index for age (BMI/A) are used.
3In the case of adolescents, nutritional status registration, including weight and height data collection, may be linked to the
Programa Saúde na Escola, Estratégia Saúde da Família (ESF) (School Health Program and Family Health Strategy) or cash transfer program, in which adolescentes who are in school are monitored by professionals from the basic health network. This is an inter-institutional plan involving the Ministry of Health and the Ministry of Education and aims to "contribute to the comprehensive training of students in the public education network through prevention, promotion and health actions".
4The adolescents' nutritional status impacts their adult life, since it is a crucial period for their development and may increase the chances of developing chronic diseases. Obesity in adolescence may be related to various risks of associated diseases, such as diabetes and cardiovascular diseases (CVD), as well as cancer, respiratorial, dermatological, and orthopedic problems resulting from genetic, environmental, and inadequate lifestyle factors. On the other hand, malnutrition can cause weakness of the immune system, reduce muscle mass, delay physical and mental development, and permanent damage to their health. Thus, more attention should be paid to the health conditions of this age group, since the nutritional status directly impacts the adults' health and public expenditure in the country.
5The
Pesquisa Nacional de Orçamentos Familiares (POF) (National Survey of Family Budgets) conducted in 2008-2009 demonstrated that overweight already affected 21.5% and 19.4% of the Brazilian male and female adolescents, respectively.
6 Furthermore, according to the POF 2008-2009, 5.8% and 4.0% of the Brazilian male and female adolescents, respectively, were obese. The
Pesquisa Nacional de Saúde do Escolar (PeNSE 2009) (National School Health Survey) which evaluated anthropometric measures of 58,971 adolescents (13 to 19 years old), observed that overweight was 23.0% and obesity at 7.3%, in the South and Southeast of the country are higher.
7 More recently, the PeNSE 2015 observed levels of overweight in boys at 23.6% and obesity at 8.3%, and in females, 23.8% were overweight and 7.3% were obese.
8Despite the importance of this nutritional surveillance in the primary care, in the Brazilian literature, a gap is identified, because previous studies have focused on isolated geopolitical scenarios.
9 However, this study analyzes the nutritional status of this group in the country and its macro-regions, with data up to 2019, a differential in the existing studies. The
Sistemas de Informação (SIS) (Information Systems Coverage) is considered a dimension of quality and has been widely studied with SISVAN data. However, the management of the quality of SIS information in Brazil is not yet organized and nor systematic. Knowing the health status of a population is important for assessing priorities and creating programs. Such indicators facilitate the analysis of information, but its quality will depend on the accuracy of the information systems.There is no way to influence social control over what is little known.
10 This study justifies itself because it will help reduce gaps in the information about the adolescents' nutritional status in contributing in the decision-making in public policies.In this logic, this study analyzes the temporal trend of coverage and nutritional status of adolescents in Brazil and in macro-regions, considering the data available in the
Sistema de Vigilância Alimentar e Nutricional (Food and Nutrition Surveillance System) from 2008 to 2019.
MethodsEcological study, conducted with secondary data from SISVAN, from 2008 to 2019, in Brazil and its five macro-regions (North, Northeast, South, Southeast and Midwest) as analysis unit.
The data on nutritional status and coverage of adolescents monitored in the system was taken in consideration, making it possible by consultations on the consolidated reports of public access and available at the SISVAN Web e-mail address (https://sisaps.saude.gov.br/sisvan/relatoriopublico/index). On the platform, these annual reports are stored with results from the last assessment of the year, each adolescent assessed is entered only once in the database, this information is derived from the food and nutritional surveillance actions that recommends the assessment of nutritional status indicators (anthropometric indexes and food consumption markers). All the available registrations on the platform were used in the analyses. For this study, the adolescents' life cycle phase was selected, this is, individuals aged 10 years or older and 20 years or younger, according to the World Health Organization (WHO).
11BMI for age is internationally recommended for individual and collective diagnosis of nutritional disorders in adolescence, is calculated as recommended by the WHO, incorporates the information of the individual's age, has been validated as an indicator of total body fat in the superior percentiles, and provides continuity with the indicator used among adults.
3The cut points for the BMI for adolescents' age indicator follow the following classification: marked thinness (< Percentile 0.1); thinness (≥ Percentile 0.1 and < Percentile 3); Eutrophy (> Percentile 3 and < Percentile 85); Overweight (> Percentile 85 and ≤ Percentile 97); Obesity (> Percentile 97 and ≤ Percentile 99.9); Severe obesity (> Percentile 99.9).
For this study, the main nutritional deviations in this age group will be evaluated: thinness (sum of Accentuated thinness and thinness) and obesity (sum of Obesity and Severe Obesity).
The monitoring of the nutritional status was analyzed by calculating the total coverage, referring to the percentage of individuals monitored by SISVAN Web. The value was obtained by the number of individuals with nutritional status registration (numerator) divided by the SUS user population (denominator), multiplied by 100.
The number of individuals followed-up by SUS was obtained by subtracting from the total Brazilian population assisted by health insurance plans.
12 Data were collected and extracted from the
Instituto Brasileiro de Geografia e Estatística (IBGE) (Brazilian Institute of Geography and Statistics) (total resident population) and from the
Agência Nacional de Saúde Suplementar (ANS) (National Agency for Supplementary Health) (private health plans)
13 in Excel
® spreadsheet format. For the calculation and sorting of the data, the javascript programming language was used. The database, compilation, analysis, preparation of tables and graphs were performed in the Power BI program and its visualization is on a web page.
To determine the temporal variation of the indicators, we first calculated the prevalence for each of the strata each year. Then, Prais-Winsten regression models were used to control autocorrection of residuals regression between the years analyzed, assuming a significance level of 5%.
14 The mean annual variation (AV) of coverage and each category of nutritional status was calculated from the following formula:[-1 + (10
β)] x 100, where β is base 10 logarithm. Non-significant
p values (
p≥0.05) indicated stable trend; significant
p values (
p≤0.05), increasing or decreasing trend, according to positive or negative annual change, respectively.
The study project was approved by the Ethics Committee on Human Research of the
Universidade de Fortaleza (Coética/Unifor): Opinion nº 4,348.452, and Certificate of Submission for Ethical Consideration nº 31540320.9.1001.5052.
ResultsBetween 2008 and 2019, a total number of 45,869,266 million adolescents were followed up by SISVAN, of these, 45.5% correspond to individuals followed up from the Northeast region, 24.5% in the Southeast, 15% in the North, 9.1% in the South, and 5.7% were from the Midwest region. Table 1 presents registrations of the follow-ups per macro-regions. Developed graphs and tables are available on the web page.
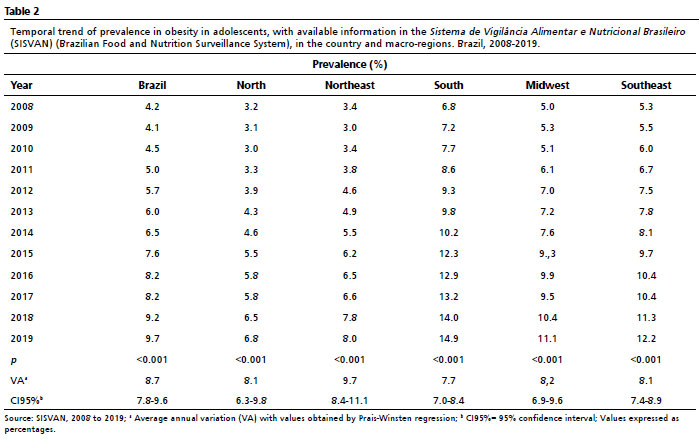
15 As for the classification of nutritional status, we identified an increasing temporal trend in the prevalence of obesity among adolescents nationally and in macro-regions. In Brazil, obesity in this age group showed an increase between 2008 and 2019, with an annual change of 8.7% (CI95%= 7.8-9.6). The Southern region showed the highest prevalence of obesity, compared to the other macro-regions. Obesity in the regions rose in a similar way (Table 2).
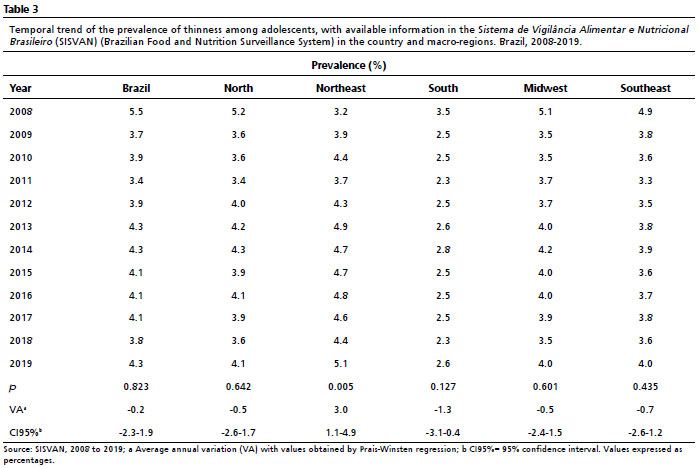
In contrast, the prevalence of thinness was stable between years. Nationally, the percentage of underweight increased from 5.5% in 2008 to 4.3% in 2019, with a non-significant annual change of -0.2% (CI95%= -2.3 - 1.9). The Northeast region differs from the Brazilian pattern and the other regions with a significant increasing annual trend in thinness. Among the macro-regions, the North and Northeast regions exhibited the highest percentages of thinness in all strata analyzed (Table 3).
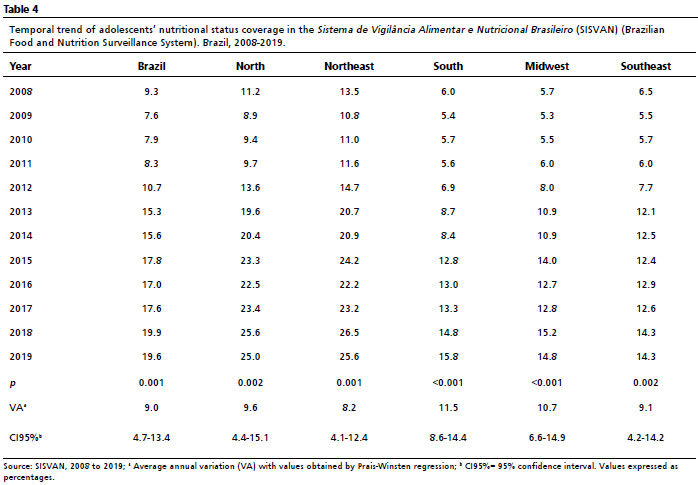
The percent coverage of adolescent nutritional status nationally and by macroregions, showed percentages from 9.3% (2008) to 19.6% (2019), with an annual change of 9.0% (CI95%= 4.7-13.4). In the regions and in Brazil, the p values showed positive and significant, indicating a trend of growth in coverage for all strata analyzed, with the highest national coverage and in all macro-regions detected in 2018 (Table 4).
DiscussionA modest coverage of the nutritional status of adolescents by SISVAN is observed with an increasing temporal trend in Brazil and in the five macro-regions analyzed. Regarding the classification of nutritional status, there was an increase in the prevalence of obesity and stability of thinness. Higher rates of obesity were identified in the South region and low weight in the North and Northeast regions.
An increase of obesity was observed in all the regions and the South region followed by the Southeast region are the ones that presented the highest percentages of adolescents living with obesity.
In this study was observed that among the macro-regions, the Northeast region showed the highest percentages of thinness and increasing significance of annual variation. Different findings were found in an epidemiological study that showed an average malnutrition rate of 1.9% and a decrease in malnutrition followed by an increase in overweight.
16The causes of obesity are not only individual or family, but environmental and social, and its main challenges are the interest of food conglomerates, political lack of interest in combating it, and the lack of pressure from civil society.
17In this context, the school has been pointed out as an opportune environment for health education programs, which is related to its inclusion in all dimensions of learning: teaching, home-school-community relations, physical and emotional environment.
18 Currently, changes in the school environment and in the policies directed to this space have been the measures recurrently suggested to prevent obesity at childhood. One example is the
Programa Saúde na Escola (PSE) (School Health Program), which is a partnership between the Ministries of Health and Education.
19 Since 2013, a list of essential PSE actions has been established that are mandatory for cities, and one of the actions is the
Linha de Cuidados para Prevenção e Tratamento do Sobrepeso e da Obesidade (Care Line for Prevention and Treatment of Overweight and Obesity). At the national level, the actions carried out in schools with the theme of healthy eating had increased from 2017 to 2019.
20Another existing initiative that reaches the school environment is the
Estratégia de Prevenção e Atenção à Obesidade Infantil (PROTEJA) (Strategy for Prevention and Care of Childhood Obesity), instituted by Ordinance GM/MS Nº 1,862, August 10, 2021, is an intersectoral Brazilian strategy that aims to detain the progress in childhood obesity and contribute to the care and the improvement of children's health and nutrition.
21The increase in the prevalence of overweight and the stability of low weight and appropriate weight indicate the occurrence of a nutritional transition for the adolescents' population. Initially identified among the adult population, this process, which has been ongoing in the country for more than 40 years, is characterized by a decline in the prevalence of malnutrition and an increase in the occurrence of overweight. Initially, a higher prevalence of overweight and obesity was observed in the Brazilian regions with a better socioeconomic level. In the last decade, the occurrence of overweight has been increasing in the low-income adult population, one of the causes was the increased consumption of ultra-processed food, to the detriment of healthy food, such as beans.
22The
Pesquisa Nacional de Saúde dos Escolares (PeNSE) (National School Health Survey) of 2015 identifies that the highest prevalence of overweight was observed in adolescents who classify themselves black or indigenous, from the South region, from urban areas, and in the low income quintile.
23 Tens of million of people have rights and duties and need opportunities to fully develop their potential. Brazil has some of the most advanced legislation in the world regarding children and adolescents' protection. However, it is necessary to prioritize public policies capable of rejecting and overcoming geographical, social, and ethnic inequalities in the country.
16The low coverage of the nutritional status of adolescents by SISVAN from 11.33% in 2008 to 11.51% in 2012, with no significant growth trend, was observed in the first six years of implementation of SISVAN Web (2008 to 2013).
24 The group of adolescents ranked fourth in coverage in 2012. Regarding the regions with the highest coverage, the North and Northeast regions stand out.
The
Informe Situacional da Geral da Coordenadoria-Geral de Alimentação e Nutrição (CGAN) (Situational Report of the General Coordination of Food and Nutrition), when comparing the expansion of the nutritional coverage of the total population monitored by SISVAN Web in 2014 and 2017, indicated an increase in the percentage of coverage in most of the Brazilian states. The coverage of the country in 2017 reached 14.1%, on the other hand, the adolescentes coverage was 17.6%. Although the coverage of adolescents is higher than the overall coverage of all phases of the country, there is still space for growth.
25 Even though the coverage of adolescents is modest, SISVAN data are similar to those of other national surveys such as POF and PeNSE, which is an indication that it is being representative.
6,8Despite the limitations presented by the modest coverage, several are the potentialities of SISVAN that can be highlighted, such as the integration with other SUS health information systems, generating reports, and its coverage in all Brazilian cities and in all the stages of life cycles.
26The main obstacles on high coverage and the use of SISVAN by primary care are: lack of human resources, physical structure and logistics; complexity of implementation; poor management and little political engagement, and problems with the matrix support for the teams responsible for supplying the system.
27In a study carried out in Natal, capital of Rio Grande do Norte, health professionals working with the PSE reported that the biggest difficulties were the lack of material and financial resources (50.5%), intersectorial disarticulation (26.7%), and followed by the excess of activities in the work process (17.1%).
28 Similarly, in a study conducted in the cities of the
Superintendência Regional de Saúde de Belo Horizonte (Regional Superintendence of Health in Belo Horizonte), the main problems faced in the cities regarding data collection for food and nutritional surveillance and data entry in SISVAN Web were: problems with the internet (62.2%); lack of training for data collection (54.1%); professional turnover (51.4%) and extensive user's registration form in the system (51.4%). Other problems cited with greater frequency were: lack of anthropometric equipment (43.2%), lack of professionals for typing (43.2%), centralization of typing in the Municipal Health Secretary (43.2%) and poor conditions of the equipment (40.5%).
29 Also regarding to the higher percentages of coverage presented by the North and Northeast, it may be related to the fact that some public policies were directed to locations with higher levels of poverty, hunger, and child malnutrition. Both the broad coverage of the ESF and
Bolsa Família Program (Welfare Program) beneficiaries in these regions; as well as the existence of collaborating groups/centers and projects that gave origin to SISVAN, especially in the Northeast, are examples.
22Despite being important, our results present limitations, such as not allowing conclusions at the individual level, since this is an investigation of ecological analysis aggregates, and this is one of the factors that may interfere in the interpretation of the findings. The use of secondary data also shows as a restriction, because they come from different sources and, consequently, may have an inconsistency in the credibility of the information, resulting from errors in collection, typing, under-registrations, and among others.
The low percentage of coverage, with a significant growth trend for the adolescents' population, observed in the first 12 years of SISVAN indicates that its use is in the process of adaptation, resulting in the production of insufficient data to support the development and adjustment of public policies to prevent diseases/illnesses and health promotion and maintenance for this public. We identified regional inequalities in the distribution of nutritional status classifications, with higher rates of overweight in the South region and underweight in the North and Northeast regions. The tendency of prevalence in obesity growth in all Brazilian macro-regions suggests the occurrence of a nutritional transition process for the adolescents' population.
References1. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Política Nacional de Alimentação e Nutrição. 1
st ed, 1
st. reimp. Brasília (DF): Ministério da Saúde; 2013. [access in 2021 Fev 2]. Available from:
http://bvsms.saude.gov.br/bvs/publicacoes/politica_nacional_alimentacao_nutricao.pdf2. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Marco de referência da vigilância alimentar e nutricional na atenção básica. Brasília (DF): Ministério da Saúde; 2015. [access in 2021 Fev 2]. Available from:
http://189.28.128.100/dab/docs/portaldab/publicacoes/marco_referencia_vigilancia_alimentar.pdf3. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Orientações para a coleta e análise de dados antropométricos em serviços de saúde: Norma Técnica do Sistema de Vigilância Alimentar e Nutricional - SISVAN. Brasília (DF): Ministério da Saúde; 2011. [access in 2021 Fev 3]. Available from:
http://189.28.128.100/dab/docs/portaldab/publicacoes/orientacoes_coleta_analise_dados_antropometricos.pdf4. Brasil. Decreto nº 6.286, de 5 de dezembro de 2007. Institui o Programa Saúde na Escola - PSE, e dá outras providências. Brasília (DF): DOU de 6 de dezembro de 2007. [access in 2021 Fev 3]. Available from:
http://www.planalto.gov.br/ccivil_03/_ato2007-2010/2007/decreto/d6286.htm5. Moura ARLI, Santana AAA, Alencar JFR, Carvalho TR, Moraes JFVN. Custo da obesidade na adolescência entre 2008 e 2018 a partir dos dados do DATASUS. Rev Contexto Saúde. 2020; 20 (40): 175-80.
6. Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa Nacional por Amostra de Domicílios: Síntese de indicadores 2009 - PNAD. Rio de Janeiro: IBGE; 2009. [access in 2021 Fev 3]. Available from:
https://www.ibge.gov.br/estatisticas/sociais/populacao/9127-pesquisa-nacional-por-amostra-de-domicilios.html7. Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa Nacional de Saúde do Escolar. Rio de Janeiro: IBGE; 2009. [access in 2021 Fev 3]. Available from:
https://www.ibge.gov.br/estatisticas/sociais/educacao/9134-pesquisa-nacional-de-saude-do-escolar.html8. Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa Nacional de Saúde do Escolar 2015. Rio de Janeiro: IBGE; 2016. [access in 2021 Fev 3]. Available from:
https://www.ibge.gov.br/estatisticas/sociais/educacao/9134-pesquisa-nacional-de-saude-do-escolar.html9. Pessoa JT, Dias FMRS, Souza SABA, Souza NP, Leal VS, Silva SA,
et al. Food and nutritional surveillance: Coverage and characterization for children under 2 years of Northeast Brazil. Res Soc Dev. 2021 May; 610 (5): e27810514909.
10. Coelho Neto G, Chioro A. Afinal, quantos Sistemas de Informação em Saúde de base nacional existem no Brasil? Cad Saúde Pública. 2021; 37 (7): e00182119.
11. World Health Organization (WHO). Young people´s health: a challenge for Society. report of a WHO study group on young people and "health for all by the year 2000". Geneva: WHO; 1986. [access in 2021 Fev 3]. Available from:
https://apps.who.int/iris/handle/10665/4172012. Enes CC, Loiola H, Oliveira MRM. Cobertura populacional do Sistema de Vigilância Alimentar e Nutricional no Estado de São Paulo, Brasil. Ciênc Saúde Colet. 2014; 19 (5): 1543-51.
13. Nascimento FA, Silva AS, Jaime PC. Cobertura da avaliação do consumo alimentar no Sistema de Vigilância Alimentar e Nutricional Brasileiro: 2008 a 2013. Rev Bras Epidemiol. 2019; 22 (1): e190028.
14. Instituto Brasileiro de Geografia e Estatística (IBGE). Relatório populacional. Brasília (DF): IBGE; 2021. [access in 2021 Jan 30]. Available from:
https://www.ibge.gov.br/cidades-e-estados15. Software Power BI. 2020. [access in 2022 Set 13]. Available from: https://app.powerbi.com/view?r=eyJrIjoiMjA3N2Q5NzktNGUzMS00YTZiLThmZjItM2FmYjRmMzRjYTNmIiwidCI6ImIxNTZhNTQxLWUyMzYtNGVkYi05 MWJmLWZjYTI1YzcwMDRmOSJ9
16. Silva VM, Farias PR, Gonçalves VS. Consumo alimentar e obesidade em adolescentes brasileiros acompanhados na Atenção Básica: estudo ecológico com dados do Sistema de Vigilância Alimentar e Nutricional. Brasília: Universidade de Brasília (UnB); 2020. [access in 2021 Jan 30]. Available from:
https://repositorio.unb.br/handle/10482/4012317. Castro IRR. Obesity prevention and control: the urgent need for effective public policies. [Editorial]. Cad Saúde Pública. 2017; 33 (7): e00100017.
18. Fialho LMF. Escola promotora de saúde: qual a sua proposta? Instrumento: Rev Estud Pesq Educ. 2022; 24 (1): 6-24.
19. Diniz CBC, Feitosa AA, Coutinho BLM, Gomes SC, Sant'anna AL, Araújo AF,
et al. Adolescent nutrition monitoring the Health Program in School. J Hum Growth Dev. 2020; 30 (1): 32-9.
20. Carmo AS, Serenini M, Pires ACL, Pedroso J, Lima AMC, Silva AS,
et al. Promoção da Alimentação Adequada e Saudável no âmbito do Programa Saúde na Escola: implementação e contribuição do Programa Crescer Saudável. Saúde Debate. 2022; 46: 129-41
21. Ministério da Saúde (BR). Secretaria de Atenção Primária à Saúde. Departamento de Promoção da Saúde. PROTEJA: Estratégia Nacional para Prevenção e Atenção à Obesidade Infantil: orientações técnicas. Brasília (DF): Ministério da Saúde; 2022. [access in 2021 Jan 30]. Available from:
http://189.28.128.100/dab/docs/portaldab/publicacoes/orienta_proteja.pdf22. Melo SPSC, Cesse EAP, Lira PIC, Ferreira LCCN, Rissin A, Batista Filho M. Sobrepeso, obesidade e fatores associados aos adultos em uma área urbana carente do Nordeste Brasileiro. Rev Bras Epidemiol. 2020; 23 (1): e200036.
23. Costa CS, Flores TR, Wend A, Neves RG, Assunção MCF, Santos IS,
et al. Comportamento sedentário e consumo de alimentos ultraprocessados entre adolescentes brasileiros: Pesquisa Nacional de Saúde do Escolar (PeNSE), 2015. Cad Saúde Pública. 2018; 34: e00021017.
24. Nascimento FA, Silva AS, Jaime PC. Cobertura da avaliação do estado nutricional no Sistema de Vigilância Alimentar e Nutricional brasileiro: 2008 a 2013. Cad Saúde Pública. 2017; 33 (12): e00161516.
25. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Coordenação-Geral de Alimentação e Nutrição. Informe situacional sobre os programas de alimentação e nutrição e de promoção da saúde na atenção básica [
Internet]. 2017. [access in 2021 Jul 22]. Available from:
https://portaldeboaspraticas.iff.fiocruz.br/biblioteca/informe-situacional-sobre-os-programas-de-alimentacao-e-nutricao-e-de-promocao/26. Ministério da Saúde (BR). Universidade Federal de Sergipe. Guia para a organização da Vigilância Alimentar e Nutricional na Atenção Primária à Saúde. Brasília (DF): Ministério da Saúde; 2022. [access in 2022 Ago 22]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/guia_organizacao_vigilancia_alimentar_nutricional.pdf27. Lima JF, Schmidt DB. Sistema de vigilância alimentar e nutricional: utilização e cobertura na atenção primária. Rev Saúde Desenv. 2018; 12 (11): 315-33.
28. Medeiros ER, Pinto ESG, Paiva ACS, Nascimento CPA, Rebouças DGC, Silva SYB. Facilidades e dificuldades na implantação do Programa Saúde na Escola em um município do nordeste do Brasil. Rev Cuid. 2018; 9(2): 2127- 34.
29. Ferreira CS, Rodrigues LA, Bento IC, Villela MPC, Cherchiglia ML, César CC. Fatores associados à cobertura do Sisvan Web para crianças menores de 5 anos, nos municípios da Superintendência Regional de Saúde de Belo Horizonte, Brasil. Ciênc Saúde Colet. 2018; 23: 3031-40.
Received on August 21, 2022
Final version presented on May 30, 2023
Approved on June 5, 2023
Associated Editor: Paola Mosquera
Acknowledgments: We would like to thank the
Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) (National Council for Scientific and Technological Development) and the
Universidade de Fortaleza (UNIFOR) through the
Fundação Edson Queiroz for scholarships in scientific initiation.
Authors' contribution: Oliveira KP and Vieira LJES: study planning, analysis and discussion of results, final review of the manuscript; Carioca AAF: data collection, analysis and interpretation; Barbosa MEJP and Muniz LSS: literature review, data organization and initial draft of the manuscript. All authors approved the final version of the article and declare no conflict of interest.


 ; Antônio Augusto Ferreira Carioca2
; Antônio Augusto Ferreira Carioca2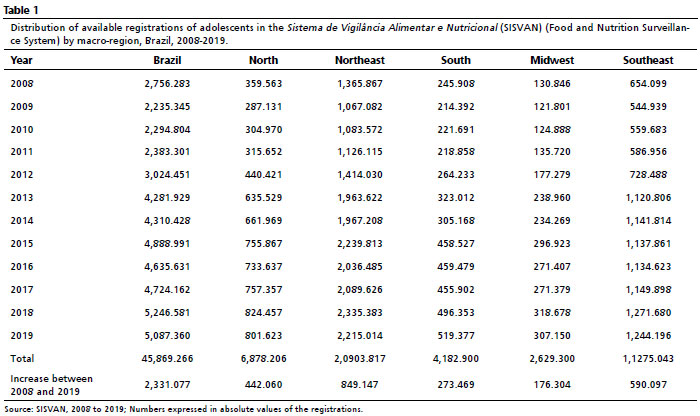






 Ler em português
Ler em português