ABSTRACT
OBJECTIVES: to determine the prevalence of pathological findings according to the type of chorionicity in pregnancies in two institutions in Bogotá, Colombia.
METHODS: descriptive, retrospective, cohort study. Biometric variables were calculated, and pathological findings were evaluated according to the type of chorionicity in multiple pregnancies. Statistical characterization was performed with absolute frequencies, calculation of relative frequencies in qualitative variables, standard deviation measures, median and interquartile range. In addition, a descriptive analysis of the information was carried out.
RESULTS: 528 studies were carried out in 141 pregnant women, 98.5% (n = 139) twins and 1.4% (n = 2) triplets. A prevalence of 35.4% of fetal complications was calculated. The most frequent was fetal growth restriction (p=0.37). According to each type of chorionicity, fetal growth restriction was presented in 50% (1/2) of the trichorionics, 16.6% (7/42) of the monochorionics, and 11.3% (11/97) of the dichorionics.
CONCLUSION: fetal growth restriction was the most common finding, both in trichorionics, monochorionics and dichorionics pregnancies.
Keywords:
Twin pregnancy, Multiple pregnancies, Twins, Biometry, Ultrasonography, Twin diseases
RESUMO
OBJETIVOS: el objetivo del estudio fue determinar la prevalencia de los hallazgos patológicos ecográficos en embarazos múltiples de acuerdo con la corionicidad en dos instituciones en Bogotá-Colombia.
MÉTODOS: estudio de cohorte, descriptivo, retrospectivo. Las variables biométricas realizadas y los hallazgos patológicos se evaluaron de acuerdo con el tipo de embarazo gemelar. Se realizó caracterización estadística con frecuencias absolutas, cálculo de frecuencias relativas en variables cualitativas, medidas de desviación estándar, mediana y rango intercuartílico. Además, se realizó análisis descriptivo de la información.
RESULTADOS: se realizaron 528 estudios en 141 gestantes, encontrando 98,5% (n=139) gemelares y 1,4% (n=2) triples. Se calculó una prevalencia de 35,4% de complicaciones fetales siendo más frecuente la restricción del crecimiento fetal (p=0,37). Según la corionicidad, esta complicación se presentó en 50% (1/2) de los tricoriónicos, 16,6% (7/42) de los monocoriónicos y 11,3% (11/97) de los dicoriónicos.
CONCLUSIÓN: la restricción del crecimiento fetal fue el hallazgo más común en los embarazos múltiples en la población estudiada.
Palavras-chave:
Embarazo gemelar, Embarazo múltiple, Gemelos, Biometría, Ultrasonografía, Enfermedades en gemelos
IntroductionTwin pregnancy is about 3% of live births and 97% of multiple births.
1,2 It is a high-risk condition for pregnant patients, given the comorbidities and complications inherent and exclusive to this type of pregnancy.
1,3Multiple pregnancies are classified according to the chorionicity (e.g. , monochorionic; dichorionic, trichorionic). Also, according to the amnionicity in monoamniotics, diamniotics, triamniotics. Or regarding zygosity (development from one or two zygotes) in monozygotic and dizygotic.
4,5Regarding morbidity and mortality in multiple pregnancies, 10% morbidity and twice the perinatal mortality have been described, being higher in pregnancies classified as monozygotic compared with dizygotic.
3,6,7 Admission to the neonatal intensive care unit due to prematurity is the most frequent condition in multiple pregnancies.
6 Other adverse outcomes are fetal growth restriction, congenital anomalies, aneuploidies, perinatal death, premature preterm rupture of ovular membranes, anemia, gestational diabetes, preeclampsia, postpartum hemorrhage, and thromboembolic events, among others.
8,9 Monochorionic twin pregnancies with single complications are rare. Including, twin-to-twin transfusion syndrome, the polycythemia anemia sequence, the twin reverse arterial perfusion sequence and the selective fetal growth restriction.
10,11 Therefore, the ultrasound identification of chorionicity and amnionicity, ideally performed in the first trimester, constitutes the cornerstone in the management of multiple gestations.
12,13In Colombia, research to determine biometrics and/or perinatal outcomes in twin pregnancies is scarce.
14,15 The lack of knowledge regarding this population of pregnant women could be an obstacle to determine the outcomes according to the sociodemographic, ultrasound, maternal perinatal morbidity, and mortality characteristics. Therefore, the main objective of the study was to determine the prevalence of pathological fetal ultrasound findings according to the type of chorionicity, also to describe the ultrasound characteristics of multiple pregnancies in two institutions in the city of Bogotá, Colombia.
MethodsDescriptive, retrospective, cohort study. The data were extracted in two institutions in the city of Bogotá, from the statistics of the ultrasound service of each center between January 2014 and December 2018. All pregnant women with multiple pregnancies were included without distinction of chorionicity or zygosity.
Ultrasonography in pregnant women was performed by six gynecologists trained in ultrasound and/or specialists in maternal-fetal medicine using the International Society of Ultrasonography recommendations.
16Demographic variables were included such as maternal age, fetal ultrasound observations such as chorionicity, gestational age, and fetal growth percentile, and biometric parameters such as crown rump length, biparietal diameter, head circumference, abdominal circumference, femoral length, and estimated fetal weight (EFW). Also, pathological findings in the ultrasound report were described, such as abortion, intrauterine fetal demise, congenital malformations, small for gestational age (if both twins have an EFW <10
th centile),
16 twin-to-twin transfusion syndrome (diagnosed by polyhydramnios/oligohydramnios sequence: amniotic fluid pocket >8-10 cm in the amniotic sac of the recipient fetus and amniotic fluid pocket
<2 cm in the amniotic sac of the donor fetus), anemia sequence polycythemia (maximum middle cerebral artery velocity >1.5 MoM in the donor fetus and maximum middle cerebral artery velocity <1 MoM in the recipient), twin reverse arterial perfusion sequence (in a monochorionic multiple gestation, a fetus with no cardiac activity or a rudimentary pump structure and Doppler demonstrating retrograde arterial flow to acardiac fetus), selective fetal growth restriction (a fetus with a monochorial gestation presents an estimated fetal weight <10
th percentile, associated with weight discordance ≥25%) and fetal weight discordance (estimated fetal weight difference ≥25% based on the weight of the older twin, greater weight-lesser weight x 100/major weight).
16The universe of the population was considered according to the inclusion criteria. The sampling was non-probabilistic. The information was collected by reviewing ultrasound records in an Excel database. The information was analyzed, performing a statistical description of absolute frequencies, calculation of relative frequencies for the qualitative variables, and measures of mean and standard deviation or median and interquartile range.
The prevalence of complications was obtained by the total complicated multiple pregnancies/total pregnant women with multiple pregnancies by the years of the ultrasound. The analysis was performed using SPSS software. A chi-square test was used.
This research was considered a risk-free study. Any type of intervention to the patient was performed. The study was bases on information based on secondary sources, which are the ultrasound reports of each patient. Ethical principles for human research from the Helsinki Declaration and the Colombian resolution 8430 of 1993 were considered in this study, and it was classified as an investigation with minimum risk.
17 The project was approved the ethics committee in both institutions. Ethical endorsement of the research was emitted by one of the institutions (ad hoc ethics committee of the other institution).
ResultsThe study included 528 ultrasound reports of 141 pregnant women, 139 twins and 2 triple pregnancies. The average number of ultrasound evaluations in each pregnancy was 2.6 (SD= 1.5) with a range from 1 to 6 ultrasound evaluations for each patient. The mean maternal age was 25.2 (SD= 6.0) (range 14 to 41). The average gestational age at which the ultrasound was performed was 25.0 weeks (SD= 7.1) (5.6 to 37.0 weeks).
In the first trimester 8.1% (n=43) ultrasound studies were performed; in the second and third trimesters of pregnancy 46.2% (n=244) and 45.6% (n=241) ultrasounds were performed, respectively.
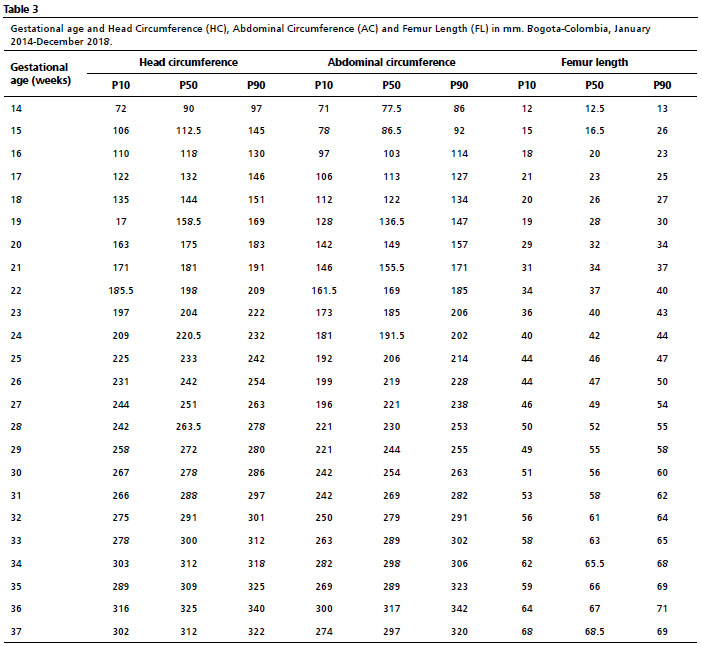
Pregnancies were classified according to their type of chorionicity and amnionicity, 68.7% (n=97) dichorionic diamniotic were found, monochorionic diamniotic in 27.6% (n=39) cases, and 2.1% (n=3) were monochorionic monoamniotic. The trichorials were 1.4% (n=2) (Table 1). Regarding the percentiles of the variables fetal biometrics and gestational age, the results are presented in Tables 2 to 4. Regarding the growth percentile according to estimated fetal weight, the average was 33.7% (SD=28.3) with a range of 0 to 97%.
The prevalence of fetal pathologies was 35.4%, fetal growth restriction in 13.4% (n=19) multiple pregnancies being the most frequent. At least one of the fetuses was affected by this condition. It was observed that 8.2% (n=8) and 7.1% (n=3) met the criteria for a small for gestational age in dichorionic and monochorionic gestations, respectively.
In the analysis of the complications and relating them to chorionicity, it was evidenced that in cases of dichorionic twin gestations, fetal growth restriction occurred in 11.3% (11/97) pregnancies and at least one of the fetuses, in monochorionic twins, 16.6% (7/42) met diagnostic criteria for selective fetal growth restriction. Regarding trichorionic pregnancies, 50% (1/2) of the pregnancies and at least one fetus presented fetal growth restriction (
p= 0.37).
Eight (4.1%) cases of bichorionic pregnancies ended in abortion, which occurred between week 7 and week 19, and 4 cases (9.5%) in monochorionic pregnancies (
p=0.33). In two of the twin pregnancies, abortion occurred in both fetuses, and the other cases had intrauterine death of a single fetus, there were no ultrasound studies after this finding.
There were 2 intrauterine deaths in one of the multiple pregnancy fetuses, one in a dichorionic pregnancy at week 23 and the other in a monochorionic pregnancy at week 33 of gestation (
p=0.15) (without new ultrasound reports after death). In four fetuses, ultrasound findings of congenital malformations were identified. A discordant malformation was evidenced in a monochorial pregnancy, since in one fetus there was a suspicion of right renal agenesis and in the other fetus of unilateral renal pyelctasia. In another dichorionic pregnancy, findings consistent with Cantrell's pentalogy were identified in one of the fetuses, another dichorionic pregnancy, and one of the fetuses presented findings consistent with alobar holoprosencephaly (
p=0.26).
Regarding the complications of monochorionic pregnancy, 11.9% (n=5) cases of twin-to-twin transfusion syndrome were found and 2.3% (n=1) met the criteria for weight discordance. There were no cases of polycythemia anemia sequence or twin reversed arterial perfusion sequence. Regarding chorionicity and the presentation of abnormal findings on ultrasound, no statistically significant differences were found, as evidenced in Table 5.
DiscussionMultiple pregnancies carry a high risk of adverse maternal and perinatal outcomes.
3,18-22 Ultrasound is an essential tool for determining the characteristics of two or more fetuses. Biometric variables can be considered conclusive factors for adverse perinatal outcomes, since they help determine the probability of complications in multiple pregnancies; for example, the risk of perinatal mortality in relation to the diagnosis of fetal growth restriction or weight discordance.
9,19In this context, fetal biometric variables as independent variables and collectively have prognostic value. In the meta-analysis by Leombroni
et al.
23 5826 women with twin pregnancies were evaluated for the ultrasonographic diagnostic precision of the discordance of fetal weights, concluding that this finding has a moderate, not optimal, diagnostic precision in these pregnancies, since the cut-off points were very diverse in the studies. Ideally, there should be specific cut-off points for each population to perform ultrasound measurements; made in an ideal setting, the measurement of fetal biometric parameters should be calculated for each population,
21,22 where the cut-off for diagnosing weight discordance was ≥25%, as reported in the literature.
18Furthermore, Araujo's
24 study in 2014, compared fetal biometric parameters in twins between 14 and 38 weeks of gestation, and these parameters were statistically different between monochorionic and dichorionic pregnancies. Our study calculated the same biometric parameters but, unlikely Araujo's
24 study, we determined the prevalence of pathological findings according to the type of chorionicity in twins. Liao
et al.
25 in 2016 evaluated 807 ultrasound reports of a total of 200 women with twin pregnancies, where the majority were dichorionic (82.4%). They also calculated ultrasound variables to determine fetal growth, like the analysis in our study, with 528 ultrasound reports of 141 multiple pregnancies where the majority were dichorionic pregnancies, and where the 5
th, 10
th, 50
th and 95
th percentiles of the biometric ultrasound variables were calculated as in Liao's study.
25Additionally, with respect to the studies carried out in Colombia, there is a descriptive one carried out at the Universidad del Valle where it is stated that performing an ultrasound diagnosis of twin pregnancy prior to week 32 of gestation significantly reduces perinatal mortality (OR= 3.58; CI95%= 1.61-7.92), due to timely prenatal care.
26 In the present study, the highest proportion of ultrasounds were performed in the second and third trimesters of pregnancy. However, the determination of chorionicity in all the reports was defined by early ultrasound characteristics, in the cases in which this evaluation was possible, taking into account that the determination of chorionicity is optimally established before the week 16, since after this week its sensitivity decreases.
1,4,13According to the classification of chorionicity and its association with adverse events, Cañas
et al.
26 reported that the general intrauterine mortality in pregnancies with dichorionic placentas was 11.25% and in monochorionic ones, 8.6%, unlike the present study, where a lower intrauterine mortality rate was evidenced when related to chorionicity (especially in dichorionic), since it was found that the percentage of intrauterine death was 1.0% of all dichorionic pregnancies and 2.3% of the total of monochorionic pregnancies. Furthermore, our finding is also much lower than that reported in other studies such as that of Glinianaia
et al.
20 where they found a fetal mortality of 31.8% studying exclusively monochorionic pregnancies. In 2015 Molina
et al.
14 438 pregnant women were evaluated in two highly complex institutions in Bogotá, different from those of the present study, where they showed a general fetal mortality of 7.7%, without classification according to chorionicity.
Concerning other Colombian studies, in 2017, Molina
et al.
27 analyzed the perinatal results in monochorionic twin pregnancies, with fetal growth restriction and twin-to-twin transfusion syndrome being the most frequent complications. In our study, monochorionic pregnancies also had the most frequent complications, those mentioned in the work by Molina
et al.
27A study of 382 multiple pregnancies, without differentiation according to chorionicity, found that weight discordance is the most frequent complication in this population.
26In another study, in 2001, the most prevalent was fetal growth restriction, followed by a fetus that was small for gestational age.
28 We found that the most frequent fetal complication is fetal growth restriction, in the group of monochorionic, dichorionic and trichorionic pregnancies.
26-28 Furthermore, we found that morbidity was higher in dichorionic than in monochorionic pregnancies, in contrast to the study by Victoria
et al.
29 where they found greater morbidity in monochorionic twins compared to dichorionic pregnancies.
The identification of ultrasound characteristics in multiple pregnancies, including the specific fetal growth profile of each population, is essential to recognize truly ill fetuses or those with a significant alteration in the growth curve, of fetuses in which these variations could be physiological.
19,22,24 On the other hand, the recognition of chorionicity is essential in the population of multiple pregnancies as a factor for the possible appearance of complications in both monochorionic and dichorionic.
22 Considering the limited sample size, difficulties in extrapolating the results and pathological fetuses of the studied population could be possible.
Given that multiple pregnancies present a high risk of adverse perinatal outcomes, the diagnosis of chorionicity, as well as other ultrasound characteristics, based on the fetal biometric parameters of each population, are essential to carry out a correct approach to diagnosis, follow-up, and management of multiple gestation, bearing in mind that it is the best way to anticipate the onset of complications and reduce perinatal morbidity and mortality rates. In the population studied, fetal growth restriction is the most common finding in multiple pregnancies in both trichorionic, monochorionic and dichorionic pregnancies.
AcknowledgmentsAuthors would like to thank the followed institutions Ecodiagnóstico El Bosque Unit Centre, South West Health Services Unit- Hospital Occidente de Kennedy and Universidad El Bosque for their contributions in this study.
References1. Blumeneld YJ, Momirova V, Rouse DJ, Caritis SN, Sciscione A, Peaceman AM,
et al. Accuracy of Sonographic Chorionicity Classification in Twin Gestations. J Ultrasound Med. 2014 Dec; 33 (12): 2187-92.
2. Gabriel R, Bonneau S, Burette J. Embarazos múltiples: estudio anatomoclínico y tratamiento. EMC - Ginecol Obstetr. 2018 Jun; 54 (2): 1-16.
3. Glinianaia SV, Obeysekera MA, Sturgiss S, Bell R. Stillbirth and neonatal mortality in monochorionic and dichorionic twins: a population-based study. Human Reprod. 2011 Sep; 26 (9): 2549-57.
4. Rencoret G. Embarazo gemelar. Rev Méd Clín Las Condes. 2014 Nov; 25 (6): 964-71.
5. Berceanu C. Morphological and ultrasound findings in multiple pregnancy placentation. Rom J Morphol Embryol. 2018; 59 (2): 435-53.
6. Emery S, Bahtiyar M, Moise K. The North American Fetal Therapy Network Consensus Statement: Management of Complicated Monochorionic Gestations. Obstetr Gynecol. 2015 Sep; 12 (3): 575-84.
7. Lu J, Cheng YK, Ting YH, Law KM, Leung TY. Pitfalls in assessing chorioamnionicity: novel observations and literature review. Am J Obstetr Gynecol. 2018 Sep; 219 (3): 242-54.
8. Vayssière C, Benoist G, Blondel B, Deruelle P, Favre R, Gallot D,
et al. Twin pregnancies: guidelines for clinical practice from the French College of Gynaecologists and Obstetricians (CNGOF). Eur J Obstetr Gynecol Reprod Biol. 2011; 156 (1): 12-7.
9. D'Antonio F, Odibo A, Berghella V, Khalil A, Hack K, Saccone G,
et al. Perinatal mortality, timing of delivery and prenatal management of monoamniotic twin pregnancy: systematic review and meta‐analysis. Ultrasound Obstetr Gynecol. 2019 Feb; 53 (2): 166-74.
10. Rodriguez-Castillo J, Delgado-Gutierrez J, Quintero-Mejia JC, Pena-Ramirez T, Garcia-Novillo S. Embarazo gemelar monocorionico monoamniotico. Presentacion de tres casos y revision de la literatura. Rev Colomb Obstetr Ginecol. 2013 Oct; 64 (4): 462-8.
11. Durán-Morales MA, Ariza-Parra EJ. Síndrome de transfusión feto fetal: una mirada global a la enfermedad. MedUNAB. 2016 Mar; 18 (3): 204-12.
12. Gil Guevara ED, Gil Mejía EG. Diagnóstico ecográfico de la corionicidad y amnionicidad en el embarazo múltiple. Rev Peru Ginecol Obstetr. 2015; 61 (3): 263-8.
13. Reddy UM, Abuhamad AZ, Levine D, Saade GR; Fetal Imaging Workshop Invited Participants. Fetal imaging: executive summary of a joint Eunice Kennedy Shriver National Institute of Child Health and Human Development, Society for Maternal-Fetal Medicine, American Institute of Ultrasound in Medicine, American College of Obstetricians and Gynecologists, American College of Radiology, Society for Pediatric Radiology, and Society of Radiologists in Ultrasound Fetal Imaging workshop. Obstetr Gynecol. 2014 May; 123 (5): 1070-82.
14. Molina Giraldo S, Araméndiz JM, Beltrán A SL, Rojas Arias JL, Acuña Osorio E, Solano Montero AF. Resultado perinatal de embarazos gemelares atendidos en dos instituciones de alta complejidad en Bogotá, Colombia. Rev Chil Obstetr Ginecol. 2015; 80 (1): 18-23.
15. Carlos Hernán B, Díaz Martínez LA, Contreras García GA, Beltrán Avendaño MA, Salazar Martínez HA, Gutiérrez Sánchez LÁ,
et al. Desenlaces materno-fetales de los embarazos atendidos en el Hospital Universitario de Santander, Bucaramanga (Colombia), 2007-2011: Estudio de cohorte. Rev Colomb Obstetr Ginecol. 2015 Mar; 66 (1): 37-45.
16. Khalil A, Rodgers M, Baschat A, Bhide A, Gratacos E, Hecher K,
et al. ISUOG Practice Guidelines: role of ultrasound in twin pregnancy. Ultrasound Obstetr Gynecol. 2016 Feb; 47 (2): 247-63.
17. World Medical Association (WMA). Declaration of Helsinki - Ethical principles for medical research involving human subjects. [
Internet]. [access in 2022 Oct 11]. Available at:
https://www.wma.net/polices-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects18. Busnelli A, Dallagiovanna C, Reschini M, Paffoni A, Fedele L, Somigliana E. Risk factors for monozygotic twinning after in vitro fertilization: a systematic review and meta-analysis. Fertil Steril. 2019 Feb; 111 (2): 302-17.
19. D'Antonio F, Odibo AO, Prefumo F, Khalil A, Buca D, Flacco ME,
et al. Weight discordance and perinatal mortality in twin pregnancy: systematic review and meta‐analysis. Ultrasound Obstetr Gynecol. 2018 Jul; 52 (1): 11-23.
20. Glinianaia S, Rankin J, Khalil A, Binder J. Prevalence, antenatal management and perinatal outcome of monochorionic monoamniotic twin pregnancy: a collaborative multicenter study in England, 2000-2013. Ultrasound Obstetr Gynecol. 2019 Feb; 53:184-92.
21. Khalil A, D'Antonio F, Dias T, Cooper D, Thilaganathan B, Hamid R,
et al. Ultrasound estimation of birth weight in twin pregnancy: comparison of biometry algorithms in the STORK multiple pregnancy cohort. Ultrasound Obstetr Gynecol. 2014 Aug; 44(2): 210-20.
22. Khalil AA, Khan N, Bowe S, Familiari A, Papageorghiou A, Bhide A,
et al. Discordance in fetal biometry and Doppler are independent predictors of the risk of perinatal loss in twin pregnancies. Am J Obstetr Gynecol. 2015; 213 (2): 222.e1-222.e10.
23. Leombroni M, Liberati M, Fanfani F, Pagani G, Familiari A, Buca D,
et al. Diagnostic accuracy of ultrasound in predicting birth‐weight discordance in twin pregnancy: systematic review and meta‐analysis. Ultrasound Obstet Gynecol. 2017 Oct; 50 (4): 442-50.
24. Araujo Júnior E, Ruano R, Javadian P, Martins WP, Elito Jr J, Pires CR,
et al. Reference charts for fetal biometric parameters in twin pregnancies according to chorionicity. Prenat Diagn. 2014 Apr; 34 (4): 382-8.
25. Liao AW, Brizot ML, Kang HJ, Assunção RA, Zugaib M. Longitudinal reference ranges for fetal ultrasound biometry in twin pregnancies. Clinics. 2012; 67 (5): 451-5.
26. Cañas Giraldo CA, Cifuentes BR, Montes H. Morbimortalidad del embarazo gemelar en el Hospital Universitario del Valle. Rev Colomb Obstetr Ginecol. 1999; 50 (3): 179-85.
27. Molina Giraldo, Solano Montero A, Santana Corredor N, Ortega, Alfonso Ayala D. Resultados périnatales en embarazos múltiples monocoriales relacionados con las características placentarias. Ginecol Obstetr Méx. 2017 Feb; 85 (2): 80-91.
28. Vallejo DL, Rangel YA, Fonseca AA, Cardona EP. Estado actual del embarazo gemelar: Revisión de la literatura. Rev Universidad Industrial de Santander. Salud 2012 Dec; 44 (3): 41-8.
29. Victoria A, Mora G, Arias F. Perinatal outcome, placental pathology, and severity of discordance in monochorionic and dichorionic twins. Obstet Gynecol. 2001; 97 (2): 310-5.
Received on February 16, 2023
Final version presented on April 29, 2023
Approved on May 16, 2023
Associated Editor: Alex Sandro Rolland
Author's contribution: All the authors contributed to the conception and structure of the article, the analysis and interpretation of data and critical revision, like:
Guzmán Yara YN: Protocol/project development, data management, data analysis, manuscript writing/editing; Montserrat UC: Protocol/project development, data collection and management, data analysis, manuscript writing/ editing; Beltrán SL: Protocol/project development, data collection; Bandera L: Protocol/project development; De la Hoz Valle J: Protocol/project development, data management, data analysis, manuscript writing/editing; Romero XC: Protocol/project development, data collection and management, data analysis, manuscript writing/ editing.
The authors approved the final version of the article and declare no conflict of interests.


 ; Montserrat Uriel Calvo2
; Montserrat Uriel Calvo2









 Ler em português
Ler em português