ABSTRACT
OBJECTIVES: to evaluate associated factors with sexual dysfunction among middle-aged women.
METHODS: cross-sectional and analytical study was carried out with climacteric women attended at a Family Health Strategy Unit in the city of Montes Claros, MG. Brazil. The eligible women answered a question form containing sociodemographic, behavioral, anthropometric, gynecological factors and sexuality. The Body Mass Index and waist circumference were used to assess nutritional status and metabolic risk. To evaluate quality of life and sexual performance the Menopause Rating Scale and the Sexual Quotient - Female Version were used, respectively. Bivariate analysis and hierarchical multiple regression were used to identify associated factors with sexual dysfunction in the climacteric period.
RESULTS: among 195 women, 29.6% had sexual dysfunction. The prevalence of unsatisfactory sexual performance was higher among women who reported moderate to severe climacteric symptoms (OR=2.47) and lower schooling level was also associated (OR=1.95). However, age at menarche below 12 years (OR=0.43) and non-white (OR=0.36) seem to have a protective effect for good sexual performance.
CONCLUSION: the prevalence of sexual dysfunction was high and the level of schooling and climacteric symptomatology were associated factors with this outcome.
Keywords:
Climacteric, Physiological sexual dysfunction, Psychogenetic sexual dysfunctions, Woman's health, Sexuality
RESUMO
OBJETIVOS: avaliar os fatores associados à disfunção sexual entre as mulheres de meia-idade.
MÉTODOS: estudo de corte transversal e analítico realizado com mulheres climatéricas atendidas em uma Unidade de Estratégia de Saúde da Família no município de Montes Claros-MG, Brasil. As mulheres elegíveis responderam a um formulário contendo questões sociodemográficas, comportamentais, antropométricas, fatores ginecológicos e sexualidade. Utilizou-se o Índice e Massa Corporal e a circunferência da cintura para avaliar o estado nutricional e risco metabólico. Para avaliar a qualidade de vida e o desempenho sexual foram utilizados a Menopause Rating Scale e o Quociente Sexual -Versão Feminina, respectivamente. Empregou-se análise bivariada e regressão múltipla hierarquizada para identificar fatores associados à disfunção sexual no climatério.
RESULTADOS: dentre 195 mulheres, 29,6% apresentaram disfunção sexual. A prevalência de desempenho sexual insatisfatório foi maior entre as mulheres que declararam sintomas climatéricos moderados a graves (OR = 2,47) e o menor grau de escolaridade (OR = 1,95). No entanto, a idade da menarca abaixo de 12 anos (OR = 0,43) e a cor de pele não branca (OR = 0,36) parecem ter efeito protetor para o bom desempenho sexual.
CONCLUSÃO: a prevalência de disfunção sexual foi elevada e o nível de escolaridade e a sintomatologia climatérica foram fatores associados a esse resultado.
Palavras-chave:
Climatério, Disfunções sexuais fisiológicas, Disfunções sexuais psicogênicas, Saúde da mulher, Sexualidade
IntroductionThe climacteric phase in the female population occurs between the ages of 40 and 65 and is a phase of life that characterizes the transition between the reproductive and non-reproductive periods with a consequent reduction in steroid hormones.
1,2 This reduction associated with other factors such as emotional and socio-cultural factors, makes women more susceptible to sexual dysfunction,
3-5 influencing their quality of life.
6Female sexual dysfunction has a multifactorial origin, involving any disorder that includes variation in the intensity and quality of desire, arousal and orgasm,
7 and may be associated with endocrine changes in the middle age.
8In Brazil, the prevalence of sexual dysfunction reaches an average of 60% of the women between the ages of 40 and 65.
9,10 The dimensions most affected have been sexual desire, vaginal lubrication and sexual satisfaction, and the main reason for their dissatisfaction is related to bodily changes, which favors low self-esteem and decreased sexual desire, the latter being the most observed.
11Sexual function is part of a healthy aging with quality of life.
12 Therefore, it is considered an important aspect of women's well-being, regardless of age.
13,14 In view of this, it is essential to know the factors that can interfere with sexual life during the climacteric period.
15 There is no consensus in the literature on factors that influence the sexuality in middle-aged women.
8The aim of this study was to assess the factors associated with sexual dysfunction among middle-aged women.
MethodsThis is a cross-sectional, analytical study carried out with climacteric women who took part in a health education event on breast cancer between August and October 2013 at a Family Health Strategy Unit (ESF) in the city of Montes Claros, MG. Brazil.
The aforementioned sample was selected due to its greater accessibility, as there was no specific space and/ or location in the city to care for climacteric women. This study included women aged between 40 and 60 years old, considered to be middle-aged by the World Health Organization (WHO),
1 apparently healthy, with good physical conditions for measuring anthropometric data and without sexual abstinence in the last six months. Exclusion criteria were pregnant women, women unable to answer the questionnaire, women with psychiatric disorders and any factor that made the interview impossible (e.g. lack of time, pathologies, illiteracy and explicit refusal).
The authors trained all the interviewers beforehand and supervised all the data collected. Eligible women who were waiting to be attended were individually invited to take part in the study.
These women answered the form developed specifically for this research, in which the independent variables were allocated into four blocks: (1) sociodemographic, (2) behavioral, (3) anthropometric and (4) gynecological.
The sociodemographic variables included age, self-reported skin color, occupation, home ownership and schooling.
The behavioral variable block took into account smoking (non-smokers and smokers/ex-smokers), alcohol consumption (consumers and non-consumers) and whether the women were satisfied with their bodies (yes or no).
The anthropometric variables were Body Mass Index (BMI) and Waist Circumference (WC). To calculate BMI, height and weight were measured.
16 To assess body weight, the women were weighed wearing light clothing and no shoes, in an orthostatic position, with their feet together and arms relaxed along their body, on a Geratherm
® Body Fat Scale (Brazil) portable electronic scale, with a capacity for 150 Kg, minimum and precision of 50 g. Height was measured using a Carci
® (Brazil) inelastic tape measure, with a scale of 0 to 150 cm, on a flat wall without a baseboard. During the measurement, the women were instructed to stand up straight, keep their feet together and look to the horizon, without bending or extending their heads. Weight and height measurements were taken in duplicate and the average obtained to calculate BMI. Overweight was considered when BMI ≥ 25kg/ m
2, according to the cut-off point recommended by the
Associação Brasileira para o Estudo da Obesidade e da Síndrome Metabólica (ABESO)
17 (Brazilian Association for the Study of Obesity and Metabolic Syndrome).
Waist circumference (WC) was obtained using an inelastic anthropometric tape scaled by 0.1cm. The measurement was taken with the individual standing with the abdomen relaxed, arms outstretched and on the side of the body. The tape measure was placed on the smallest circumference of the abdomen or on the curvature located between the ribs and the hip bone (iliac crest), without compressing the tissues. Three measurements were taken, followed by an arithmetic mean. Those with WC ≥80 cm and very high WC ≥88 cm were considered to be at metabolic risk.
18The gynecological variables included: 1) climacteric symptoms (asymptomatic-mild and moderate-severe). This assessment used the Menopause Rating Scale (MRS), an instrument validated for Brazilian Portuguese language, consisting of 11 questions that addressed the symptoms segmented into somato-vegetative, psychological and urogenital domains. Each woman analyzed and gave her opinion on each symptom and could classify it as absent, mild, moderate, severe or very severe.
19 2) climacteric phases: pre-menopause (if menstrual cycles were naturally maintained), post-menopause (if there was spontaneous amenorrhea for a period of 12 consecutive months or more) and did not have menopause yet, if there was menstruation in the last 12 months, even if irregular. 3) type of menopause (spontaneous, hysterectomized and did not have it yet). 4) age at menopause (<50 or ≥50 years). 5) age at menarche (≥12 or <12 years).
The second instrument was the Sexual Quotient, female version (SQ-F) used to assess sexual function. This instrument assesses the various domains of women's sexual activity and was developed and validated specifically for the Brazilian female population. It consists of 10 questions that assess each phase of the sexual response cycle: questions 1, 2 and 8 on sexual desire and interest; question 3, foreplay; questions 4 and 5, personal arousal and attuned with the partner; questions 6 and 7, comfort; questions 9 and 10, orgasm and satisfaction.
20Each question must be answered on a scale of zero to five, with zero indicating "never" and five "always". The score is obtained by adding the points from all the questions multiplied by two, resulting in a score ranging from zero to 100. Overall sexual performance/satisfaction is calculated by multiplying the sum of the values of the 10 questions by two, and is interpreted as follows: 82100 points, good to excellent; 62-80 points, fair to good; 42-60 points, unfavorable to fair; 22-40 points, poor to unfavorable and 0-20 points, null to poor. The higher the scores for questions on the QS-F (with the exception of question 7, which refers to the presence of pain), the best indication of the woman's sexual performance/ satisfaction.
20A score of less than or equal to 60 is established as the cut-off point for diagnosing the presence of female sexual dysfunction.
20Initially, descriptive analyses were carried out on all the variables investigated by means of their frequency distributions.Bivariate analyses were then carried out between the outcome variable (sexual function) and each independent variable (sociodemographic, behavioral, anthropometric and gynecological) using the logistic regression model, estimating the odds ratio (OR) and its 95% confidence interval. Variables with a descriptive level (p-value) of less than 0.25 were selected for multiple analysis. The logistic regression model was used in the multiple analysis. The Odds Ratio (OR) with a 95% confidence interval (CI95%) was used to analyze the strength of the association. The statistical program PASWR 17.0 was used to carry out the analyses.
The research project for this study was approved by the Research Ethics Committee of the
Universidade Estadual de Montes Claros (UNIMONTES) under opinion number 311.572 (CAAE: 17846513.0.0000.5146).
ResultsThe sample consisted of 253 women with a mean age of 50.2 years (SD ± 5.8 years). Of these women, 195 reported being sexually active and 58 had not had sexual intercourse in the last six months, resulting in a total of 195 women eligible to answer the QSF.
The sample was dichotomized into two subgroups in terms of the standard of sexual function, based on the QS-F scores, with 47.4% having a good standard sexual function and 29.6% having sexual dysfunction. The other characteristics of the group are shown in Table 1.
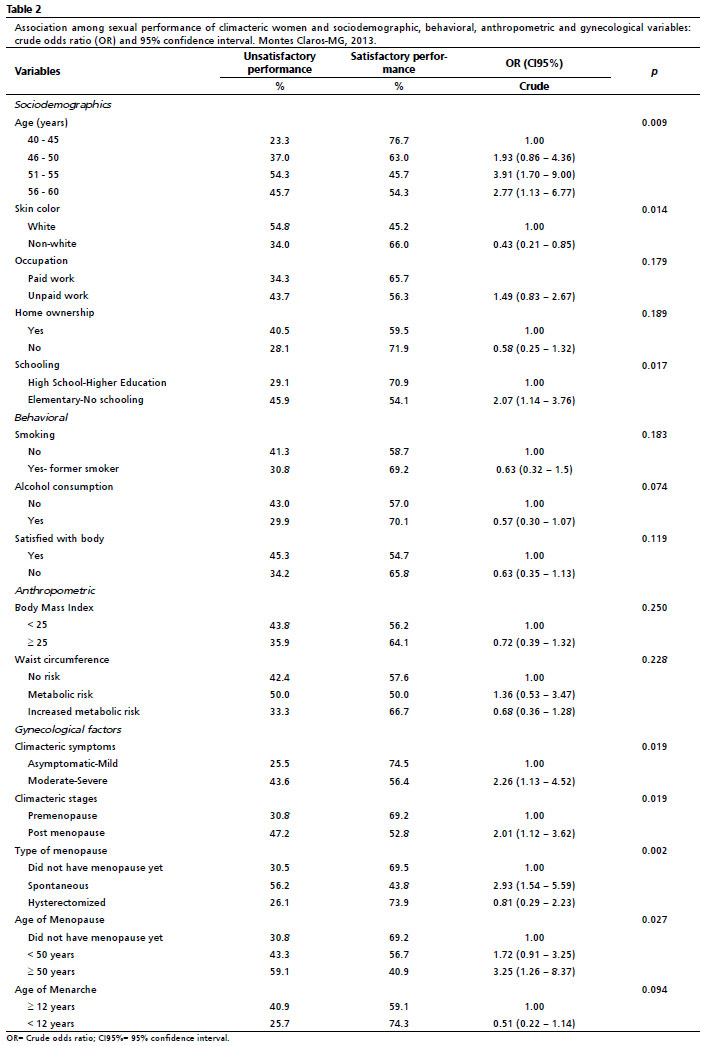
Table 2 shows the results of the bivariate analyses. All the variables were found to be associated at the 0.25% level with the sexual performance outcome: age (
p=0.009) skin color (
p=0.014), occupation (
p=0.179), home ownership (
p=0.189), schooling (
p=0.017), smoking (
p=0.183), alcohol consumption (
p =0.074), satisfied with body (
p=0, 119), BMI (
p=0.25), WC (
p=0.228), climacteric symptoms (
p=0.019), climacteric stages (
p=0.019), type of menopause (
p=0.002), age of menopause (
p=0.027), age of menarche (
p=0.094). These variables were selected for the final multiple analysis.
The variable "climacteric symptoms" was a factor associated with "sexual performance". The prevalence of unsatisfactory sexual performance was higher among women who reported moderate to severe symptoms (OR=2.47), when compared to those who presented mild symptoms or no symptoms at all (Table 3).
It was found that women who had a low level of schooling (elementary school / no schooling) had a higher prevalence of sexual dissatisfaction when compared to those who reported having high school and higher education (OR=1.95) (Table 3).
On the other hand, the variable on age of menarche below 12 years and non-white seemed to have a protective effect on good sexual performance, respectively (OR=0.43; CI95%=0.18-1.02), (OR=0.36; CI95%=0.170.76) (Table 3).
DiscussionThis study showed that just over a quarter of the women had sexual dysfunction, which was more evident in those who self-reported moderate to severe climacteric symptoms. The outcome in sexual performance was associated with age, severity of climacteric manifestations, low level of schooling and skin color.
In this study, sexual dysfunction had a frequency of 29.6%, a value lower than those found in studies carried out in Brazil and in other countries. In Brazil, in the states of Pernambuco and Sergipe, studies revealed that 44.4% and 42.9% of the women were at risk of sexual dysfunction, respectively.
21,22 In a study carried out in an outpatient clinic at a public hospital in the Northeast of Brazil, women aged between 40 and 65, more than half of them had sexual dysfunction (58.7%).
23 In other studies which evaluated middle-aged Iranian women, the risk of sexual dysfunction reached 46% and 68%, respectively.
24,25 Other studies of middle-aged women have also found a high frequency of sexual dysfunction.
10,26,27 These variations can be attributed to factors such as the type of questionnaire used, sample size, study design and sociodemographic characteristics.
In this present study, age had an influence on sexual performance, especially in the 51 to 55 age group, with a higher percentage of unsatisfactory performance. Findings in a study of 162 post-menopausal Iranian women showed that age, combined with anxiety, interfered with sexual function.
24 At this stage of life, there are various factors that interfere with sexual function and sexuality, such as the hormonal and physiological changes that are characteristics at this stage.
8,28The MRS domains were higher in the group of women at risk of sexual dysfunction, when compared to those who were not, thus suggesting a greater intensity of symptoms in the group at risk of sexual dysfunction, as shown by Cabral
et al.
9The reduction in estrogen levels in the female body interferes with sexual response, as this hormone plays a crucial role in sexual desire, thus increases the risk of sexual dysfunction.
10,26,29 Several studies have also corroborated these results, showing that the arrival of menopause can have a negative impact on sexual function, especially when associated with the common symptoms of this stage at a woman's life.
9,10In this research, an investigation was carried out with women living in the state of Bahia and associated low schooling with sexual dysfunction which this factor was also associated as a high risk of sexual dysfunction.
30 Individuals with greater social vulnerability (which is often related to a lower level of schooling) and, consequently, financial vulnerability, can have repercussions on their sexuality.
30As for skin color, women who called themselves white had a higher risk of sexual dysfunction than others. A study of climacteric women living in Teresina, in the state of Piauí, Brazil, revealed that most of the women were not white and that 64% of the sample was at risk of sexual dysfunction.
10Among the population studied, the prevalence of sexual dysfunction was high and an analysis of possible factors were associated with its occurrence revealing the influence of schooling, as well as climacteric symptoms. It is noteworthy that in Brazil, there are not many studies evaluating the pattern of sexual function in climacteric women and its association with other factors.
21,30This study was carried out with a non-probabilistic sample, which represents a limitation to the external validity of the results. However, it is important for the population in question, these women need to improve their quality of life, since the presence of sexual activity in the ageing process preserves good relationships with their partners, reducing feelings of loneliness.
Further studies should be planned and carried out in order to find out about the various factors that may be associated with sexual dysfunction in climacteric women, enabling a better multidisciplinary approach in order to provide a better quality of life.
References1. World Health Organization (WHO). Investigaciones sobre la menopausia en los años noventa: informe de un Grupo Cientifico de la OMS. Geneva: WHO; 1996. [acesso em 2022 Jun 20]. Disponível em:
https://apps.who.int/iris/handle/10665/419842. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Manual de atenção à mulher no climatério/menopausa. Brasília (DF): Ministério da Saúde; 2008. [acesso em 2022 Mai 13]. Disponível em:
http://bvsms.saude.gov.br/bvs/publicacoes/manual_atencao_mulher_climaterio.pdf3. Johnson A, Roberts L, Elkins G. Complementary and Alternative Medicine for Menopause. J Evid Based Integr Med. 2019; 24: 2515690X19829380.
4. Scavello I, Maseroli E, Di Stasi V, Vignozzi L. Sexual Health in Menopause. Medicina (Kaunas). 2019; 55 (9): 559.
5. Gracia CR, Freeman EW. Onset of the Menopause Transition: The Earliest Signs and Symptoms. Obstet Gynecol Clin North Am. 2018; 45 (4): 585-97.
6. Clayton AH, Valladares Juarez EM. Female Sexual Dysfunction. Med Clin North Am. 2019; 103 (4): 681-98.
7. Female Sexual Dysfunction: ACOG Practice Bulletin Summary, NUMBER 213. Obstet Gynecol. 2019 Jul; 134 (1): 203-5.
8. Nappi RE, Cucinella L, Martella S, Rossi M, Tiranini L, Martini E. Female sexual dysfunction (FSD): Prevalence and impact on quality of life (QoL). Maturitas. 2016; 94: 87-91.
9. Cabral PU, Canário AC, Spyrides MH, Uchôa SA, Eleutério J Jr, Gonçalves AK. Determinants of sexual dysfunction among middle-aged women. Int J Gynaecol Obstet. 2013; 120 (3): 271-4.
10. Trento SRSS, Madeiro A, Rufino AC. Sexual Function and Associated Factors in Postmenopausal Women. Rev Bras Ginecol Obstet. 2021; 43 (7): 522-9.
11. Afshari P, Houshyar Z, Javadifar N, Pourmotahari F, Jorfi M. The Relationship Between Body Image and Sexual Function in Middle-Aged Women. Electron Physician. 2016; 8 (11): 3302-8.
12. Souza Jr EV, Silva Filho BF, Barros VS, Souza AR, Cordeiro JRJ, Siqueira LR,
et al. Sexuality is associated with the quality of life of the elderly!. Rev Bras Enferm. 2021 Jul; 74 (Suppl. 2): e20201272.
13. Thomas HN, Neal-Perry GS, Hess R. Female Sexual Function at Midlife and Beyond. Obstet Gynecol Clin North Am. 2018; 45 (4): 709-22.
14. Silva FG, Pelzer MT, Neutzling BRS. Attitudes of Elderly Women Regarding the Expression of Their Sexuality. Aquichan 2019; 19 (3): e1934.
15. Santos S, Lima CM, Vicente JTS, Silvestre GCSB, Neves HG, Figueiredo SEFMR. Climacteric Period and Its Implications in Sexuality. Rev Enferm Atual. 2018; 86: 1-10.
16. World Health Organization (WHO). Obesity: preventing and managing the global epidemic: report of a WHO consultation. Geneva: WHO; 2000. [acesso em 2013 Jun 20]. Disponível em:
https://apps.who.int/iris/handle/10665/4233017. Associação Brasileira para o Estudo da Obesidade e da Síndrome Metabólica (ABESO). Diretrizes Brasileiras de Obesidade (2015/2016). São Paulo (SP): ABESO; 2016. [acesso em 2022 Mar 22]. Disponível em:
https://abeso.org.br/wp-content/uploads/2019/12/Diretrizes-Download-Diretrizes-Brasileiras-de-Obesidade-2016.pdf18. Callaway CW, Chumlea WC, Bouchard C, Himes JH, Lohman TG, Martin AD,
et al. Circumferences. In: Lohman TG, Roche AF, Martorell R, editors. Anthropometric standardization reference manual. Champaign: Human Kinetics Books; 1988. p. 39-54.
19. Heinemann K, Ruebig A, Potthoff P, Schneider HP, Strelow F, Heinemann LA,
et al. The Menopause Rating Scale (MRS) scale: a methodological review. Health Qual Life Outcomes. 2004 Sep; 2: 45.
20. Abdo CHN. Quociente Sexual Feminino: um Questionário Brasileiro para Avaliar a Atividade Sexual da Mulher. Diagn Tratamento. 2009; 14 (2): 89-1.
21. Fonseca GMS; Lima JCRC, Silva KM, Barbosa SSA, Oliveira BDR. Prevalência das disfunções sexuais no período do climatério em uma clínica especializada na saúde da mulher em Caruaru/PE. Fisioter Bras. 2021; 22 (1): 72-85.
22. Aquino KSJ, Prado DS, Santos BR, Barreto IDC. Fatores Associados a Disfunções Sexuais no Climatério. Rev Bras Sex Hum. 2019; 29 (2): 36-46.
23. Cruz EF, Nina VJ, Figuerêdo ED. Climacteric Symptoms and Sexual Dysfunction: Association between the Blatt-Kupperman Index and the Female Sexual Function Index. Rev Bras Ginecol Obstet. 2017; 39 (2): 66-71.
24. Tavoli A, Tavoli Z, Effatpanah M, Montazeri A. Prevalence and Associated Risk Factors for Sexual Dysfunction Among Postmenopausal Women: a Study from Iran. Womens Midlife Health. 2021; 7 (1): 10.
25. Rahnavardi M, Khalesi ZB, Rezaie-Chamani S. Effects of Lifestyle on Sexual Function Among Postmenopausal Women. Afr Saúde Sci. 2021; 21 (4): 1823-9.
26. Dabrowska-Galas M, Dabrowska J, Michalski B. Sexual Dysfunction in Menopausal Women. Sex Med. 2019; 7 (4): 472-9.
27. Worsley R, Bell RJ, Gartoulla P, Davis SR. Prevalence and Predictors of Low Sexual Desire, Sexually Related Personal Distress, and Hypoactive Sexual Desire Dysfunction in a Community-Based Sample of Midlife Women. J Sex Med. 2017; 14 (5): 675-86.
28. Barreiros BR, Oliveira NR, Vaz MMT. Função sexual em mulheres no climatério: estudo transversal. Rev Pesqui Fisioter. 2020; 10 (1): 50-7.
29. Crema IL, De Tilio R, Campos MT. Repercussões da menopausa para a sexualidade de idosas: revisão integrativa da literatura. Psicologia (Cons Fed Psicol). 2017; 37 (3): 753-69.
30. Barreto APP, Nogueira A, Teixeira B, Brasil C, Lemos A, Lôrdelo P. O impacto da disfunção sexual na qualidade de vida feminina: um estudo observacional. Rev Pesq Fisio. 2018; 8 (4): 511-7.
Received on March 13, 2023
Final version presented on July 23, 2023
Approved on August 7, 2023
Associated Editor: Melânia Amorim
Acknowledgements: We would like to thank the Interinstitutional Master's Program along with the
Universidade Estadual de Montes Claros (Unimontes) and
Faculdades Integradas Pitágoras de Montes Claros (FIPMoc) for their technical support.
Authors’ contribution: Gonçalves JTT and Silveira MF conceived the study, carried out the experimental design, analyzed the data and interpreted the results. Gonçalves JTT and Gonçalves CT carried out the data collection. Gonçalves JTT and Vieira KH drafted the manuscript and critically reviewed it for important intellectual content. Reis VMCP statistically analyzed the data and interpreted the results. Santana RF critically revised it for intellectual content. All the authors approved the final version of the article and declared no conflicts of interest.


 ; Camila Teles Gonçalves2
; Camila Teles Gonçalves2







 Ler em português
Ler em português