ABSTRACT
OBJECTIVES: to characterize the nutritional status of indigenous children underfive years of age living in rural communities in the Upper Solimões River region, inhabited by seven ethnic groups, based on data of december 2013.
METHODS: weight and height data extracted from SISVAN-I (Indigenous Food and Nutritional Surveillance System) forms filled in 2013 for 7,520 children (86.0% of the estimated children in this age group). The indices height-for-age (H/A), weight-for-age (W/A), weight-for-height(W/H), and body mass index-for-age (BMI/A) were calculated. Growth reference curves proposed by the World Health Organization were used to calculate z-scores.
RESULTS: the height-for-age (H/A) index presented the lowest mean z-score values, reaching −1.95 among children between 36 and 60 months. Mean z-score values for the weight-for-age (W/A) index also remained below zero. Mean z-score values for the indices weight-for-height (W/H) and body mass index-for-age (BMI/A) remained slightly above zero, reaching a maximum value of 0.5. Of all children, 45.7% presented low H/A, 9.6% presented low W/A, 4.5% presented low W/H, and 10.7% presented overweight based on BMI/A.
CONCLUSION: our analysis show that in 2013 poor nutritional status persisted as an important health issue among these rural indigenous children.
Keywords:
Nutritional assessment, Indigenous health, Chronic undernutrition, Amazonia
RESUMO
OBJETIVOS: caracterizar o estado nutricional de crianças indígenas menores de cinco anos, de comunidades rurais na região do Alto Solimões, habitada por sete etnias, com base em dados de dezembro de 2013.
MÉTODOS: foram extraídos dos formulários do SISVAN Indígena dados de peso e estatura, coletados em 2013, de 7.520 crianças (86,0% das crianças estimadas nesta faixa etária). Foram calculados os índices estatura-para-idade (E/I), peso-para-idade (P/I), peso-para-estatura (P/E) e índice de massa corporal para idade (IMC/I). Curvas de referência para crescimento propostas pela Organização Mundial da Saúde foram utilizadas para calcular escores z.
RESULTADOS: o índice estatura-para-idade (E/I) apresentou os menores valores médios de escore z, chegando a −1,95 nas crianças entre 36 e 60 meses. Os valores médios do escore z do índice peso-para-idade (P/I) também permaneceram abaixo de zero. Os valores médios do escore z para os índices P/E e índice de massa corporal para idade (IMC/I) mantiveram-se ligeiramente acima de zero, atingindo valor máximo de 0,5. Do total de crianças, 45,7% apresentaram baixa E/I, 9,6%, baixo P/I, 4,5% baixo P/E e 10,7% de excesso de peso de acordo com o IMC/I.
CONCLUSÃO: em 2013 a desnutrição persistia como um importante agravo à saúde nessas crianças.
Palavras-chave:
Avaliação nutricional, Saúde indígena, Desnutrição crônica, Amazônia
IntroductionNational health studies in Brazil have shown improvements in child health and nutrition indicators, with significant reduction of mortality and undernutrition levels.
1,2 Despite these advances, the principal health tendencies in the indigenous population in the country, especially in Amazonia, remained little knownuntil they were first assessed at the national scale and communicated academically and publicly beginning in the 2010s.
3Given the limited information about Amazonian child health and nutrition available from nationally representative studies, information produced at the local level remains essential. According to the First National Survey of Indigenous People's Health and Nutrition in Brazil (henceforth, the National Survey), conducted in 2008-2009, approximately 25% of indigenous children under five years presented chronic linear growth deficit.
4 This study also showed that in the North region of Brazil (where the state of Amazonas is located) this profile was even more accentuated, with 40.8% of children in this age group presenting chronic undernutrition.
Childhood undernutrition is a serious global problem affecting millions of children worldwide. It is mainly attributed to resource scarcity and impaired nutrient absorption, leading to severely detrimental consequences for children's development. In addition to stunting and low weight, undernutrition can also result in anemia, diarrhea, and impairments in cognitive and physical development. These effects ultimately affect children's school performance, general well-being, and quality of life.
5Recent nutritional assessments of diverse communities in the Amazon region
6,7 converge in finding chronic undernutrition the most severe nutritional disturbance in children under five years of age, often surpassing 50% of children evaluated.
6-9 Especially in the state of Amazonas, the few surveys undertaken in rural areas also point to chronic undernutrition as one of the principal health problems of childhood. According to Alencar
et al. ,
10,11 23.0% of children under five living along the principal waterways in the state presented linear growth deficit, reaching 35% of children along the Rio Negro.
However scarce, these studies reiterate the contemporaneity of the diagnostic made by Josué de Castro in
Geografia da Fome in the 1940s,
12 when he coined the term "endemic hunger" in reference to "…the presence of protein, vitamin, and mineral salt deficiencies" in residents of the North region of Brazil.
13 However, in this North region, it remains unclear which regional indigenous populations are most affected by such health inequities as high prevalence of child undernutrition even though health policies and services for indigenous people in Brazil have expanded and improved since the late 1990s, such as, outsourcing of health actions, planning of actions at the district level with the approval of the District Council, allocation of resources, supply of services, structuring of the network, improvement of logistics allowing greater reach of the target population, and training of human resources.
14,15In view of the importance of undernutrition in the nutritional profile of indigenous children in Brazil,
16 in 2006 the SISVAN-I (Indigenous Food and Nutritional Surveillance System) was implemented within the Indigenous Healthcare Subsystem. It is considered an important tool for monitoring the evolution of undernutrition in children and thereby guiding public policy.
17 Data produced by the SISVAN-I also provide an unusual opportunity to calculate and compare diagnostic nutritional indicators in a statistically underrepresented region.
This data source presents an unique advantage by incorporating robust data from the entire indigenous child population (the demographic universe) through frequent active monitoring by professionals supported by infraestrutre developed to overcome enormous logistical challenges inherent to accesing communities in Amazonia, such as limited air and terrestrial transportation services, long distances between urban centers and communities, expensive and unpredictible river transportation, and dynamic environmental obstacles and barriers.
The Upper Solimões River and its tributaries, in the "triple frontier" region where the borders of Brazil, Colombia, and Peru meet, are characterized demographically by a pronounced indigenous population within which the Tikuna ethnic group is most numerous (46,000 in 2010).
18 Others include Kokama, Kaixana, Kanamari, Kambeba, Maku-Yuhup, and Witoto. Like many other frontier regions in Amazonia, the Upper Solimões is a polyethnic and multicultural area with intense migratory movement and diversified commercial activities.
19 In this setting, lifestyles, habitation, sanitation, food security, and transmission dynamics of infectious and parasitic diseases disproportionally affect more vulnerable populations including indigenous peoples.
20To better understand the health inequities affecting an especially populous and ethnically diverse indigenous populationin the Upper Solimões River region, state of Amazonas, Brazil, the present study sought to characterize the nutritional profile of rural indigenous children under five years of age in December 2013 based on data from the SISVAN-I.
MethodsA cross-sectional study was conducted based on data collected by the Multiprofessional Health Teams of SISVAN-I in December 2013, utilizing the form "Daily follow-up map of children," on the occasion of the routine nutritional surveillance in which the first author participated at that time.
Primary healthcare services were provided to indigenous people in the study area by the Upper Solimões River Special Indigenous Sanitary District (
Distrito Sanitário Especial Indígena Alto Rio Solimões), which is part of the Indigenous Healthcare Subsystem.
This district was also responsible for nutritional surveillance of residents of approximately 188 local indigenous communities. Data analyzed in the present study were registered in 2013 in indigenous communities by teams of health professionals during nutritional surveillance activities. Data were registered on a SISVAN-I form, "Daily Map of Pregnant Women and Children Monitoring (priority <5 years)", used to monitor nutritional status and facilitate prevention, identification, and resolution of nutritional problems. Information collected includes the demographic values age and sex and the anthropometric measurements weight and height.
The study sought to include the entire population (universe) of indigenous children under five years, in the region (pertaining to all ethnic groups), with no sampling technique being employed. Criteria for exclusion from analysis were: absence of information on the form for sex, weight, height, date of birth, or date of assessment, as well as duplicate records. The study population totalled 8,692 children identified on forms, of whom 1,172 were excluded from analyses. Our analyses assumed that missing data were randomly distributed with respect to outcome variables and therefore that exclusion did not introduce systematic bias.
Study variables were: date of birth, date of measurement, sex, and anthropometric measurements (weight and height or, for children under 24 months of age, weight and length). Percent coverage was calculated for municipalities and regional centers (
polos base) of the Upper Solimões River Special Indigenous Sanitary District according to technical guidelines governing nutritional surveillance within the Indigenous Healthcare Subsystem,
21 whereby the number of children under five accompanied during the month is divided by the total number registered.
Most weight and height measurements were taken in primary healthcare units located in communities by Indigenous Health Agents appropriately trained and supervised by nursing professionals in accordance with SISVAN-I procedures.
22 To minimize data loss and bias due to absence, three attempts were made to actively seek previously unassessed children under five years of age by household visits by Indigenous Health Agents. To reduce measurement and data entry bias, all assessments were made following standard SISVAN-I procedures by members of Multiprofessional Health Teams (nurses, nursing technicians, nutritionists, and indigenous health agents) trained and supervised by the first author (FGM), who established and implemented the SISVAN-I in the Upper Solimões River Special Indigenous Sanitary District in 2006.
22Weight was measured with a portable spring scale manufactured by Cauduro (model 210-GA), with 25 kg capacity and 100 g sensitivity. Length of children under 24 months of age was measured in supine position with a portable aluminum anthropometer manufactured by Equipel, with range of measurement from 0.35 to 2.00 m and sensitivity of 5 mm. This anthropometer was also used to measure the height of children from 24 months of age in standing position. All measurements were taken with the child wearing minimal clothing and barefoot.
Data entry was performed no Epi Info 7.0 twice, and the two resulting databases were compared for divergences, which were researched and corrected manually by consulting the original instruments.
The indices height-for-age or length-for-age (H/A), weight-for-age (W/A), weight-for-height or weight-for-length (W/H), and body mass index-for-age (BMI/A) were calculated as recommended by the Brazilian Ministry of Health and the World Health Organization (WHO). Growth reference curves proposed by the WHO were used to calculate Z-scores.
23 Values less than −2 for H/A (chronic undernutrition), W/A (underweight), W/H (wasting), and BMI/A(thinness) were classified as low. Z-score values greater than +2 for W/H and BMI/A were classified as overweight. Values from −2 to +2 were classified as eutrophy. All anthropometric indices were calculated using the software Anthro version 3.2.2.
24Anthropometric indices that exceeded biological plausibility per WHO guidelines were excluded (n=10; 0.13%).
25 Prevalence of low and overweight indice values were described according to sex and age group.
Statistical analyses were conducted using IBM SPSS Statistics, version 21.0 for Windows (SPSS Inc. , Chicago, Illinois).
Descriptive statistics were calculated for all anthropometric indices (H/A, W/A, W/H, and BMI/A). Prevalence of four nutritional categories (chronic undernutrition, wasting, eutrophy, and overweight) was estimated for children of both sexes and for males and females separately. Differences were evaluated using the chi-squared test with a significance level of 95%.
This study was approved by the Research Ethics Committee of the Federal University of Amazonas (UFAM) under Opinion Nº 721204 and by the National Commission for Research Ethics, National Health Council (CONEP/CNS) under CAAE Nº 26050913.0.0000.5020. In addition, it had the consent and support of the Special Indigenous Health Secretariat, Ministry of Health (SESAI-MS) through the Upper Solimões River Special Indigenous Sanitary District (DSEI-ARS) and the Upper Solimões River Indigenous Health District Council (CONDISI).
ResultsOf a total of 7,520 Indigenous children analyzed, 49.6% (3,730) were female. The overall means for age, weight, and height were 27 months (SD=16.8), 11.20 kg (SD=3.3), and 82.3 cm (SD=13.4), respectively.
Nutritional assessment coverage by SISVAN-I was 86.0% (7,520) (Table 1). Participation was high, with some losses due to recording error, inconsistent values, or missing measurements (weight or height). Coverage by municipality varied from 91.5% (Santo Antônio do Içá) to 58.0% (Tonantins). Of the 12 regional centers, 10 had assessment coverage values above 86.0%.
The percentage of data included in analyses from 97.3% for BMI/A to 99.4% for W/H, with very few values being excluded due to biological implausibility. Significant differences were not observed in data completeness between sexes, age groups, or regional centers, suggesting data consistency (data not presented in tables).
The H/A index presented the lowest mean Z-score values. Beginning at 12 months, mean values were especially low, reaching −1.95 among children ≥ 36 months (Figure 1). Mean Z-score values for the W/A index also remained below zero, tending to decrease with age and reaching −1.04 in the age group ≥ 48 months. Mean Z-score values for the indices W/H and BMI/A remained slightly above zero, reaching a maximum value of 0.5.
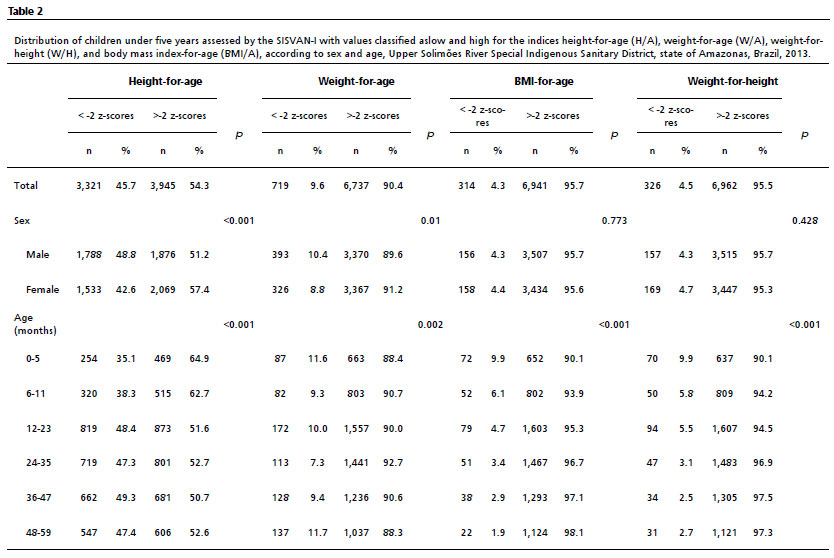
Prevalence results for four indicators are presented in Table 2 by gender and age group. Low H/A and low W/A were observed in 45.7% (varying from 35.1% to 49.3% according to age group) and 9.6% (varying from 7.3% to 11.7% according to age group) of children, respectively. Boys presented significantly higher prevalence of low H/A (48.8%) than girls (42.6%), as well as higher prevalence of low W/A (10.4% for boys and 8.8% for girls) (
p≤0.05).Higher prevalence of low H/A was observed among younger children (0 to 11 months). Prevalence of low W/A was elevated during the first months of life (11.6%) and among older children (11.7%). All anthropometric indices were significantly different in relation to age (
p≤0.05).
Low W/H and low BMI/A afflicted 4.5% and 4.3% of children, respectively, with no significant differences between the sexes (
p>0.05). Elevated W/H and BMI/A (z-scores ≥ +2) were observed in 8.8% and 10.7%, respectively, of children with nonsignificant differences between sexes.
DiscussionThe present study shows a very unfavorable nutritional scenario for indigenous children under five years attended by the Upper Solimões River Special Indigenous Sanitary District in 2013. The most notable finding was chronic undernutrition (low H/A) among nearly half (45.7%) of the 7,520 children analyzed, affecting all age groups and both sexes. This value is nearly double that documented in Brazil for indigenous children in the same age group nationally (25.7%) but only slightly higher than in the North region (40.8%).
4 Prevalence of chronic undernutrition among indigenous children in the Upper Solimões River was 6.4 times greater than in the general (primarily non-indigenous) population nationwide (7.0%) and 5.4 times greater than in the general population in the North region (8.4%).
2The prevalence of low W/A (acute undernutrition) observed among indigenous children in the Upper Solimões (9.6%) is close to that documented for the North region by the National Survey (11.4%).
4 Compared with the prevalence reported for the general population nationwide (2.9%),
2 the profile of wasting among indigenous children in the Upper Solimões region and the North region is severe. The frequency of low W/H among indigenous children in the Upper Solimões (4.5%) was nearly four times greater than observed in the national general population.
2The nutritional profile of indigenous children in the Upper Solimões River region in 2013 revealed great inequalities relative to the general population at the national and regional levels. Nutritional surveys conducted in this border region suggests that the nutritional profile of indigenous children is marked by a high frequency of chronic undernutrition both in rural areas (59.4%
versus 29.1% among non-indigenous children) and in urban areas (33.8%
versus 19.3% among non-indigenous children).
6 According to Vieira
et al. ,
26 indigenous children pertaining to the Tikuna ethnic group, the most populous in the study region, have 2.47 times greater chance of presenting H/A deficit than non-indigenous children in the same region. Socioeconomic data suggest indigenous children in the Upper Solimões region are inserted in a context of high vulnerability to nutritional disorders, characterized by elevated demographic mobility in an international frontier region, rapid urbanization associated with turbulent non-indigenous occupation of the territory, low coverage and quality of health services, absence of sanitation services, comorbidities (e.g. , malaria, intestinal parasites, and diarrhea), poverty, and food insecurity.
20As demonstrated by other studies also based on data from the SISVAN-I that analyzed nutritional status among indigenous children in other regions of Brazil,
27,28 the system has proved to be an important tool for nutritional monitoring and evaluation in this population segment.
In the case of the Upper Solimões River, our analysis reaffirms the persistence of undernutrition as one of the principal health disorders among indigenous children, without indication of improvement for over three decades.
6,26,29 This scenario contributes substantially to the overall elevated burden of infectious and chronic non-communicable diseases found in the region's indigenous population.
20It is important to observe that although the coverage of the SISVAN-I throughout Amazonia is comparatively low and tends to present technical and organizational limitations with regard to data entry at the local level,
27,30 the SISVAN-I coverage in our study region was high, and inconsistent data levels were low, allowing for a robust analysis. The observed high prevalence levels of unfavorable nutritional indicators point to the need for regional indigenous peoples' health services to implement short and long-term intervention measures to mitigate the enduring high load of nutritional deficiencies in a population that lives along a complex and dispersed hydrographic network.
Unfortunately, attempts to propose such measures have not been successful due to lack of effective communicaton and engagement between policy planners, health professionals, and stakeholders in local communities, including political leaders, indigenous professionals (such as health agents, sanitation agents, and school teachers), parents, and other actors who are typically not consulted. It is insufficient to implement rapid and narrow intervention strategies such as sporadic distribution of donated basic food baskets.
As a limitation, we can cite the gap between data collection and publication, which unfortunately is common in the Brazilian scenario of studies with indigenous peoples. Knowledge on the indigenous nutritional profile in Brazil is still fragmented and has limited geographic and ethnic coverage, so that an asymmetry persists between the volume of information available. This scenario may be the result of little involvement of researchers with the theme, despite the relevance and lack of data. And the low academic-scientific incentive, causing possible time gaps. Another point to be considered is that it is not possible to extrapolate our findings for all indigenous children from the ethnic groups involved. These are limitations in the coverage of SISVAN-I.
Strengths of this study include delineation of the study area as equivalent to the most populous DSEI in the country and exceptional coverage of registered children. This is the first study in Brazil to include nutritional assessment of nearly all children under five years residing within an entire DSEI. There is opportunity for future research that employs rigorous analytical techniques, such as adjusted estimates, capable of producing even more precise results to reliably evidentiate the child undernutrition profile among indigenous children in the Upper Solimões River region.
References1. Canella DS, Duran AC, Claro RM. Malnutrition in all its forms and social inequalities in Brazil. Public Health Nutr. 2020 Aug; 23 (Suppl. 1): S29-S38.
2. Universidade Federal do Rio de Janeiro (UFRJ). Estado Nutricional Antropométrico da Criança e da Mãe: Prevalência de indicadores antropométrico de crianças brasileiras menores de 5 anos de idade e suas mães biológicas: ENANI 2019. Rio de Janeiro (RJ): UFRJ; 2022. [access in 2023 Jun 20]. Available from:
https://enani.nutricao.ufrj.br/ wpcontent/uploads/2022/02/Relatorio_Estado_Nutricional-5.pdf3. Coimbra Jr. CE, Santos RV, Welch JR, Cardoso AM, Souza MC, Garnelo L,
et al. The First National Survey of Indigenous People's Health and Nutrition in Brazil: rationale, methodology, and overview of results. BMC Public Health. 2013 Jan; 13: 52.
4. Horta BL, Santos RV, Welch JR, Cardoso AM, Santos JV, Assis AMO,
et al. Nutritional status of indigenous children: findings from the First National Survey of Indigenous People's Health and Nutrition in Brazil. Int J Equity Health. 2013 Apr; 12: 23.
5. World Health Organization (WHO). Malnutrition. [
Internet]. Geneve, Switzerland: WHO; 2020. [access in 2023 Mar 13]. Available from:
https://www.who.int/news-room/questions-and-answers/item/malnutrition6. Araújo TS, Oliveira CSM, Muniz PT, Silva-Nunes M, Cardoso MA. Desnutrição infantil em um dos municípios de maior risco nutricional do Brasil: estudo de base populacional na Amazônia Ocidental Brasileira. Rev Bras Epidemiol. 2016 Sep; 19 (3): 554-66.
7. Duarte MG, Santos SFS, Minatto G, Nobre GC, Santos JOL, Sousa TF,
et al. Estado nutricional de crianças do baixo Amazonas: concordância entre três critérios de classificação. J Hum Growth Dev. 2018 Jun; 28 (2): 139-47.
8. Escobar AL, Santos RV, Coimbra Jr CEA. Avaliação nutricional de crianças indígenas Pakaanóva (Wari'), Rondônia, Brasil. Rev Bras Saúde Matern Infant. 2003; 3 (4): 457-61.
9. Guimarães RCR, Silva HP. Estado nutricional e crescimento de crianças quilombolas de diferentes comunidades do estado do Pará. Amazônica-Revista de Antropologia. 2015 Jan; 7 (1): 186-209.
10. Alencar FH, Yuyama LKO, Rodrigues EF, Esteves AVF, Mendonça MMB, Silva WA. Magnitude da desnutrição infantil no Estado do Amazonas/AM-Brasil. Acta Amazonica. 2008 Dez; 38 (4): 701-5.
11. Alencar FH, Yuyama LKO, Nagahama D, Parente RCP. Estudo Antropométrico de pré-escolares da calha do Rio Negro, Amazonas, Brasil. II-Barcelos. Acta Amazonica. 1999 Jun; 29 (2): 293-302.
12. Castro J. Geografia da fome: o dilema brasileiro: pão ou aço. 10
th ed. Rio de Janeiro, RJ: Antares; 1984.
13. Vasconcelos FAG. Josué de Castro e a Geografia da Fome no Brasil. Cad Saúde Pública. 2008 Nov; 24 (11): 2710-17.
14. Garnelo L, Brandão L. Avaliação Preliminar do Processo de Distritalização Sanitária Indígena no Estado do Amazonas. In: Coimbra Jr CE, Santos RV and Escobar AL (eds). Epidemiologia e saúde dos povos indígenas no Brasil. Rio de Janeiro, RJ: Editora Fiocruz; 2003, p. 235-57.
15. Medeiros FG. Perfil nutricional das crianças indígenas menores de cinco anos do Distrito Sanitário Especial Indígena Alto Rio Solimões, estado do Amazonas, Brasil [Dissertação]. Manaus: Universidade Federal do Amazonas; 2015.
16. Ferreira AA, Barros DC, Bagni UV. Avaliação nutricional na atenção básica: reflexões sobre práticas e saberes. Rio de Janeiro, RJ: Editora FIOCRUZ; 2018.
17. Caldas ADR, Santos RV. Vigilância alimentar e nutricional para os povos indígenas no Brasil: análise da construção de uma política pública em saúde. Physis: Rev Saúde Coletiva. 2012 Jun; 22 (2): 545-65.
18. Instituto Brasileiro de Geografia e Estatística (IBGE). Censo Demográfico 2010: Características Gerais dos Indígenas. Resultados do Universo. Rio de Janeiro (RJ): IBGE; 2012.
https://biblioteca.ibge.gov.br/visualizacao/periodicos/95/cd_2010_indigenas_universo.pdf19. Garcés CLL. Tikunas brasileiros, colombianos e peruanos: etnicidade e nacionalidade na região das fronteiras do Alto Amazonas/Solimões. Belém (PA): Museu Paraense Emílio Goeldi; 2014.
20. Belo EN, Orellana JDY, Levino A, Basta PC. Tuberculose nos municípios amazonenses da fronteira Brasil-Colômbia-Peru-Venezuela: situação epidemiológica e fatores associados ao abandono. Rev Panam Salud Pública. 2013 Nov; 34 (5): 321-9.
21. Ministério da Saúde (BR). Fundação Nacional de Saúde (FUNASA). Departamento de Saúde Indígena. Norma Técnica: Vigilância Alimentar e Nutricional para os Distritos Sanitários Especiais Indígenas. Brasília (DF): Ministério da Saúde; 2005. [access in 2018 Abr 25]. Available from:
https://acervo.socioambiental.org/sites/default/files/documents/F2D00078.pdf22. Barros DC, Silva DO, Gugelmin S. Vigilância Alimentar e Nutricional para a Saúde Indígena. Rio de Janeiro: Editora Fiocruz; 2008.
23. World Health Organization (WHO). WHO child growth standards: length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: methods and development. Geneva: WHO; 2006. [access in 2014 Mar 5]. Available from:
https://www.who.int/publications/i/item/924154693X24. World Health Organization (WHO). WHO Anthro for Personal Computers, versão 3.2.2 de 2011: Software for assessing growth and development of the world's children. Geneva: WHO; 2010. [access in 2014 Jul 10] . Available from:
https://cdn.who.int/media/docs/default-source/child-growth/child-growth-standards/software/anthro-pc-manual-v322.pdf?sfvrsn=c4e76522_225. World Health Organization (WHO). WHO AnthroPlus for personal computers manual: software for assessing growth of the world's children and adolescents. Geneva: WHO; 2009. [access in 2014 Jul 10] . Available from:
https://cdn.who.int/media/docs/default-source/child-growth/growth-reference-5-19-years/who-anthroplus-manual.pdf?sfvrsn=ddd24b2_126. Viera AA, Braga JU, Moraes CL. Condições de saúde e nutrição de crianças indígenas e não-indígenas que vivem às margens do rio Solimões, Estado do Amazonas, Brasil. [Carta] Cad Saúde Pública. 2000; 16 (3): 873.
27. Pantoja LN, Orellana JDY, Leite MS, Basta PC. Cobertura do Sistema de Vigilância Alimentar e Nutricional Indígena (SISVAN-I) e prevalência de desvios nutricionais em crianças Yanomami menores de 60 meses, Amazônia, Brasil. Rev Bras Saúde Matern Infant. 2014; 14 (1): 53-63.
28. Silva OLO, Lindemann IL, Prado SG, Freitas KC, Souza AS. Vigilância alimentar e nutricional de crianças indígenas menores de cinco anos em Mato Grosso do Sul, 2002-2011. Epidemiol Serv Saúde. 2014; 23 (3): 541-6.
29. Araújo TL, Lopes MVO, Cavalcante TF, Guedes NG, Moreira RP, Chaves ES,
et al. Análise de indicadores de risco para hipertensão arterial em crianças e adolescentes. Rev Esc Enferm USP. 2008 Mar; 42 (1): 120-6.
30. Ministério da Saúde (BR). Secretaria Especial de Saúde Indígena. Departamento de Atenção à Saúde. Coordenação Geral de Atenção Primária à Saúde Indígena. Divisão de Ações de Saúde Indígena. Saúde indígena: análise da situação de saúde no SasiSUS. Brasília (DF): Ministério da Saúde; 2019. [access in 2023 Jun 19]. Available from:
https://pesquisa.bvsalud.org/bvsms/resource/pt/mis-40418Received on January 2, 2023
Final version presented on June 5, 2023
Approved on June 25, 2023
Associated Editor: Paola Mosquera
Author's contribution: Medeiros FG: study design, data collection. Organization, supervision of data entry and consolidation of the database. Participated in the analysis, interpretation and discussion of data and writing of the manuscript. Mainboug EMT: participated in the design of the study. Contributed to the interpretation of data and writing of the manuscript. Ferreira AA: contributed to the structuring of the manuscript, data analysis and interpretation. Balieiro AAS: contributed to the structuring of the study, data processing and statistical analysis. Welch JR and Coimbra Jr. CEA: contributed to the structuring of the manuscript, data analysis, interpretation and discussion. All authors approved the final version of the article and declare no conflict of interest.


 ; Evelyne Marie Therese Mainbourg2
; Evelyne Marie Therese Mainbourg2







 Ler em português
Ler em português