ABSTRACT
OBJECTIVES: to investigate the association between sociodemographic, gestational/puerperal factors and postpartum weight retention (PPWR) after 12 months in Brazilian women at a university hospital.
METHODS: prospective cohort with puerperal women recruited at the maternity ward of a university hospital in a Brazilian metropolis. At baseline (n=260), sociodemographic and anthropometric information on the mother-child binomial and data related to the gestational period were collected. Maternal dietary patterns were measured using a food frequency questionnaire and subsequently determined by Principal Component Analysis.
RESULTS: 75 women, with a mean age of 28.4 years (CI95%= 27.0-29.7), 25.3% with excessive PPPR, with an average of 3.6 kg (CI95%= 1.7) continued in the follow-up. -5.4). Higher gestational weight gain (GWG) (β= 0.36; CI95%= 0.18-0.70) and lower maternal age (β= -0.41; CI95%= -0.92--0.22) were PRPP predictors (p≥0.001) (adjusted for per capita income, parity, type of delivery, number of prenatal visits, baby's birth weight, breastfeeding and physical activity).
CONCLUSION: there was a high occurrence of excessive PPPR, favored by higher GPG and lower maternal age. This highlights the importance of monitoring women's health during the reproductive period, with guidance on ways of life (diet and physical activity), to favor better outcomes for mother-child.
Keywords:
Maternal health, Postpartum period, Risk factors, Weight gain during pregnancy, Postpartum weight retention
RESUMO
OBJETIVOS: investigar a associação entre fatores sociodemográficos, gestacionais/puerperais com a retenção de peso pós-parto (RPPP) após 12 meses em mulheres brasileiras em hospital universitário.
MÉTODOS: coorte prospectiva com puérperas recrutadas na maternidade do hospital universitário de uma metrópole brasileira. Na linha de base (n=260) foram coletadas informações sociodemográficas, antropométricas do binômio mãe-filho e dados relativos ao período gestacional. O padrão alimentar materno foi mensurado por meio do questionário de frequência alimentar e posteriormente determinado pela Análise de Componentes Principais. A RPPP foi classificada como risco para obesidade se ≥7,5Kg.
RESULTADOS: 75 mulheres continuaram no seguimento, com média de 28,4 anos de idade (IC95%= 27,0-29,7), 25,3% com RPPP excessiva, sendo em média 3,6 Kg (IC95%= 1,7-5,4). Maior ganho de peso gestacional (GPG) (β= 0,36; IC95%= 0,18-0,70) e menor idade materna (β= -0,41; IC95%= -0,92--0,22) foram preditores da RPPP (p≥0,001) (ajustado pela renda per capita, paridade, tipo de parto, número de consultas pré-natal, peso ao nascer do bebê, aleitamento materno e atividade física).
CONCLUSÃO: evidenciou-se elevada ocorrência de RPPP excessiva, favorecida pelo maior GPG e menor idade materna. Aponta-se assim a importância do monitoramento da saúde da mulher durante o período reprodutivo, com orientações sobre modos de vida (alimentação e atividade física), para favorecer melhores desfechos para mãe-filho.
Palavras-chave:
Saúde materna, Período pós-parto, Fatores de risco, Ganho de peso na gestação, Retenção de peso pós-parto
IntroductionIt is essential to care for and pay attention to every cycle of a woman's health, especially during pregnancy and postpartum, which are periods of risk for the development of obesity.
1 Municipal data show that 15% and 40% of adult women are obese and overweight, in this order.
2 In Brazil, such data is highly common. The search conducted by Vigitel 2021 (Monitoring Risk Factors and Protection against Chronic Diseases via Telephone Questionnaire) identified that 46.7% of women aged from 18 to 44 years are overweight at some level.
3 The report from SISVAN (Monitoring System for Food and Nutrition) 2022 shows that around 67.6% of adult women present the same condition.
4Postpartum weight retention (PPWR) is one of the causes of overweight in adult fertile women. PPWR is the difference between pre-pregnancy weight (PPW) and postpartum weight.
5,6 Prospective studies indicate that less than 65% of women return to their pre-pregnancy weight in 12 months postpartum.
7PPWR reveals to have multiple causes. Pre-pregnancy eating habits need special attention because in case they are unhealthy, they can lead to excessive gestational weight gain (GWG), and unfavorable results in the mother-child binomial.
1 Sociodemographic aspects such as income, age, parity, and education level are also crucial for the nutritional habits of pregnant women.
8,9 Furthermore, anthropometric factors (such as inadequate GWG and slow postpartum weight loss) and the insufficient practice of physical exercises
1 are highlighted as causative factors of PPWR.
PPWR research is commonly conducted in the first weeks/months postpartum due to the higher impact of this period on maternal weight change.
7 However, it is expected that women return to their PPW in a year, and if that does not occur, the chances of long-term weight retention increase. In this case, the weight after 15 years is higher than when compared to women that return to their PPW.
10This study aimed at investigating the association between sociodemographic, gestational, and postpartum factors and weight retention 12 months postpartum, having in mind the importance of this theme and its influence on the planning of women's healthcare actions.
MethodsA prospective cohort was conducted between July 2018 and July 2020, with puerperal women recruited at the maternity ward of a university hospital in a Brazilian metropolis.
The inclusion criteria for the sample were: women no more than 48 hours postpartum, aged between 20 to 40 years, with live full-term babies, in good health, and willing to participate in the study. The exclusion criteria were: women in a multiple pregnancy, or women who reported having gestational diabetes
mellitus or pre-pregnancy diabetes
mellitus. Women who reported pre-eclampsia or complications in maternal-child health that demanded medical healthcare during the study period or the absence of anthropometric data that allowed the calculation of weight retention 12 months postpartum were also exclusion criteria.
The first contact was made soon after giving birth, and the participants answered questions related to their birthday, age, occupation, address, family income, level of education and marital status. Gestational and puerperal data related to eating habits were also part of the initial data collection.
Data on the gestational and puerperal period were self-referred: the number of prenatal visits,
11 PPW and GWG,
12 type of delivery, parity status, physical exercise during pregnancy, and breastfeeding data (BF). Additionally, the gestational age was obtained from the medical report.
The height was measured with an anthropometer assembled to a Welmy
® scale. Pre-pregnancy BMI (weight/height
2) was calculated and classified according to the World Health Organization.
12 The postpartum weight was gotten from the participants' records.
The gestational food intake of the participants was evaluated using the Food Frequency Questionnaire (FFQ), semi-quantitative, validated for the Brazilian adult population
14 and with reference to the last six months of pregnancy. This tool presents 52 food items divided into the following groups: milk and dairy products; meat and eggs; oils; snacks and canned food; cereals and legumes; vegetables and fruits; desserts and sweets; beverages; diet and light ultra-processed products. The questionnaire had the following seven options for frequency of consumption: once a week; twice or more times a day; five to six times a week; twice to four times a week; once a week; once to three times a month; rarely or never. Such information was collected to identify the dietary patterns
a posteriori. 15The minimum sample size (n=260) was estimated by means of a formula for sample size definition in which the number of individuals in the study must be five times higher than the number of items in the food intake data collection instrument. In this way, the gestational dietary pattern could be identified.
15The dietary patterns were identified by the Principal Component Analysis (PCA),
15 using an orthogonal rotation (
Varimax) to highlight the interpretation of each factor. First, the number of items in the questionnaire was reduced from 52 individual items to 19 groups of foods or foods individually to extract the dietary patterns. The dietary patterns described by each factor were interpreted by factorial loads. The foods and groups of foods that had a factorial load higher or equal to 0.2 in the rotated matrix reflected a strong association with the components and, therefore, were used as part of the dietary patterns.
A year after the initial data collection, a similar questionnaire was applied at the consultation. It contained information about breastfeeding, current physical exercise practices, and current maternal weight (12 months postpartum), obtained with a
Welmy® scale.
65% of the women invited (n=260) did not show up for the follow-up meeting and were contacted via telephone and answered a questionnaire similar to the one applied at the in-person meetings. In case the participant did not answer the first phone call, we tried again twice on different days and times. Of these invited women, 20 attended the in-person meetings and 55 agreed to answer the questionnaire via phone call.
Sensitivity analysis between the groups was conducted (n=20 from in-person and n=55 from phone calls) for further joint and data analysis. No significative differences were found concerning the sociodemographic variables between the groups according to the way of contact - in-person or phone call, allowing the joint analysis.
Thus, the analysis was composed of 75 women and their newborns, representing 29% of the initial sample and with 60% of sampling power in the finite sample, from the average PPWR, considering a 95% confidence interval and 5% sampling error.
PPWR is the absolute difference between the 12 months postpartum weight, taken in the in-person meeting and self-referred in the phone calls, and the PPW. When the PPWR was higher or equal to 7.5 kg,
5,6 it was classified as a risk of developing obesity, and it was called "excessive retention" in this study.
The database was built with the help of
Epilnfo™ 3.5.1 through double typing, and after proper consistency analysis, the descriptive and bivariate analyses were done. The normality of the distribution of the variables was verified through the
Kolmogorov-Smirnov test. A descriptive analysis of the data was performed through absolute and relative frequencies, measures of the central tendency, and dispersion. The quantitative variables were described in average and 95% confidence interval.
The T-student and ANOVA tests were used to compare the average of independent variables and the outcome (12 months postpartum weight retention). The correlation test of Spearman was used to assess the correlation between the variable outcome and the quantitative variables.
The associations between the explicative variables and 12 months postpartum weight retention were determined by the linear regression model. The variable that presented
p<0,20 in the bivariate analysis were included in the model, with backward elimination. The final adjustment of the model was performed by variables considered important by the literature in relation to the outcome:
per capita income, parity, type of delivery, number of prenatal visits, baby's birth weight, BF 12 months postpartum, and physical exercise 12 months postpartum. The final model significance was assessed by the F-test of the variance analysis and the adjustment quality by the coefficient of determination (R
2).
The analyses were performed using the software Statistical Package for the Social Sciences (SPSS) 20.0. The significance level adopted was 5% (
p <0.05) for all the analyses performed.
This study was approved by the Committee of Ethics in Research (COEP) under the number 86818118.0.0000.5149.
ResultsOf the 260 women who agreed to participate in the study, 75 stayed until the final stage of follow-up (12 months postpartum). The sample presented a mean age of 28.4 years (CI95%= 27.0 - 29.7); 67.6% finished high school, were multiparous (53.7%) and 45.3% started the pregnancy with some degree of overweight. Excessive PPWR (≥7.5Kg) was identified in 25.3% of the sample. Only 10.7% of women returned to their PPW 12 months postpartum. Other maternal characteristics are shown in Table 1.

Three different dietary patterns were identified during the Principal Component Analysis. They referred to the gestational period (n=260), corresponding to 33.14% of the total variance (Table 2). The first pattern, "Pattern 1", was composed of Italian bread, fresh meat and eggs, cereals, tubers, beans, processed foods, cold meats and sausages, and fast food (14.44%). The second pattern, "Pattern 2" covered vegetables, fruits and fruit juice, and olive oil (9.86%). Finally, "Pattern 3" was composed of milk, ultra-processed dairy products, and cheese (8.33%). Only "Pattern 1" showed an association with PPWR (
p<0.05).
Weight retention 12 months postpartum presented an average of 3.6kg (CI95%= 1.7 -5.4 Kg), and there was a correlation between PPWR and higher GWG (r=0.35;
p=0.003); and the association with the dietary pattern 1 (
p=0.01) and BF 12 months (
p=0.04) (Table 1).
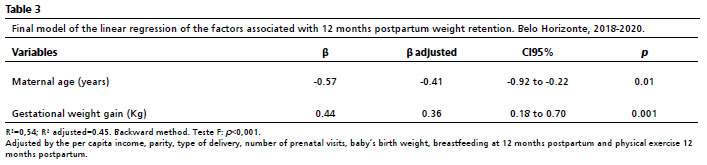
The highest GWG (β= 0.36; CI95%= 0.18-0.70) and the lowest maternal age (β= -0.41; CI95%= -0.92--0.22) were predictors of weight retention 12 months postpartum and they explained almost 45% of the variation of this outcome, after adjustments for
per capita income, parity, type of delivery, number of prenatal visits, baby's birth weight, BF 12 months postpartum and physical exercise (Table 3).
DiscussionIn this study, there was a high prevalence of excessive PPWR, associated with higher GWG and lower maternal age, regardless of the adjustments. PPWR was also associated with Pattern 1 (Italian bread, fresh meat and eggs, cereals, tubers, beans, processed foods, cold meats and sausages, and fast food
). The prevalence and average PPWR identified were similar to the ones found in other studies and show the importance of investigations about this topic for woman's health.
5,6,9,16,17Although the pre-pregnancy nutritional state is not directly associated with PPWR in this investigation, the weight gain during pregnancy was evident, which is highlighted in the literature with similar characteristics.
18 A meta-analysis that considered more than 65 thousand women showed that GWG above the recommendation can be kept until 20 years postpartum.
19 It is essential to mention that the higher the GWG, the higher difficulty and time required to lose it. That was seen in another meta-analysis
20 that suggested that inadequate GWG leads to higher short and long-term PPWR, increasing the chances of developing or maintaining obesity.
PPWR is multifactorial and it is noted that the woman's pre-pregnancy nutritional state is among its most relevant contribution. The current guidelines
21 point to the importance of a eutrophic state in the reproductive period and early pregnancy in order to allow moderate GWG and consequently provide less weight retention, with a return to weight retention within one year postpartum. This study showed that more than 40% of women began the pregnancy with some degree of overweight and only 10% returned to their PPW, with similar results also found in another Brazilian study.
18 In a cohort with North American women aged between 14 to 21 years (n=4.436), it was identified that 60% began pregnancy with overweight/obesity and had an average retention of 2.9 kg.
22 Mahabamunuge
et al. 16 found average weight retention of 3.4 kg six months postpartum in 348 American women and around 31% PPWR.
Similar findings were seen in a national study that followed 266 women during pregnancy until nine months postpartum.
6 Moreover, in a cohort study in Pelotas that assessed 4.098 women, a prevalence of postpartum weight was found, with an average PPWR lower in the same period (1.4 Kg).
7 However, even though they are very different, these numbers are high, considering the impact of long-term weight retention on the woman's health with a higher chance of developing overweight, obesity, and other downsides.
Regarding the findings about the association of higher PPWR with lower maternal age, Kac
et al. ,
6 also identified higher PPWR among women with lower age (<23 years). These results can be attributed to the early beginning of the reproductive cycle, a predictor for the development of postpartum obesity,
6 as well as the dietary pattern observed in young pregnant women.
A cross-sectional study
23 (n=1.035) conducted with Brazilian pregnant women identified 2.9 more chances of ultra-processed foods intake (CI95%= 1.68-5.17;
p<0.001) in the participants aged ≤ 19 years. A diet with a higher presence of this type of food is harmful to women's health due to the high content of sugar, fat, and sodium present in these products, which increase overweight, obesity, and other non-transmissible chronic diseases
24 These findings are corroborated in studies from other places
25,26 and show higher consumption of ultra-processed food in young pregnant women.
Additionally, the positive association found between dietary pattern 1 and increased PPWR corroborates and extends the results observed in the literature. A systematic review, based on 11 studies of cohort and cross-sectional design, pointed out that higher adherence to mixed and Western dietary patterns rich in ultra-processed foods during pregnancy was associated with a higher prevalence of excessive GWG (24.48-55.20%). This result is due to the unbalance in the energy, macro, and micronutrient supply, which can contribute to undesirable outcomes such as inadequate fetal growth, excessive fat accumulation, and metabolic complications.
27In addition to the data found in relation to GWG, the gestational dietary pattern is also pointed out as interfering with postpartum weight gain. Despite the change in dietary patterns according to the country/population assessed, the literature findings demonstrate a positive association between adherence to unhealthy, Western, and sugar/fat-rich dietary patterns with negative health outcomes.
27 A study conducted with Brazilian women observed that a high intake of saturated fat and processed foods (present in Pattern 1) during pregnancy revealed a significant increase in PPWR, especially in the first 15 days.
28 A Norwegian cohort also found that adherence to national guidelines, consistent with a dietary pattern similar to traditional, healthy, and prudent ones, resulted in lower postpartum weight gain over the following eight years when compared with women who had low adherence to this diet.
29Among the positive aspects of this study is the breadth of the postpartum evaluation period, since studies commonly evaluate shorter intervals postpartum. However, it is worth pointing out some limitations such as follow-up loss and the obtaining of self-reported data. Given the longitudinal structure of the work, losses were expected, especially given the period evaluated. In a paper investigating a similar theme
1, the authors observed that in the Brazilian context, cohort studies during the pregnancy-puerperal period report difficulty in the follow-up.
However, a complementary data collection was carried out with women who did not attend the in-person meeting, although with low adherence. The COVID-19 pandemic that broke out during the completion of the collection also partially explains the losses in data collection. Another issue is that GWG and PPW are self-reported by the woman, which can lead to underestimations. However, it is important to note that studies have validated and found high agreement between self-reported and taken measures, demonstrating accuracy in the reported measures.
12,30In summary, the results of this work demonstrated a high occurrence of excessive PPWR, which was favored by higher GWG and lower maternal age. These data denote the importance of monitoring women's postpartum nutritional status, as pointed out in other investigations, in order to assist in the gradual return to pre-pregnancy weight. It is also necessary to improve the structure of prenatal care, giving attention to nutrition, and consequently continuous follow-up of the GWG, with more attention to vulnerable groups, such as younger mothers. Moreover, the offer of guidance on lifestyles (diet and physical exercise) pertinent to the socioeconomic contexts of each woman also deserves relevance.
Finally, we point out the demand for public policies directed to the integral care of puerperal women, especially during the first postpartum year, considered critical in the return to PPW, with long-term impacts on women's health.
References1. Martins APB, Benicio MHD. Influência do consumo alimentar na gestação sobre a retenção de peso pós-parto. Rev Saúde Pública. 2011; 45 (5): 870-7.
2. World Health Organization (WHO). Obesity and overweight. [
Internet]. [access in 2021 Out 5]. Available from:
https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight3. Ministério de Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Análise em Saúde e Vigilância de Doenças Não Transmissíveis. Vigitel Brasil 2021: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico: estimativas sobre freqüência e distribuição sociodemográfica e fatores de risco e proteção para doenças crônicas nas capitais dos 26 Estados Brasileiros e no Distrito Federal em 2021. Brasília (DF): Ministério de Saúde; 2022. [access in 2021 Out 5]. Available from:
https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/svsa/vigitel/vigitel-brasil-2021-estimativas-sobre-frequencia-e-distribuicao-sociodemografica-de-fatores-de-risco-e-protecao-para-doencas-cronicas4. Ministério da Saúde (BR). Secretária de Atenção Básica à Saúde. Sistema de Vigilância Alimentar e Nutricional - SISVAN: Relatórios do Estado nutricional dos indivíduos acompanhados por período, fase do ciclo da vida e índice. Brasília (DF): Ministério da Saúde; 2023. [access in 2023 Fev 28]. Available from:
https://sisaps.saude.gov.br/sisvan/relatoriopublico/index5. Vasconcelos CMCS, Costa FS, Almeida PC, Araujo Júnior E, Sampaio HAC. Fatores de risco associados à retenção de peso seis meses após o parto. Rev Bras Ginecol Obstet. 2014; 36 (5): 222-7.
6. KAC G, Benicio MHDA, Velásquez-Meléndez G, Valente JG. Nine months postpartum weight retention predictors for Brazilian women. Public Health Nutrition. Cambridge University Press; 2004; 7 (5): 621-8.
7. Flores TR, Nunes BP, Miranda VIA, Silveira MF, Domingues MR, Bertoldi AD. Ganho de peso gestacional e retenção de peso no pós-parto: dados da coorte de nascimentos de 2015, Pelotas, Rio Grande do Sul, Brasil. Cad Saúde Pública. 2020; 36 (11): e00203619.
8. Castro MBT, Kac G, Sichieri R. Padrão de consumo alimentar em mulheres no pós-parto atendidas em um centro municipal de saúde do Rio de Janeiro, Brasil. Cad Saúde Pública. 2006; 22 (6): 1159-70.
9. Chagas DC, Silva AAM, Ribeiro CCC, Batista RFL, Alves MTSSB. Efeitos do ganho de peso gestacional e do aleitamento materno na retenção de peso pós-parto em mulheres da coorte BRISA. Cad Saúde Pública 2017; 33 (5): e00007916.
10. Rode L, Kjærgaard H, Ottesen B, Damm P, Hegaard H. Association between gestational weight gain according to body mass index and postpartum weight in a large cohort of Danish women. Matern Child Health J. 2012 Fev; 16 (2): 406-13.
11. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Área Técnica de Saúde da Mulher. Pré-natal e Puerpério: atenção qualificada e humanizada - manual técnico. 3ª ed. Brasília (DF): Ministério da Saúde; 2006. [access in 2021 Out 5]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/manual_pre_natal_puerperio_3ed.pdf12. Araújo RGPS, Gama SGN, Barros DC, Saunders C, Mattos IE. Validade de peso, estatura e IMC referidos por puérperas do estudo Nascer no Brasil. Rev Saúde Pública. 2017; 51: 115.
13. Organização Mundial da Saúde (OMS). Physical status: the use and interpretation of anthropometry. Geneva: WHO; 1995. [access in 2023 Fev 28]. Available from:
https://apps.who.int/iris/bitstream/handle/10665/37003/WHO_TRS_854.pdf?sequence=1&isAllowed=y14. Ribeiro AC, Sávio KEO, Rodrigues MLCF, Costa THM, Schmitz BAS. Validação de um questionário de frequência de consumo alimentar para população adulta. Rev Nutr. 2006; 19 (5): 553-62.
15. Olinto MTA. Padrões alimentares: análise de componentes principais. In: Kac G, Sichieri R, Gigante DP, organizadores. Epidemiologia nutricional [
Internet]. Rio de Janeiro: Editora FIOCRUZ/Atheneu, 2007. p. 213-25. Available from: SciELO Books: <
http://books.scielo.org>16. Mahabamunuge J, Simione M, Hong B, Horan C, Ayala SG, Davison K,
et al. Association of sugar-sweetened beverage intake with maternal postpartum weight retention. Public Health Nutr. 2021 Sep; 24 (13): 4196-203.
17. Huang Z, Li N, Hu YM. Dietary patterns and their effects on postpartum weight retention of lactating women in south central China. Nutrition. 2019; 67-68: 110555.
18. Nast M, Oliveira A, Rauber F, Vitolo MR. Excessive gestational weight gain is risk factor for overweight among women. Rev Bras Ginecol Obstet. 2013 Dec; 35 (12): 536-40.
19. Nehring I, Schmoll S, Beyerlein A, Hauner H, von Kries R. Gestational weight gain and longterm postpartum weight retention: a metaanalysis. Am J Clin Nutr. 2014 Out; 94 (5): 1225-31.
20. Mannan M, Suhail AD, Abdullah AM. Association between weight gain during pregnancy and postpartum weight retention and obesity: a bias-adjusted meta-analysis. Nutr Rev. 2013 Jun; 71 (6): 343-52.
21. Institute of Medicine; National Research Council. Weight gain during pregnancy: reexamining the guidelines. Washington (DC): National Academies Press; 2009.
22. Leonard S, Rasmussen K, King J, Abrams B. Trajectories of maternal weight from before pregnancy through postpartum and associations with childhood obesity. Am J Clin Nutr. 2017 Nov; 106 (5): 1295-1301.
23. Pereira MT, Cattafesta M, Santos Neto ET, Salaroli LB. Maternal and Sociodemographic Factors Influence the Consumption of Ultraprocessed and Minimally-Processed Foods in Pregnant Women. Rev Bras Ginecol Obstet. 2020 Jul; 42 (7): 380-9.
24. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Guia alimentar para a população brasileira. 2
nd ed. Brasília (DF): Ministério da Saúde; 2014. [access in 2021 Out 5]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/guia_alimentar_populacao_brasileira_2ed.pdf25. Teixeira JA, Castro TG, Grant CC, Wall CR, Castro ALDS, Francisco RPV,
et al. Dietary patterns are influenced by socio-demographic conditions of women in childbearing age: a cohort study of pregnant women. BMC Public Health. 2018 Mar; 18 (1): 301.
26. Hutchinson AD, Charters M, Prichard I, Fletcher C, Wilson C. Understanding maternal dietary choices during pregnancy: The role of social norms and mindful eating. Appetite. 2017 May; 112: 227-34.
27. Ferreira LB, Lobo CV, Miranda AEDS, Carvalho BDC, Santos LCD. Dietary Patterns during Pregnancy and Gestational Weight Gain: A Systematic Review. Rev Bras Ginecol Obstet. 2022 Mai; 44 (5): 540-57.
28. Martins APB, Benicio MHD. Influência do consumo alimentar na gestação sobre a retenção de peso pós-parto. Rev Saúde Pública. 2011 Out; 45 (5): 870-7.
29. Skreden M, Hillesund ER, Wills AK, Brantsæter AL, Bere E, Øverby NC. Adherence to the New Nordic Diet during pregnancy and subsequent maternal weight development: A study conducted in the Norwegian Mother and Child Cohort Study (MoBa). Br J Nutr. 2018 Mai; 119 (11): 1286-94.
30. Han E, Abrams B, Sridhar S, Xu F, Hedderson M. Validity of Self-Reported Pre-Pregnancy Weight and Body Mass Index Classification in an Integrated Health Care Delivery System. Paediatr Perinat Epidemiol. 2016 Jul; 30 (4): 314-9.
Received on November 17, 2022
Final version presented on April 25, 2023
Approved on April 28, 2023
Associated Editor: Melânia Amorim
Acknowledgments: We thank the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES - Código Financeiro 001), Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq - Productivity Scholarship in Research (301555/2019-2) and Edital Universal 2016 (406644 /2016-0) for the financial support.
Author’s contribution: Carvalho BC: performed the bibliographic review, conception, interpretation of data, and final writing. Ferreira LB e Santos TN performed the bibliographic review, analysis, interpretation of data, and final writing. Vieira and Souza RC performed a critical analysis of the results and the paper revising. Santos LC guided the research, performed a critical analysis of the results, supported the writing, and revised and approved the final version of the manuscript. All the authors approved the final version of the article and declare no conflict of interest.


 ; Larissa Bueno Ferreira2
; Larissa Bueno Ferreira2







 Ler em português
Ler em português