ABSTRACT
OBJECTIVES: to determine and characterize the prevalence of congenital malformations among live births in Rondônia, from 2015 to 2019.
METHODS: an ecological study was conducted using publicly available data at Sistema de Informações sobre Nascidos Vivos collected in January 2021. The prevalence of congenital malformation and possible associations were calculated. The strength of the association between variables was measured using the odds ratio. Variables that were statistically significant at the 5% level were selected for adjusted odds ratio calculation using logistic regression models. The R programming language was used for all analyses and interactions with the database. A 95% confidence interval was considered.
RESULTS: a total of 1,110 records were analyzed. The overall prevalence of congenital malformation was 8.36, with higher rates observed among mothers over 35 years, those with low educational levels, unmarried status, and preterm birth. Infants with low birth weight and low Apgar scores also had higher prevalence rates of congenital malformations.
CONCLUSION: the prevalence of congenital malformations in the state was similar to the national average, but regional disparities were observed and warrant further investigation.
Keywords:
Congenital anomalies, Public health surveillance, Epidemiology
RESUMO
OBJETIVOS: determinar e caracterizar a prevalência de malformações congênitas entre nascidos vivos em Rondônia, no período de 2015 a 2019.
MÉTODOS: estudo ecológico, com dados públicos disponíveis no Sistema de Informações sobre Nascidos Vivos coletados em janeiro de 2021. Foi calculada a prevalência das malformações e as possíveis associações. A força de associação entre as variáveis foi medida pela razão de odds. Aquelas variáveis consideradas estatisticamente significante ao nível de 5% foram selecionadas para o cálculo de razão de odds ajustada, usando modelo de regressão logística. A linguagem de programação R foi usada para todas as análises e interação com o banco de dados. O Intervalo de Confiança considerado foi de 95%.
RESULTADOS: foram analisados 1.110 registros. A prevalência geral de malformação congênita foi de 8,36, sendo maior entre mães com idade acima de 35 anos, baixa escolaridade, solteiras, com partos prematuros; crianças com baixo peso ao nascer e baixos escores de Apgar.
CONCLUSÃO: a prevalência de malformação congênita no estado foi próxima da nacional, mas houve discrepâncias entre as regiões de saúde que merecem uma investigação futura.
Palavras-chave:
Anormalidades congênitas, Vigilância em saúde pública, Epidemiologia
IntroductionCongenital malformations (CM) are functional, neuromotor, and/or morphological changes consisting of malformations, rupture, deformations, and dysplasia, which occur during embryonic development and are present at birth or manifest themselves later in life.
1These anomalies can result from genetic factors, environmental factors, the combination of both, or exposure to infectious agents harmful to the fetal formation, such as rubella, human immunodeficiency virus (HIV), and Zika virus, in addition to the use of licit and illicit drugs, teratogenic substances, radiation, and maternal endocrine diseases. The anomalies can be isolated or present in a combination or characteristic pattern that can affect one or more organ systems.
2MCs are important causes of newborns (NB) and child death, chronic disease, and disability, especially in low- and middle-income countries, where 95% of all deaths due to these anomalies occur.
3The World Health Organization (WHO) reports that MCs rank 17
th among causes of the global burden of disease and are responsible for approximately 7% of neonatal deaths and 25,3-38,8 million disability-adjusted life years (DALYs) worldwide. Thus, MCs can contribute to long-term disability, significantly impacting individuals, families, health systems, and societies.
4Surveillance of births, including stillbirths and elective pregnancy terminations due to fetal anomalies, is essential to identify children with malformations and determine the frequency of apparent etiologies.
5 In Brazil, these data are collected and stored in the Information System on Live Births (Sinasc) of the Ministry of Health (MS), which allows demographic and epidemiological analyses. The data are available in Sinasc are collected from the Live Births Declaration (DNV), a ministerial document that enables several analyses in the maternal and child health area,
6 helping to understand and dimension the health situation of the NB, helping to estimate risks and identify vulnerable groups, collaborating in the construction of indicators.
7However, there is a scarcity of scientific studies investigating the epidemiological data on MC prevalence and its maternal-fetal risk factors in the state of Rondônia, especially in the northern region of the country. Therefore, this study aims to determine and characterize the prevalence of congenital malformations among live births in Rondônia in the period from 2015 to 2019.
MethodsThis is an ecological study, with a description and comparison of secondary information by health regions. The MC data for the state of Rondônia, in the period from 2015 to 2019, were obtained from Sinasc in January 2021, through the website of the Department of Informatics of the Unified Health System of the Ministry of Health (DATASUS).
Rondônia is a state with a population of 1,777,225 inhabitants and a population density of 6.58hab. /km
2. It has a crude birth rate of 18.6 and a territorial area of 238,512.8 km
2, covering 52 municipalities, which corresponds to about 4.7% of the total area of the Legal Amazon. In the last 20 years, the Human Development Index had an exponential increase, from 0.407 (very low: up to 0.499) in 1991 to 0.690 (medium: 0.600-0.699) in 2010.
8For SUS organization and management, the state is divided into seven health regions: Madeira-Mamoré, Vale do Jamari, Central, Zona da Mata, Café, Cone Sul, and Vale do Guaporé. These regions will be considered units of interest in this study.
9Initially, 4,387 records (3.2%) were excluded because they did not contain information on the presence or absence of malformations. Some numerical variables were categorized to allow the association analysis with the presence of malformations. Those considered were: mother's age ("less than 35 years" or "35 years or more"); the number of previous pregnancies ("None", "One", "Two" and "Three or more"); the number of live-born children ("None", "One", "Two" and "Three or more"); the number of fetal losses ("None", "One" and "Two or more"). Regarding newborns, the following variables were considered: birth weight ("less than 2,500 grams" or "2,500 grams or more") and Apgar score on the 1st and 5th minutes of life ("Less than 7" or "Equal to or greater than 7").
The following variables were also selected: the numbers of births by place of residence of the mother; municipality of occurrence and residence (used to group the data by health regions); marital status (single, married, widowed, separated/divorced) and maternal education ("up to 7 years" of study, "8-11 years", "12 or more years"). Obstetric characteristics included the following variables: duration of pregnancy (in weeks); type of pregnancy ("single", "double", "triple or more"); type of delivery ("cesarean" or "vaginal"), and the number of prenatal visits ("none", "up to 6 times", "7 times or more"). In the newborn profile, the variables year of birth and ICD code of MC were considered.
The prevalence of congenital malformations was calculated using the formula:
Prevalence =
n of live births with malformation x 1000Total number of live births in the period
The data were consolidated in the form of coefficients and proportions. Initially, all collected variables were individually evaluated to determine their association with the presence of CM. To analyze the associations between categorical variables and the outcome of the presence of malformations, the chi-square test was used, considering a significance level of 0.05.
The strength of the association between variables was assessed by Odds Ratio (OR). The variables that showed statistically significant association were selected for inclusion in the logistic regression model. The following variables were considered significant: health region, mother's age, mother's education, marital status, number of pregnancies, number of live children, gestation length, pregnancy type, delivery type, number of prenatal visits, infant's birth weight, and first- and fifth-minute Apgar scores.
A logistic regression model was fitted to calculate the adjusted odds ratio (AOR) of the selected variables. The independent variables were included in the model simultaneously to control for the effect of each on the presence of MC.
The stepwise forward logistic regression method was used to select the variables that remained significant in the final model, considering the likelihood ratio criterion.
The fit of the model to the observed data was evaluated by the Hosmer-Lemeshow test. The p-value obtained was 0.122, indicating a good fit of the model to the data.
To assess the accuracy and fit of the model, the 95% confidence intervals for the AOR and the corresponding p values were calculated.
10 Multicollinearity among the independent variables was assessed using the Variance Inflation Factor (VIF) test, and no significant multicollinearities were observed among the independent variables included in the logistic regression model.
Sinasc presents its records by municipalities. To obtain the data by Health Regions, they were grouped taking into account the municipality of residence of the mother, classifying it in its respective health region using the statistical program. Thus, the categorical variable "Health Region" was created for the analyses.
All analyses, database preparation, prevalence calculations, OR, and confidence intervals were performed in Microsoft
® Office Excel
® and R version 4.0.1 programs.
As the data are public domain and non-identifiable, the research protocol did not need to be submitted to a Research Ethics Committee.
ResultsIn the period from 2015 to 2019, 1,110 cases of MC were reported in Rondônia, representing 0.8% of the total 132,737 NV records. The prevalence in the state during this period was 8.36 per thousand NV, compared to the national prevalence of 8.74 cases per thousand NV. It was observed that the lowest prevalence was recorded in 2015, with 7.55 cases per thousand NV, while the highest prevalence was observed in 2016, with 9.14 cases per thousand NV. In 2017, the prevalence was 8.21 cases per thousand NV, followed by 8.87 cases per thousand NV in 2018 and 8.06 cases per thousand NV in 2019.
The Madeira-Mamoré region, composed of five municipalities, including the state capital, Porto Velho, had the highest prevalence of MC, with 10.34 cases per thousand NV. This prevalence was higher than the other health regions of the state and also the national average. In 2015, 88 occurrences were recorded in this region, followed by 114 in 2016, 102 in 2017 and 2018, and 98 in 2019. The second highest prevalence was found in the Vale do Jamari region, with 8.61 cases per thousand NV, while the Café region had the lowest prevalence, with 5.54 MC cases per thousand NV. Table 1 presents the prevalences by Health Regions.

Among the variables that define the maternal profile, a higher prevalence of MC was observed in babies born to mothers aged over 35 years, with low education (up to seven years), and widows and single mothers. In the obstetric profile of mothers, it was possible to identify a higher prevalence in multigender women (8.94 cases per thousand NB), with three children or more (9.50 cases per thousand NB), and with premature NBs (21.35 cases per thousand NB), coming from multiple gestations, a cesarean delivery (9.08 cases per thousand NB) and no prenatal consultation (12.82 cases per thousand NB).
The prevalence of MC was also higher among RNs with low birth weight (≤ 2,500g) and those with Apgar scores less than seven at the 1
st and 5
th minute (42.92 and 106.96 cases per thousand NV, respectively), (Table 2).
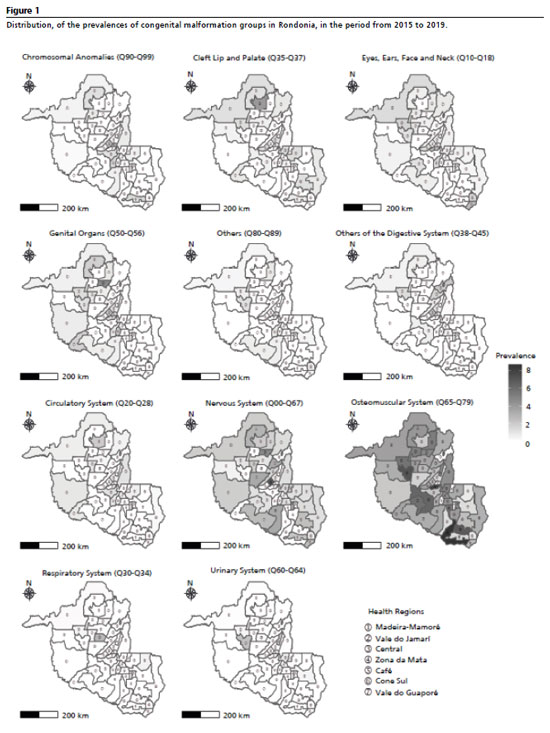
As for the groups found, of the 1,110 live births with CM in the state, 194 presented more than one malformation. The most prevalent group was CM of the osteomuscular system, with a prevalence of 3.47 cases per thousand NB, followed by CM of the nervous system, with 1.41 cases per thousand NB, and of the eye, ear, face, and neck with 0.79 cases per thousand NB. This distribution was also observed in the Madeira Mamoré and Vale do Jamari regions.
In the Café and Cone Sul regions, besides the CMs of the osteomuscular system and nervous system, cleft lip, and palate CMs were the most frequent. In the Vale do Guaporé and Zona da Mata regions, the third most prevalent group was the genital CMs. CMs of the circulatory system and chromosomal CMs shared third place among the most frequent in the Central region (Figure 1).
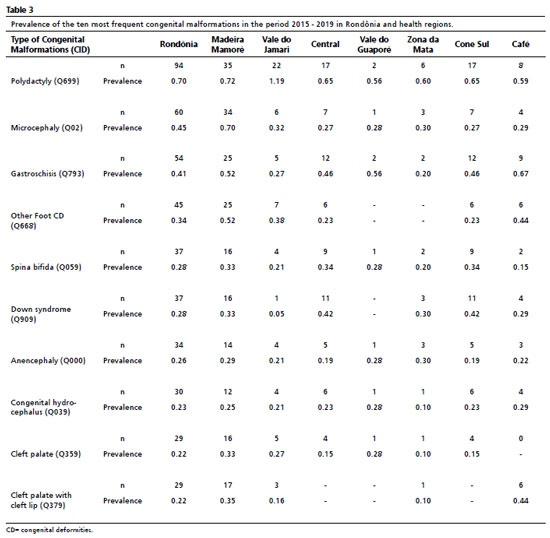
Among the ten most common CM in Rondônia, the diagnoses with the highest number of records were related to the osteomuscular system, including polydactyly, gastroschisis, and other congenital foot deformities. Of the 60 CM records from the nervous system, the most common diagnosis was microcephaly, followed by spina bifida, anencephaly, and hydrocephalus (Table 3).
DiscussionIn the present study, it was observed that the prevalence of CM in Rondônia, during the period from 2015 to 2019, was similar to the national average, but with significant variations among the health regions of the state.
The northern regions of Rondônia, such as Madeira Mamoré, had a higher prevalence of CM, while the southern regions, such as Café, had a lower prevalence. These disparities can be attributed to variations in case detection, due to more active and structured surveillance, and socioeconomic differences between regions.
The Madeira Mamoré region, where the capital Porto Velho is located, plays a key role in the provision of health services, especially in the care of high-risk deliveries, being a reference for several thematic networks of health care. Besides serving the local population, this region also receives patients from inland municipalities and neighboring states, expanding its influence in health care.
11This study identified a greater strength of association of CM among mothers with lower educational levels, as well as those who had no or less than six prenatal consultations, corroborating other studies.
7,12 Although the number of prenatal consultations showed an association with CM in the bivariate analysis, this association cannot be confirmed in the multivariate analysis.
Low education, in general, is related to unfavorable socioeconomic conditions, more difficult access to health services, greater likelihood of exposure to nutritional deficiencies, and less understanding of the importance of preventive measures during prenatal care, including the proper use of medications and awareness of the risks of gestational diseases. These factors may contribute to the increase in cases of CM.
13,14Studies report that adherence to prenatal care is related to the level of maternal education.
15 Higher maternal education may be associated with a better socioeconomic status, which favors the understanding of the importance of health care and awareness about regular participation in prenatal appointments. This leads to greater prevention and early detection of maternal conditions that may contribute to the development of CM.
12,16Although the present study found a higher prevalence of CM among single mothers, other studies conducted in Brazil have not observed an association between the types of malformations and marital status.
16,17Similar to other studies,
14,18 a relationship was observed between twin pregnancy and CM, compared to single pregnancies. This relationship can be partially explained by errors in cell divisions (genetic factors), the presence of chromosomal defects, intrauterine environmental factors, and possible constriction of the amniotic sac or umbilical cord.
19The association between CM and cesarean delivery observed in this study can be explained by the high correlation between these variables, since this procedure is usually indicated by doctors in pregnancies diagnosed with CM, due to the greater possibility of complications during delivery and the need for care support for the NB.
12,20Regarding the characteristics of the newborn, an association between CM and preterm births of less than 36 weeks was observed. In Brazil, prematurity is the leading cause of neonatal mortality, followed by CM.
21 Several maternal and neonatal variables, including pre-pregnancy maternal habits and pathologies, can influence prematurity and CM. Therefore, prematurity can be a consequence of the presence of CM, aggravating the pathology and increasing the risk in cases of multiple diagnoses.
19In this study, we observed a higher prevalence of unsatisfactory scores in the Apgar test at the 1st and 5th minute, indicating a higher risk at birth for babies with CM.In this study, we observed a higher prevalence of unsatisfactory scores in the Apgar test at the 1st and 5th minute, indicating a higher risk at birth for babies with CM.
22 These findings are consistent with other research
15,16,17,22,23 that also found an association between malformations, low birth weight, and Apgar scores.
Notifications of CM in Rondônia follow a similar pattern to the country, with CM of the osteomuscular system being the most common, due to the ease of identification during prenatal care and at birth.
14 As of 2015, there has been increased attention to records of CM of the nervous system due to the Zika virus epidemic,
24,25 which also affected Rondônia in 2016. Pregestational and gestational diabetes mellitus, along with folic acid deficiency, are known risk factors for central nervous system CM, highlighting the importance of prenatal care in the prevention and treatment of these conditions.
26Furthermore, some health regions showed an expressive prevalence of malformations related to the circulatory system, chromosomal, genital organs, and cleft lip and palate. These associations may be related to genetic, environmental, and other unknown factors, and deserve further investigation in the future.
Since the 1970s, farming has become the engine of growth in Rondônia, driving the intensive use of pesticides, which are recognized as risk factors for human health, including teratogenic effects.
27 Pesticides can cause malformations in different body systems, such as cardiovascular, genitourinary, osteomuscular, chromosomal, and gastrointestinal, as well as cleft lip and palate, and hip deformities.
27,28During the period of the present study, the commercialization of pesticides in Rondônia was alarming, reaching an average of 9,199 tons. This positions the state as one of the main consumers of pesticides in the country and the leader in the northern region in terms of marketed quantity. These data underscore the concern with the impact of these products on health and the environment.
29Despite being the main source of data on maternal and child health in Brazil, Sinasc has limitations, such as the low sensitivity regarding CM information, which results in underreporting and compromises the quality of the data. Problems such as lack of clarity in the forms, absence of precise definitions, absence of specific information in the statements, quality of training of professionals, and the insertion of late diagnoses of CM are factors that hinder data collection and must be addressed to improve data collection and improve the accuracy of the information available.
13,16,30 These issues must be addressed to improve the registration and monitoring system.
Despite the limitations presented, the present study achieved its objective by determining and characterizing the prevalence of CM in Rondônia. The prevalence in the state was similar to the national average but with significant variations among health regions. A higher prevalence was observed in the Madeira Mamoré Region, especially among mothers over 35 years of age, with a low level of education, and single mothers. There was also an association with premature births, low birth weight, and low Apgar scores in newborns.
22 These findings are consistent with other research
15,16,17,22,23 that also found an association between malformations, low birth weight, and Apgar scores.
Notifications of CM in Rondônia follow a similar pattern to the country, with CM of the osteomuscular system being the most common, due to the ease of identification during prenatal care and at birth.
14 As of 2015, there has been increased attention to records of CM of the nervous system due to the Zika virus epidemic,
24,25 which also affected Rondônia in 2016. Pregestational and gestational diabetes mellitus, along with folic acid deficiency, are known risk factors for central nervous system CM, highlighting the importance of prenatal care in the prevention and treatment of these conditions.
26Furthermore, some health regions showed an expressive prevalence of malformations related to the circulatory system, chromosomal, genital organs, and cleft lip and palate. These associations may be related to genetic, environmental, and other unknown factors, and deserve further investigation in the future.
Since the 1970s, farming has become the engine of growth in Rondônia, driving the intensive use of pesticides, which are recognized as risk factors for human health, including teratogenic effects.
27 Pesticides can cause malformations in different body systems, such as cardiovascular, genitourinary, osteomuscular, chromosomal, and gastrointestinal, as well as cleft lip and palate, and hip deformities.
27,28During the period of the present study, the commercialization of pesticides in Rondônia was alarming, reaching an average of 9,199 tons. This positions the state as one of the main consumers of pesticides in the country and the leader in the northern region in terms of marketed quantity. These data underscore the concern with the impact of these products on health and the environment.
29Despite being the main source of data on maternal and child health in Brazil, Sinasc has limitations, such as the low sensitivity regarding CM information, which results in underreporting and compromises the quality of the data. Problems such as lack of clarity in the forms, absence of precise definitions, absence of specific information in the statements, quality of training of professionals, and the insertion of late diagnoses of CM are factors that hinder data collection and must be addressed to improve data collection and improve the accuracy of the information available.
13,16,30 These issues must be addressed to improve the registration and monitoring system.
Despite the limitations presented, the present study achieved its objective by determining and characterizing the prevalence of CM in Rondônia. The prevalence in the state was similar to the national average but with significant variations among health regions. A higher prevalence was observed in the Madeira Mamoré Region, especially among mothers over 35 years of age, with a low level of education, and single mothers. There was also an association with premature births, low birth weight, and low Apgar scores in newborns.
These results highlight the importance of surveillance and monitoring of CMs, as well as the implementation of preventive measures and proper care during pregnancy. The early identification of risk factors and the provision of adequate support to pregnant women can contribute to reducing the occurrence of CMs and to the better management of diagnosed cases. In addition, the study highlights the need for investments in education and maternal and child health, especially in regions with a higher prevalence of CMs.
It is recommended to expand the study to a more comprehensive analysis of maternal-fetal risk factors, including genetic, environmental, and infectious aspects. This will allow the identification of effective prevention and intervention measures to reduce the incidence of CM in Rondônia. In addition, it is important to consider long-term follow-up of CM cases to assess the impact of these conditions on the health and development of affected children, providing crucial information to address their healthcare needs and specific interventions.
Finally, it is of utmost importance to share the results of the study with health professionals, public managers, and others involved in maternal and child health. The dissemination of scientific knowledge will be fundamental to support decisions in the creation and implementation of health policies directed to the prevention and treatment of CM in Rondônia.
References1. European Surveillance of Congenital Anomalies (EUROCAT). European Platform on Rare Disease Registration. [Internet]. 2021 [access in 2021 Out 21]. Available from:
https://eu-rd-platform.jrc.ec.europa.eu2. Mendes IC, Jesuino RSA, Pinheiro DS, Rebelo ACS. Congenital anomalies and its main avoidable causes: a review. Rev Med Minas Gerais. 2018; 28: e-1977.
3. Figueroa L, Garces A, Hambidge KM, CMClure EM, Moore J, Goldenberg R, et al. Prevalence of clinically-evident congenital anomalies in the Western highlands of Guatemala. Reprod Health. 2020 Nov; 17 (Supl. 2): 153.
4. World Health Organization (WHO). WHO methods and data sources for the global burden of disease estimates - 2000-2019. Geneva: WHO; 2020. [access in 2021 Nov 27]. Available from:
https://cdn.who.int/media/docs/default-source/gho-documents/global-health-estimates/ghe2019_daly-methods.pdf?sfvrsn=31b25009_75. Toufaily MH, Westgate M-N, Lin AE, Holmes LB. Causes of Congenital Malformations. Birth Defects Res. 2018 Jan; 110 (2): 87-91.
6. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Análise Epidemiológca e Vigilância de Doenças Não Transmissíveis. Declaração de Nascido Vivo: manual de instruções para preenchimento. [Internet]. Brasília (DF): Ministério da Saúde; 2022. 4th ed. [access in 2021 Nov 27]. Available from:
http://bvsms.saude.gov.br/bvs/publicacoes/declaracao_nascido_vivo_manual_4ed.pdf7. Ávila ALA, Mendonça Jr JF, Motta LHR, Nascente Jr REP, Silva TA, Guerra HS. Perfil epidemiológico das puérperas e nascidos vivos no estado de Goiás. Rev Educ Saúde. 2019; 7 (1): 90-9.
8. Instituto Brasileiro de Geografia e Estatística (IBGE). População estimada: IBGE, Diretoria de Pesquisas, Coordenação de População e Indicadores Sociais, Estimativas da população residente com data de referência 1 de julho de 2018. [Internet]. 2019. [access in 2021 Nov 27]. Available from:
https://cidades.ibge.gov.br/brasil/ro/panorama9. Santos L. Região de saúde e suas redes de atenção: modelo organizativo-sistêmico do SUS. Ciênc Saúde Colet. 2017; 22 (4): 1281-9.
10. Szumilas M. Explaining Odds Ratios. J Can Acad Child Adolesc Psychiatry. 2010 Aug; 19 (3): 227-9.
11. Vanassi BM, Parma GC, Magalhaes VS, Santos ACC, Iser BPM. Congenital anomalies in Santa Catarina: case distribution and trends in 2010-2018. Rev Paul Pediatr. 2022; 40: e2020331.
12. Reis AT, Santos RS, Mendes TAR. Prevalência de malformações congênitas no município do Rio de Janeiro, Brasil, entre 2000 e 2006. Rev Enferm UERJ. 19 (3): 364-8.
13. Forci K, Alami MH, Bouaiti E, Slaoui M, MdaghriAlaoui A, ThimouIzgua A. Prevalence of congenital malformations at the "les Orangers" maternity and reproductive health Hospital of Rabat: descriptive study of 470 anomalies. BCM Pediatr. 2020 Jun; 20 (1): 272.
14. Cosme HW, Lima LS, Barbosa LG. Prevalência de anomalias congênitas e fatores associados em recém-nascidos do município de São Paulo no período de 2010 a 2014. Rev Paul Pediatr. 2017; 35 (1): 33-8.
15. Rodrigues RPGTO, Santos AAP, Santos WB, Santos JAM, Oliveira JCS, Teixeira LM, et al. Perfil das malformações congênitas em um estado do nordeste brasileiro. Res Soc Dev. 2020; 9 (12): e40491211298.
16. Luz GS, Karam SM, Dumith SC. Anomalias congênitas no estado do Rio Grande do Sul: análise de série temporal. Rev Bras Epidemiol. 2019; 22: e190040.
17. Fontoura FC, Cardoso MVLML. Association between congenital malformation and neonatal and maternal variables in neonatal units of a Northeast Brazilian city. Texto Contexto Enferm. 2014; 23 (4): 907-14.
18. Brizot ML, Fujita MM, Reis NSV, Banduki Neto JD, Regina S, Miyadahira S, et al. Malformações Fetais em Gestação Múltipla. Rev Bras Ginecol Obstetr. 2000; 22 (8): 511-7.
19. Harris BS, Bishop KC, Kemeny HR, Walker JS, Rhee E, Kuller JA. Risk Factors for Birth Defects. Obstet Gynecol Surv. 2017 Feb; 72 (2): 123-35.
20. Costa TS, Silva MSO, Souza AES, Carvalho ACS, Paiva CEA, Santos KT, et al. Perfil epidemiológico das malformações congênitas do sistema nervoso central no estado do Pará, Brasil. Braz J Health Rev. 2021; 4 (1): 2765-76.
21. França EB, Lansky S, Rego MAS, Malta DC, França JS, Teixeira R, et al. Principais causas da mortalidade na infância no Brasil, em 1990 e 2015: estimativas do estudo de Carga Global de Doença. Rev Bras Epidemiol. 2017; 20 (Suppl. 1): 46-60.
22. Freitas LCS, Nunes AA, Meneguci J, Nascimento Neto GC, Castro SS. Association of congenital anomalies in live births with their obstetric-neonatal and sociodemographic profiles. Texto Contexto Enferm. 2021; 30: e20200256.
23. Gonçalves MKS, Cardoso MD, Lima RAF, Oliveira CM, Bonfim CV. Prevalência e fatores associados às malformações congênitas em nascidos vivos. Acta Paul Enferm. 2021; 34: eAPE00852.
24. Marinho F, Araújo VEM, Porto DL, Ferreira HL, Coelho MRS, Lecca RCR, et al. Microcefalia no Brasil: prevalência e caracterização dos casos a partir do Sistema de Informações sobre Nascidos Vivos (Sinasc), 2000-2015. Epidemiol Serv Saúde. 2016; 25 (4): 701-12.
25. Reis LC, Barbian MH, Cardoso-dos-Santos AC, Silva EVL, Boquett JA, Schuler-Faccini L. Prevalence of congenital anomalies at birth among live births in the state of Maranhão from 2001 to 2016: temporal and spatial analysis. Rev Bras Epidemiol. 2021; 24 (Suppl. 1): e210020.
26. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Boletim Epidemiológico No 06. Anomalias congênitas no Brasil, 2010 a 2019: análise de um grupo prioritário para a vigilância ao nascimento. Brasília (DF); 2021. (Volume 52). [access in 2022 Jul 20]. Available from:
https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/edicoes/2021/boletim_epidemiologico_svs_6_anomalias.pdf27. Nascimento B, Silva R, Ferreira A, Silva E, Junior J, Dias L, et al. Impacto ambiental sobre a saúde humana devido à exposição aos agrotóxicos. UNICIÊNCIAS. 2021; 25 (1): 44-56.
28. Dutra LS, Ferreira AP. Associação entre malformações congênitas e a utilização de agrotóxicos em monoculturas no Paraná, Brasil. Saúde Debate. 2017; 41 (Spe 2): 241-53.
29. Franco TF, Parmejiani RS, Cunha MPL, Miranda A, Marques RC, Guimarães JRD. Characterization and distribution of pesticide use from 2015 to 2019, by health regions in the state of Rondônia (RO), Amazon, Brazil. Rev Bras Ciênc Ambient. 2021; 56 (3): 445-58.
30. Luquetti DV, Koifman RJ. Qualidade da notificação de anomalias congênitas pelo Sistema de Informações sobre Nascidos Vivos (Sinasc): estudo comparativo nos anos 2004 e 2007. Cad Saúde Pública. 2010; 26 (9): 1756-65.
Received on September 13, 2022
Final version presented on June 5, 2023
Approved on June 7, 2023
Associated Editor: Lygia Vanderlei
Acknowledgments: We thank the Council for Scientific and Technological Development (CNPq) for the financial support (Process nº 424808/2018-8 and scholarship for TFF) and the professionals of the Unified Health System (SUS) and the Ministry of Health for contributing to the realization of this work.
Authors' contribution: Franco TF: study conception and design, data analysis and interpretation, manuscript writing and editing; Marques RC and Buralli RJ: study conception and design, and manuscript revision; Miranda A: study conception and design, data analysis and interpretation, manuscript revision; Dórea JG: study conception and design, and review of the manuscript; Cunha MPL: study conception and design, acquisition of funding, project, and resource management, and review of the manuscript; Guimarães JRD: study conception and design, acquisition of funding, project, and resource management, supervision, and the writing and editing of the manuscript.
All authors approved the final version of the article and declare no conflict of interest.


 ; Rejane Corrêa Marques2
; Rejane Corrêa Marques2






 Ler em português
Ler em português