ABSTRACT
OBJECTIVES: to evaluate the success rate of labor induction and determinants of successful outcome.
METHODS: retrospective cohort study of parturients that undergone labor induction between 2006 and 2015. Data was retrieved from the medical records and multivariate logistic regression was used to evaluate the determinants of successful labor induction.
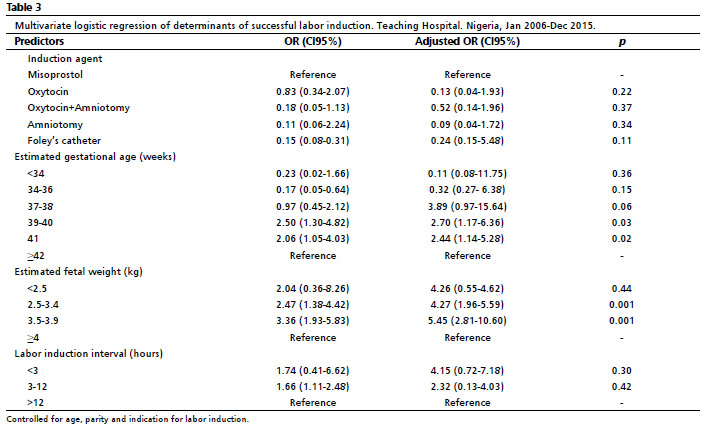
RESULTS: the rate of labor induction was 10.9%. Out of the 940 women analysed, six hundred and fifty-six women (69.8%) had successful vaginal delivery. Labor induction at 39-40 weeks (OR=2.70; CI95%=1.17-6.36), 41 weeks (OR=2.44; CI95%=1.14-5.28), estimated fetal weight between 2.5 and 3.4kg (OR=4.27, CI95%=1.96-5.59) and estimated fetal weight of 3.5-3.9kg (OR=5.45; CI95%=2.81-10.60) increased the odds of achieving vaginal delivery.
CONCLUSIONS: our findings suggest that 39, 40 and 41 weeks are optimal gestational ages for labor induction with respect to successful vaginal delivery. Also, estimated fetal weight between 2.5kg and 3.9kg favours successful vaginal delivery.
Keywords:
Cesarean section, Gestational age, Labor induction, Vaginal delivery
RESUMO
OBJETIVOS: avaliar a taxa de sucesso da indução do trabalho de parto e determinantes de um resultado bem sucedido.
MÉTODOS: estudo de coorte retrospectivo de parturientes que submeteram a indução de trabalho de parto entre 2006 e 2015. Os dados foram recuperados dos registros médicos e a regressão logística multivariada foi utilizada para avaliar os determinantes da indução de trabalho de parto bem sucedida.
RESULTADOS: a taxa de indução de trabalho de parto foi de 10,9%. Das 940 mulheres analisadas, seiscentas e cinquenta e seis mulheres (69,8%) tiveram um parto vaginal bem sucedido. A indução de trabalho de parto nas 39-40 semanas (OR=2,70; IC95%=1,17-6,36), 41 semanas (OR=2,44; IC95%=1,14-5,28), peso fetal estimado entre 2,5 e 3,4kg OR=4,27; IC95%=1,96-5,59) e peso fetal estimado entre 3,5-3,9kg (OR=5,45; IC95%=2,81-10,60) aumentou as probabilidades de conseguir um parto vaginal.
CONCLUSÃO: as nossas conclusões sugerem que as 39, 40 e 41 semanas são idades gestacionais ideais para a indução do trabalho de parto no que diz respeito ao sucesso do parto vaginal. Além disso, o peso fetal estimado entre 2,5kg e 3,9kg favorece o parto vaginal bem sucedido.
Palavras-chave:
Parto cesáreo, Idade gestacional, Indução do trabalho de parto, Parto vaginal
IntroductionLabor induction is a common obstetric procedure that is widely carried out all over the world in cases where continuation of pregnancy is hazardous to either mother; baby or both.
1,2 Labor induction can be defined as any procedure that stimulates uterine contractions before labor begins spontaneously.
3 The decision to induce labor is usually made when its benefits outweigh the risks.
2,4,5 Labor induction could be life-saving for both mother and baby; improving maternal and perinatal outcomes.
6-8 In fact, labor induction was found to reduce perinatal deaths by 66% in Africa.
6 Some researchers highlighted the criticisms that greeted labor induction in the early years.
5Elective labor induction was even described as "meddlesome obstetrics" by some Obstetricians.
9 The major concerns were precipitate labor, postpartum hemorrhage, cervical lacerations and birth asphyxia.
5 It however continued to gain acceptance despite the objections from leading Obstetricians. This acceptance was due to reports from case series and matched case control studies that showed that the benefits outweigh the risks in selected patients.
5,10 The labor induction rate has been on the increase since then. The labor induction rates vary worldwide. According to World Health Organization (WHO) Global survey on Maternal and Perinatal Health, which included 373 healthcare facilities in 24 countries and nearly 300, 000 deliveries, 9.6% of the deliveries involved labor induction.
1 The induction rate was the lowest in Niger (1.4%) and the highest in Sri Lanka (35.5%).
1 In Nigeria, Lawani
et al. ,
10 reported induction rate of 11.5%.
Indications for labor induction include post-dated pregnancy, premature rupture of membranes, intrauterine growth restriction and rhesus isoimmunisation.
9-12 Maternal conditions like diabetes mellitus, hypertensive disorders of pregnancy, and renal disease can also create a need for labor induction.
4,10-12 Several methods are available for labor induction .
6 These include amniotomy, oxytocin, prostaglandins and mechanical methods such as sweeping of membrane.
11-14 Prior assessment of the cervix is necessary to determine the favorability of the cervix for labor induction.
15 This is usually done with the aid of Bishop score.
15,16However, labor induction is not without complications; these include uterine hyperstimulation, fetal distress, intrapartum fetal death, uterine rupture, genital tract lacerations, postpartum hemorrhage, etc.
14 Many parturients are usually concerned whenever labor induction is being discussed as the preferred mode of delivery. Their concerns usually ranged from prolonged labor, dystocia, fetal distress, intrapartum fetal demise and eventual cesarean section due to failed labor induction. It is therefore necessary to audit the practice of labor induction in this center in order to know the success rates and its determinants. These factors can be used to predict success; and ultimately improve patient selection process for labor induction. We aimed to evaluate the success rate of labor induction and determinants of successful outcome in a teaching hospital in Nigeria.
MethodsThis was a retrospective cohort study of parturients who undergone cervical ripening and labor induction at the Department of Obstetrics and Gynecology at a teaching hospital in Nigeria between January 2006 and December 2015. This hospital serves as a referral center for patients in three states in Nigeria. The hospital is located in a semi-urban area of the state. Parturients scheduled for labor induction was usually assessed for cervical ripening before labor induction. The departmental protocol for labor induction involved prior cervical ripening before labor induction if the Bishop score is less than 6. The methods of cervical ripening prior to labor induction were transcervical extra amniotic passage of Foley catheter (Agary Catheters,Yangzhou, Jiangsu, China) and passage of vaginal misoprostol. (CytotecR Pfizer, Division of Pfizer Inc, NY, USA) Labor induction is routinely commenced when Bishop Score is greater than 6. Some parturients progressed into labor spontaneously after cervical ripening while some did require amniotomy, oxytocin or both for labor induction. Amniotomy is the preferred option for labor induction after successful cervical ripening. Oxytocin may be added if required to augment uterine contractions. Oxytocin may be used alone if there are contraindications to amniotomy e.g intrauterine fetal death and retroviral infection.
Inclusion criteria were parturients with singleton cephalic pregnancy, fetal biophysical profile of 8 or 10 with reactive cardiotocograph and no previous cesarean section who underwent labor induction for medical reasons after the age of viability; which is 28weeks of pregnancy in Nigeria. Exclusion criteria were previous cesarean section at any gestational age, fetal abnormalities, uterine fibroid, placenta previa, placenta abruption, chorioamnionitis, previous myomectomy or any uterine surgery, amniotic fluid index less than 7, multiple gestation and incomplete medical records. All participants were identified through labor ward and delivery records. The written medical records were retrieved from the Department of Health Information Management and a study proforma was used to extract the relevant data. Data retrieved include age, parity, schooling, indication for labor induction, method of labor induction, duration of labor, complications, Apgar score, and birth weight. The primary outcome measure was successful vaginal delivery. Data was analyzed with Statistical Package for Social Sciences version 23 by IBM Incorporated, NY. , USA. Continuous variables were summarized with means and standard deviation while categorical variables were summarised with frequency and percentages. Chi-square was used for bivariate analysis of associated factors with labor induction. Multivariate logistic regression was used to predict the determinants of successful vaginal delivery. A logistic regression model was used to control for confounding factors. Model for fit for the model was assessed with the Hosmer-Lemeshow test. All tests were two tailed and
p<0.05 was taken as statistically significant.
Ethical clearance for this study was obtained from the Ethics and Research Committee of the hospital (Protocol Number ERC/2013/09/05).
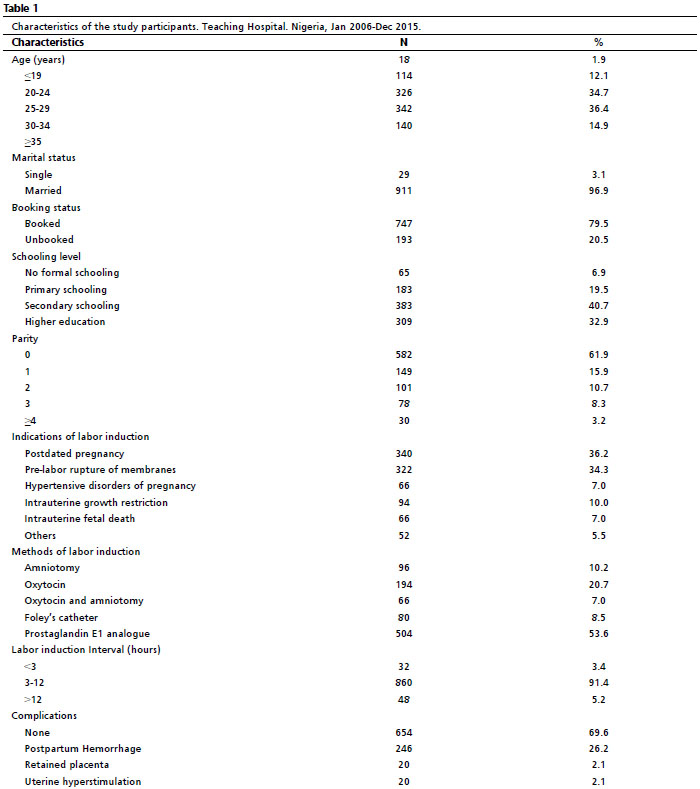
ResultsDuring the study period, there were 10,012 deliveries, 1,090 (10.9%) had labor induction. Data for 940 women were complete and available for review; and therefore, included in analysis. (Figure 1) The mean age of the participants was 30.24±4.5 years. Majority of the women were married and received antenatal care in our center (booked) (Table 1). The mean parity was 0.80±1.31. Majority of the participants were nulliparous (Table 1). The common indications for labor induction were post-dated pregnancy, pre-labor rupture of membranes, hypertensive disorders of pregnancy, intrauterine growth restriction and intrauterine fetal death (Table 1). More than half of the participants progressed to spontaneous labor after cervical ripening while the remaining had amniotomy (10.2%), oxytocin (20.7%), or oxytocin with amniotomy (7%). The mean of labor induction interval was 10.45±6.22 hours. Most of the women delivered between 3- 12 hours of commencement of labor induction (91.4%). Vaginal delivery was achieved in 656 (69.8%) parturients while 284 (30.2%) had emergency cesarean section. The main indications for cesarean section were cephalopelvic disproportion (62.5%), fetal distress (24.8%), and cord prolapse (2.8%). The mean birth weight was 3.12±0.77kg. Most babies had good Apgar score (Apgar score ≥ 7) at 1
st minute (749, 79.7%) and 5
th minute (836, 88.9%). Thirteen babies (1.4%) were severely asphyxiated and there were 4 (0.4%) intrapartum fetal deaths. Primary postpartum hemorrhage was the major complication reported in 26.2%. There was no maternal mortality.
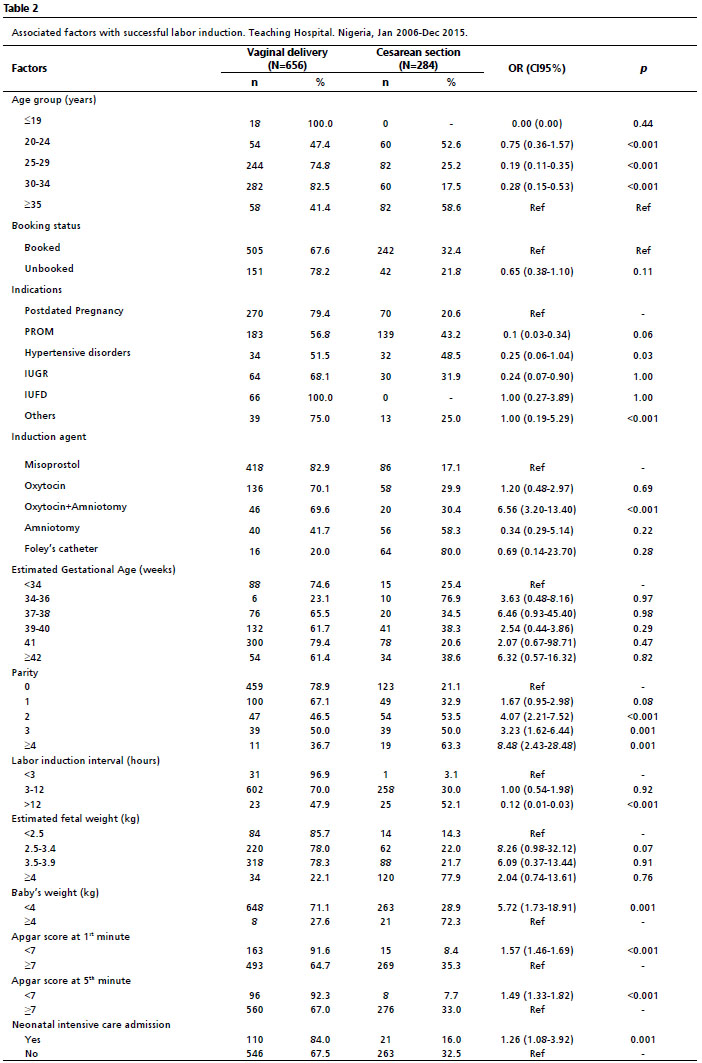
There were significant associations between the outcomes of labor induction and socio-demographic characteristics (Table 2). Women older than 19 years old were less likely to achieve vaginal delivery compared with those younger than 19 years of age, although it was not statistically significant (Table 2). In addition, women aged 24 to 34 years were less likely to achieve vaginal delivery compared to women older than 35 years (Table 2). Unbooked patients were also less likely to achieve vaginal delivery compared with booked patients though the association was not statistically significant (OR=0.65; CI95%=0.38-1.10;
p=0.11). Use of oxytocin+amniotomy increased the probability of achieving vaginal delivery in this cohort (OR=5.56; CI95%=3.20-13.40,
p<0.001) (Table 2).
After controlling for age, parity and indication for labor induction with a multivariate logistic regression model, the odds of achieving vaginal delivery with labor induction was doubled at weeks 39-40 (adjusted OR=2.70; CI95%=1.17-6.36) and weeks 41 (adjusted OR=2.44; CI95%=1.14-5.28) when compared with labor induction at 42weeks of pregnancy. (Table 3) Also, the odds of achieving vaginal delivery with labor induction was increased at estimated fetal weight between 2.5 and 3.4 kg (adjusted OR=4.27; CI95%=1.96-5.59) and estimated fetal weight of 3.5-3.9kg (adjusted OR=5.45; CI95%=2.81-10.60) compared with estimated fetal weight of greater than or equal to 4kg. However, no induction agent could predict successful vaginal delivery (Table 3).
DiscussionThe labor induction rate in this study was comparable to induction rates in other parts of the country and Africa,
2,10 however, this rate was higher than 6.3% reported by Bukola
et al. 6 This could be attributed to the fact that this study was a review of practice at a referral center where high risk pregnancies are being managed which is in tandem with Bukola' s submission that induction rates were significantly higher at tertiary health facilities.
3,6, In developed countries with better facilities for intrapartum fetal monitoring, the labor induction rates are higher.
6,17,18 Also, the labor induction rate has been on upward trend, even in the developing nations. In 2002, Ekele
et al. 19 reported induction rate of 3% while several studies afterwards reported higher rates.
6,10 Increase in availability of intrapartum fetal monitoring devices like continuous electronic fetal monitoring could be responsible for this trend.
The commonest indication for labor induction in this study was comparable to other studies in Nigeria. Post-dated pregnancy was the commonest indication for labor induction as reported by other studies in Nigeria.
10,12 The high prevalence of post-dated pregnancy in this audit might be connected to unavailability of dating scan which would have assisted in dating the pregnancies as induction rates have been found to be higher when there was gestational error.
20 The proportion of women that had labor induction on account of intrauterine fetal death in this study was similar to the proportion documented by Bukola
et al. 6 Bukola
et al. 6 however moved on to affirm that some of these deaths could have been averted by timely recourse to labor induction . Misoprostol was the preferred agent for cervical ripening in this center and majority of these women progressed spontaneously into labor. Use of prostaglandin E1 analogue was however not a statistically significant determinant of labor induction outcome. This finding is similar to a previous study in this center by Owolabi
et al. 21 in which misoprostol was compared to Foley's catheter for cervical ripening and labor induction. Prostaglandins are now the commonest induction agents being used worldwide.
11 Misoprostol has been found to be safe and effective.
22,23The mean of labor induction interval was less than 12 hours which was also comparable to labor induction interval reported by Owolabi
et al. 21 The proportion of parturients that had vaginal delivery was comparable to 64.7% documented among nulliparous women who had labor induction in 2008.
24 It was however lower than 85% reported by Ibrahim
et al. 12 in another center in Nigeria. This difference might be attributed to differences in induction rates and probably patients' selection process. The commonest indication for cesarean section was cephalopelvic disproportion as reported in similar studies. The first and fifth minute Apgar score were comparable to other studies in which most babies had good Apgar score.
12,24 The four intrapartum deaths were due to delay in decision-incision interval for four women with fetal distress. Most women did not have complications; and the reported complications have been documented by previous studies.
10,12,25 An important fact to note is that these complications also occur in spontaneous labor.
24Labor induction at 39
th and 41
st weeks of pregnancy doubled successful labor induction outcome. This suggests that 39
th, 40
th and 41
st weeks are optimal gestational ages for labor induction with respect to successful vaginal delivery. Many existing evidences had shown that delivery before 41
st or 42
nd weeks of pregnancy leads to improved maternal and neonatal outcomes.
26,27 Nilcoson
et al. 26 estimated optimal gestational age for delivery to be between 38
th and 41
st weeks for different groups of women. However, there have been concerns about increased cesarean section rates associated with labor induction.
25,28,29 Therefore, further studies are necessary to compare the maternal and neonatal outcomes of labor induction with spontaneous labor at these gestational ages.
Similarly, estimated fetal weight of 2.5kg to 3.9 kg doubled the odds of achieving vaginal delivery. Macrosomia is known to predict failed labor induction as documented in other studies.
2,30 The strength of this study is that it is a comprehensive audit of the labor induction practice in this center; and it can be generalised for the tertiary obstetric care centers in Nigeria because their obstetric practices are comparable. The weakness lies in being a retrospective review; accompanied with missing data. Also, neonatal death was not captured in this review. In conclusion, labor induction is a safe obstetric intervention that should be offered to women when it is indicated especially in developing nations where there is still great aversion for abdominal delivery. Delays before surgical intervention should be reduced to the minimum in order to prevent avoidable perinatal deaths. Our findings suggest that 39, 40 and 41 weeks are optimal gestational ages for labor induction with respect to successful vaginal delivery. Future studies should compare maternal and fetal outcome of spontaneous labor with induced labor at 39, 40 and 41 weeks of pregnancy.
References1. World Health Organization (WHO). WHO recommendations for induction of labour. Geneva: WHO; 2011. [access in 2022 jan 10]. Available from:
http://whqlibdoc.who.int/publications/2011/9789241501156_eng.pdf.
2. Rade BK, Mitku YM, Weldemicheal AB, Zenebe ZM, Desalegn AY, Bitsu BD. Induction of labor and its determinant factors: retrospective cross-sectional study from a public hospital in Ethiopia. J Preg Child Health. 2018; 5 (5): 1000388.
3. Gattás DSMB, Amorim MMR, Feitosa FEL,
et al. Misoprostol administered sublingually at a dose of 12.5 μg versus vaginally at a dose of 25 μg for the induction of full-term labor: a randomized controlled trial protocol. Reprod Health. 2018; 15 (1): 65.
4. Ade-Ojo IP, Akintayo AA. Induction of labor in the developing countries- an overview. J Med Med Sci. 2013; 4 (7): 258-62.
5. Seijmonsbergen-Schermers AE, Scherjon S, Jonge A. Induction of labour should be offered to all women at term. BJOG. 2019; 126 (13): 1599.
6. Bukola F, Idi N, M'Mimunya M, Jean-Jose WM, Kidza M, Isilda N,
et al. Unmet need for induction of labor in Africa: secondary analysis from the 2004-2005 Global Maternal and Perinatal Health Survey (A cross-sectional survey). BMC Public Health. 2012; 12: 722.
7. Koopmans CM, Bijlenga D, Groen H, McVijgen S, Aarnoudse JG, Bekedam DJ,
et al. Induction of labor versus expectant monitoring for gestational hypertension or mild pre-eclampsia after 36 weeks' gestation (HYPITAT): a multicentre, open-label randomised controlled trial. Lancet. 2009 Sep; 374 (9694): 979-88.
8. Middleton P, Shepherd E, Morris J, Crowther CA, Gomersall JC. Induction of labour at or beyond 37 weeks' gestation. Cochrane Database Syst Rev. 2020 Jul; 7 (7): CD004945.
9. Badejoko O, Onwudiegwu U. Management of Normal and Abnormal Labour. In: Okonofua, F, Balogun JA, Odunsi K, Chilaka VN. (eds) Contemporary Obstetrics and Gynecology for Developing Countries. Berlim: Springer, Cham; 2021. p. 117-27.
10. Lawani OL, Onyebuchi KO, Iyoke CA, Okafo CN, Ajah LO. Obstetric Outcome and significance of labor induction in a Health Resource poor setting. Obstet Gynecol Int. 2014; 2014: 419621.
11. Coates D, Makris A, Catling C, Henry A, Scarf V, Watts N,
et al. A systematic scoping review of clinical indications for induction of labour. PLoS One. 2020 Jan; 15 (1): e0228196.
12. Ibrahim IA, Obilahi A, Ekine AA. The safety of induction of labor in the Niger Delta Region. Green J Med Sci. 2012; 2 (6): 173-8.
13. de Vaan MDt, Ten Eikelder MLg, Jozwiak M, Palmer KR, Davies-Tuck M, Bloemenkamp KWM,
et al. Mechanical methods for induction of labour. Cochrane Database Syst Rev. 2019 Oct; 10 (10): CD001233.
14. Ikeotuonye AC, Anikwe CC, Obuna JA, Okorochukwu BC, Ejikeme BN, Ifemelumna CC,
et al. Relationship between Bishop score and success of induction of labour in Federal Teaching Hospital, Abakaliki, Ebonyi State. Open J Obstet Gynaecol. 2018 Sep; 8 (11): 980-92.
15. Wormer KC, Bauer A, Williford AE. Bishop Score. [Updated 2021 Sep 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 .
16. Bishop EH. Pelvic scoring for elective induction. Obstet Gynaecol. 1964 Aug; 24: 266-8.
17. MacDorman MF, Matthews JF, Martin JA, Malloy MH. Trends and characteristics of induced labor in the United States, 1989-1998. Paediatr Perinat Epidemiol 2002 Jul; 16 (3): 263-73.
18. Danilak VA, Botti JJ, Roach JJ, Savitz DA, Muri JH, Caldwell DL. Changes in delivery methods at specialty care hospitals in the United States between 2006 and 2010. J Perinatol. 2013 Dec; 33 (12): 919-23.
19. Ekele BA, Oyetunji JA. Induction of labor at Usman Danfodio University Teaching Hospital, Sokoto. Trop J Obstet Gynaecol. 2002; 19 (2): 74-7.
20. Onyebuchi A, Okafor L, Mamah J, Obi V, Esike C, Umeora O,
et al. Management and Obsttric outcomes of Pst-date pregnancies in Abakaliki, Eonyi State, Southeast Nigeria: A cross-sectional study. Int J Women Health Reprod Sci. 2022; 10 (4): 1-4.
21. Owolabi AT, Kuti O, Ogunlola IO. Randomised trial of intravaginal prostaglandin E1 analogue and intracervical Foley's catheter for cervical ripening and induction of labor. J Obstet Gynaecol. 2005 Aug; 25 (6): 565-8.
22. Loto OM, Fadahunsi AA, Kolade CO. Safety and efficacy of prostaglandin E1 analogue for induction of labor in a semi urban hospital setting. J Obstet Gynaecol. 2004 Sep; 24 (6): 638-40.
23. Loto OM, Ikuomola AA, Ibrahim 6IA, Onwudiegwu U. Comparative study of the outcome of induction of labor using 25µg and 50µg of vaginal prostaglandin E1 analogue. J Matern Fetal Neonatal Med. 2012 Nov; 25 (11): 2359-62.
24. Orji EO, Olabode TO. Comparative study of labor progress and delivery outcome among induced versus spontaneous labor in nulliparous women using WHO modified parthograph. NJOG. 2008; 3 (1): 24-8.
25. Pevzner L, Rayburn WF, Rumney P, Wing DA. Factors predicting successful labor induction with dinoprostone and misoprostol vaginal inserts. Obstet Gynecol. 2009 Aug; 114 (2): 261-7.
26. Nicholson JM, Kellar LC, Kellar GM. The impact of interaction between increasing gestational age and obstetric risk on birth outcomes. J Perinatol. 2006; 26 (7): 392-402.
27. Caughey AB. What is the optimal gestational age for delivery? J Perinatol. 2006; 26 (7): 387-8.
28. Vahratian A, Zhang J, Troendle JF, Sciscione AC, Hoffman MK. Labor progression and risk of cesarean delivery in electively induced nulliparas. Obstet Gynecol. 2005 Apr; 105 (4): 698-704.
29. Hassan WN, Shallal F, Roomi AB. Prediction of successful Induction of labor using ultrasonic fetal parameters. Curr Women Health Rev. 2022; 18 (1): 134-9.
30. Moldéus K, Cheng YW, Wikström AK, Stephansson O. Induction of labor versus expectant management of large-for-gestational-age infants in nulliparous women. PLoS One 2017 Jul; 12 (7): e0180748.
Received on June 15, 2021
Final version presented on October 4, 2022
Approved on October 11, 2022
Associated Editor: Alex Sandro Souza
Authors’ contribution: Okunola TO: conceived the study, participated in its design and coordination of the study, data analysis and drafting the manuscript. Bola-Oyebamiji SB and Sowemimo O: in study design, data analysis and drafted the manuscript. Ajenifuja KO: study design, drafting of manuscript and supervision.
All authors approved the final version of the article and declare no conflicts of the interest.


 ; Sekinat Bolanle Bola-Oyebamiji2
; Sekinat Bolanle Bola-Oyebamiji2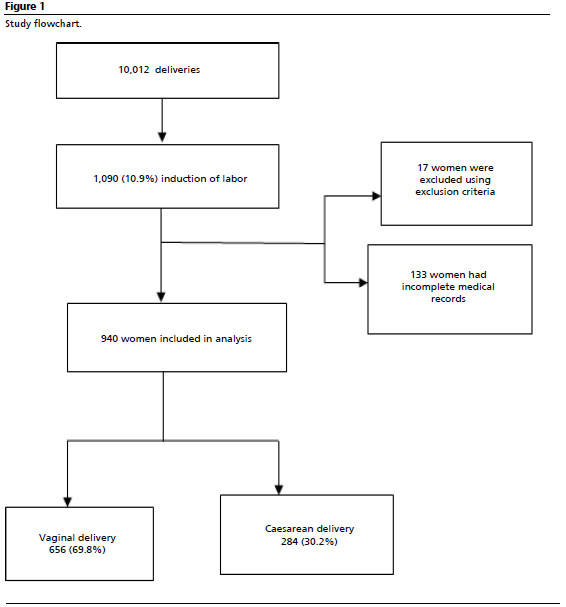






 Ler em português
Ler em português