ABSTRACT
OBJECTIVES: to characterize the profile of pregnant women and newborns accompanied at a reference center for infectious-parasitic diseases, after the exposure of T. gondii, establishing comparisons with a previous study, in the same location, ten years ago.
METHODS: this is a retrospective cohort study, with a follow-up of four years (2016 to 2019), using the previous study carried out from 2002 to 2010 as a comparative for the variables assessed. Mothers who presented tests suggestive of seroconversion for the disease during prenatal care and their respective concepts, followed up over a year, were included. The chi-square test was used, assuming a significance level of 5% for the comparison of the groups in the two periods.
RESULTS: during the period from 2016 to 2019, 79 binomials were studied, whereas 58 binomials were accompanied in the previous period. Comparing both periods, the findings showed lower proportions of adolescents (p<0.001), with low schooling (p<0.001), with low serological testing (p<0.001) and with late or postnatal diagnosis (p<0.001). As to the children, the findings showed fewer changes in fundoscopy (p<0.001), strabismus (p=0.002), hepatomegaly (p=0.026) and any sequelae (p<0.001).
CONCLUSION: a positive advance was observed regarding the care provided for the mother-child binomial affected by T. gondii, with a reduction in negative outcomes for the child. However, there are still challenges concerning the diagnosis and proper management of the disease.
Keywords:
Vertical transmission of infectious diseases, Toxoplasmosis, Congenital toxoplasmosis, Prenatal care
RESUMO
OBJETIVOS: caracterizar o perfil de gestantes e neonatos acompanhadas em um centro de referência em doenças infecto-parasitárias, após exposição ao Toxoplasma gondii, estabelecendo comparações em relação a estudo prévio, no mesmo local, há dez anos.
MÉTODOS: trata-se de estudo de coorte retrospectivo, com seguimento de quatro anos (2016 a 2019), servindo o estudo prévio realizado de 2002 a 2010 como comparativo para as variáveis estudadas. Foram incluídas mães que apresentaram durante o pré-natal exames sugestivos soroconversão para a doença e seus respectivos conceptos, acompanhados ao longo de um ano. Utilizou-se o teste qui-quadrado, assumindo-se nível de significância de 5% para a comparação dos grupos nos dois períodos.
RESULTADOS: durante o período de 2016 a 2019, foram estudados 79 binômios, enquanto no período anterior foram acompanhados 58 binômios. Comparando-se os dois períodos, em relação às mães, registraram-se menores proporções de adolescentes (p<0,001), de baixa escolaridade (p<0,001), baixa realização de testes sorológicos (p<0,001) e com diagnóstico tardio ou pós-natal (p<0,001). Em relação às crianças, verificaram-se menores proporções de alterações de fundoscopia (p<0,001), estrabismo (p=0,002), hepatomegalia (p=0,026) e qualquer sequela (p<0,001).
CONCLUSÃO: observou-se um avanço em relação aos cuidados para o binômio mãe-filho acometido pelo T. gondii, com redução de desfechos negativos sobre a criança. Todavia, ainda existem desafios para o diagnóstico e adequado manejo da doença.
Palavras-chave:
Transmissão vertical de doenças infecciosas, Toxoplasmose, Toxoplasmose congênita, Assistência pré-natal
IntroductionToxoplasmosis is considered a neglected disease and still represents a major challenge for healthcare services and professionals.
1,2 Gestational and congenital Toxoplasmosis have been in the list of compulsory notifiable diseases in Brazil since February 2016.
2 The disease becomes relevant when affecting pregnant women owing to the risk of vertical transmission and fetal involvement with a broad spectrum of manifestations, ranging from asymptomatic or oligosymptomatic forms, subclinical lesions with subsequent reactivation and even severe and permanent lesions with special tropism for the organs of the nervous system.
3-5In recent years, scientific publications have highlighted how the quality of prenatal care, aiming at the early diagnosis and treatment of the disease, is crucial to the favorable outcome of pregnancy.
6,7 Additionally, neonatal screening measures, treatment and multidisciplinary follow-up of affected children, even in the absence of maternal treatment during pregnancy, have been associated with lower disease recurrence rates and fewer sequelae.
8There are gaps in literature as to the longitudinal behavior of gestational and congenital toxoplasmosis within the same region. A study was published in 2012 characterizing the profile of pregnant women and children treated at a reference center for Toxoplasmosis in the North State of Minas Gerais, during a period of eight years.
9 By returning to the indicators previously studied, a new scenario, or even nuances were not yet studied, could be revealed in view of the new knowledge acquired over time about the parasite, the behavior of the disease and the proper management of patients involved in this context, enabling new perspectives of approach.
The aim of this study was to evaluate the profile of pregnant women and neonates followed up at a reference center for infectious-parasitic diseases, after the exposure of
T. gondii, making comparison with a study previously conducted at the same location ten years ago.
MethodsThis is a study developed in two phases: in the first phase, a retrospective cohort study was conducted with a follow-up of four years (2016 to 2019); in the second phase, a comparative analysis of the variables studied was performed with a previous study conducted from 2002 to 2010, in the same place.
9 The study was conducted in the city of Montes Claros, in the North of Minas Gerais. With an estimated population of about 417,000 inhabitants, the city represents an important regional hub and its scope in health care reaches more than one hundred cities in the region. In 2012, the population was about 370,000 inhabitants with five general hospitals, seven polyclinics, 14 healthcare centers and 59 teams of the Family Health Strategies (FHS), with an average of 6000 births a year. In 2020, the city outpatient care was conducted in 4 polyclinics, 142 FHS units and 3 maternity hospitals, all of which are linked with the Public Health System (SUS) registering an average of 7000 births a year.
The
Centro de Referência em Doenças Infecciosas (CERDI) (Reference Center for Infectious Diseases), located in one of the polyclinics in the city, assists children exposed to vertical transmission diseases referred from maternity hospitals for follow-up after hospital discharge, in the same city or in the whereabouts.
The target population of this study was children and mothers with a diagnosis of toxoplasmosis referred from maternity hospitals, according to the city protocol. Children born of mothers who presented tests suggestive of seroconversion for the disease (positive IgM and IgG, or positive IgM and/or IgA) during prenatal care, or mothers initially susceptible to the disease who presented positive IgM and/or IgG (ascending titers) during pregnancy were included. Mothers with positive serology (IgM) at the time of delivery and who did not have previous serologies were also included. Mothers with serology suggestive of immunity acquired prior to the current pregnancy and mothers who had evidence of false positive IgM were excluded, that is, those who did not achieve IgG seroconversion even after 30 days of the initial IgM test.
The children were examined monthly in the first six months of life and then every three months if they were not under treatment. In case the children were under treatment, the appointments were held monthly until the first year of life. The children were followed up for at least one year and the conclusion of the diagnosis was based on the persistence or absence of IgG titers for toxoplasmosis. Fundoscopic examinations were performed at birth, at three and six months. For children diagnosed with disease, the intervals were established based on the alterations found and the opinion of the specialist, as well as on the neurological evaluation and cephalic segment CT scan.
IgM and IgG dosages were performed in the first appointment and monthly in the first six months (to certify the decrease and/or rise of IgG titers). The IgA dosage was collected, whenever possible, after the tenth day until the third month of the child's life. Tests performed with the same serological technique and collections conducted in the same laboratory were prioritized. The collection of maternal serology for pairing with the child's first examination was also performed whenever possible.
Data collection was conducted prospectively directly from medical records using specially constructed forms, addressing variables on maternal characteristics (age, schooling, beginning of prenatal care, number of appointments attended, prophylactic counseling, eating habits, presence of animals in the peridomicile), exams performed during prenatal care (serologies, amniocentesis with amniotic fluid study),treatment performed during pregnancy (treatment time, drug regimen used, period of use, adverse reactions), birth data (weight, head circumference, Apgar score, presence of clinical and/or laboratory changes, ophthalmologic evaluation, transfontanellar ultrasound or cranial CT scan, CSF study, treatment and presence of sequelae) and follow-up data until the conclusion of diagnosis.
After specific coding, the data were registered in the IBM SPSS version 22 software (Armonk, NY; USA). The variables were assessed based on the distribution of absolute frequencies and percentages. Pearson's chi-square test was used in the definition of factors associated with sequelae, assuming a significance level of 5% (
p<0.05) for comparative analyses between the periods studied.
The project was approved by the Research Ethics Committee of the
Universidade Estadual de Montes Claros (UNIMONTES) protocol No. 2,341,969 and CAAE. 73134517.9.0000.5146.
Results79 binomials (mother-child) were followed up during the period 2016-2019. The population studied was predominantly urban (83.5%) and from the city where the study was conducted. The percentage of adolescent mothers was 17.7% and schooling level equal to or less than eight years (complete elementary school) was recorded for 11.4% of the mothers. Table 1 presents the results characterizing the group studied in a comparative way between the two periods.
A significant change was found regarding the age group of the mothers, such as an increase in the number of mothers over 30 years of age (35.4%) and a reduction in the proportion of adolescent mothers (17.7%). In relation to schooling, there was a significant reduction in the proportion of mothers with eight years or less of schooling.
As to prenatal care, 66 mothers (83.5%) attended more than six consultations, 60 of them (75.9%) started prenatal care in the first trimester and 55 (68.4%) did not receive prophylactic counseling for toxoplasmosis. Regarding eating habits, 42 (53.2%) mothers reported having ingested raw food (such as milk, vegetables, fruit) and 18 (22.8%) reported eating under cooked meat. Concerning the presence of animals at home and in the peridomicile, 39 (49.4%) reported having cats, 10 (12.7%) had other kind of animals besides cats (dogs, chickens, poultry, goats, or cattle) and 11 (13.9%) practiced gardening without the use of gloves during pregnancy.
Most mothers were screened for
T. gondii during pregnancy and only two did not perform any serological tests. Compared to the previous period, Table 1 shows a significant increase in the proportion of mothers who had serological tests performed during pregnancy (
p=0.007). An increase in the number of specific tests for toxoplasmosis performed during pregnancy as well as a reduction in the proportion of mothers who had no serological test performed (
p<0.001) were also observed. The proportion of more recent diagnoses was significantly higher for the group of mothers in the period 2016-2019(
p<0.001). IgG and IgM dosage for Toxoplasmosis was conducted three or more times for 33 (41.8%) mothers and 68 (86.1%) did not have IgA dosage performed. IgG avidity test was requested for 40 (50.6%) mothers during prenatal care, of these, 15 (19%) performed with in the 16
th week of gestation. 28 (35.4%) avidity tests were above the cutoff point for the exam indicating high avidity. Only 6 (7.6%) pregnant women underwent amniocentesis and amniotic fluid examination and only one exam turned out positive.
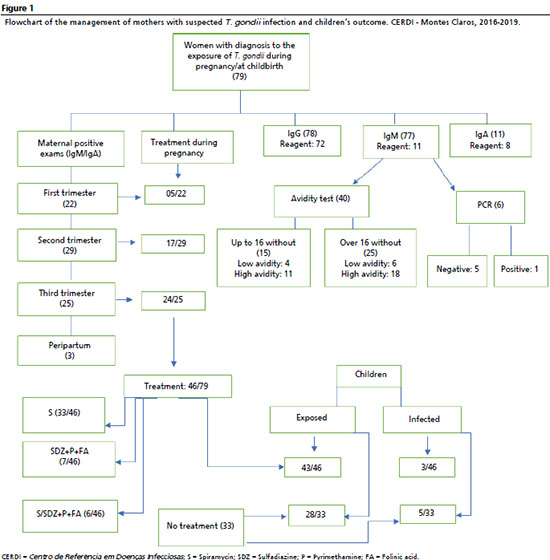
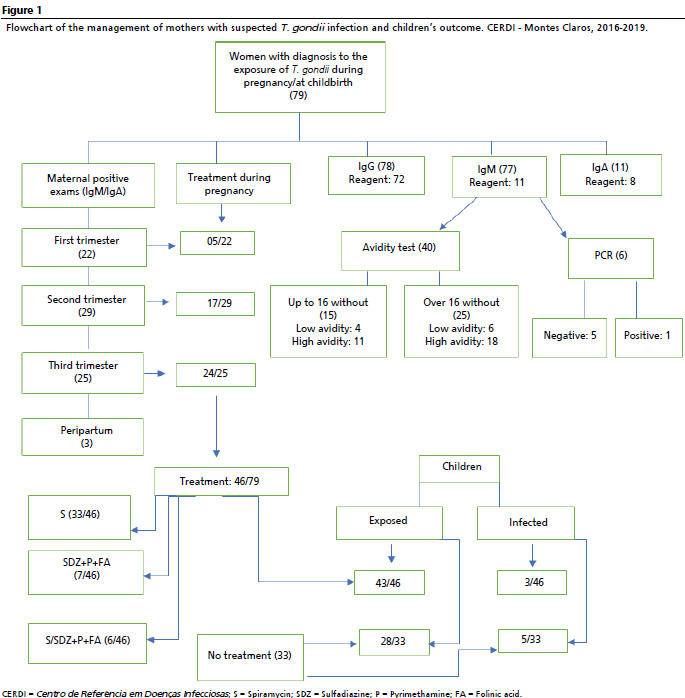
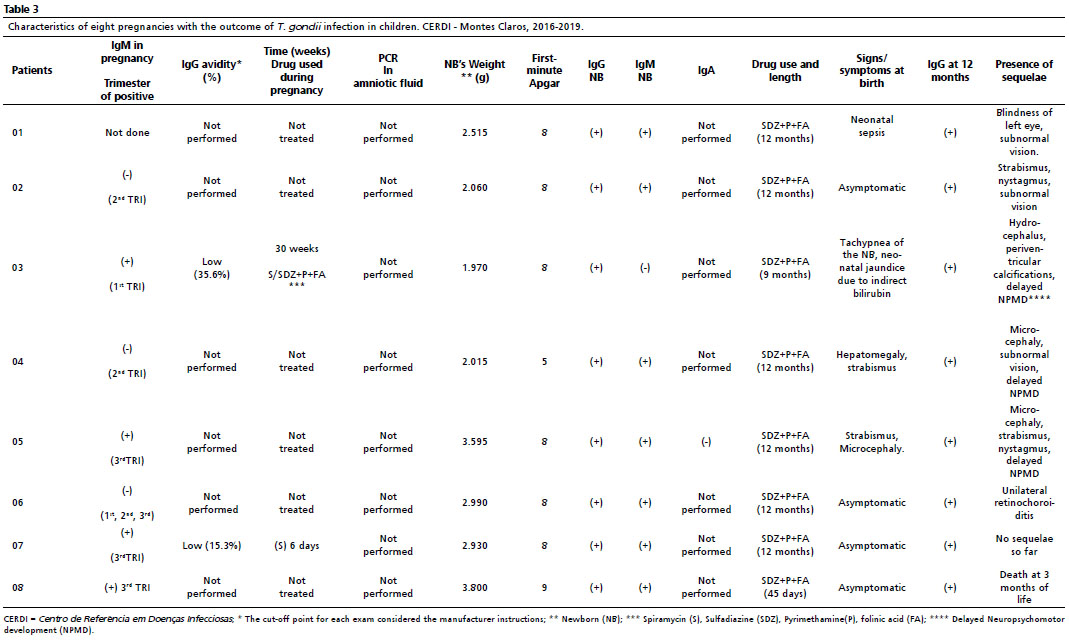
Treatment was provided to 46 (58.2%) pregnant women within the three trimesters of pregnancy, either at the time of diagnosis or after referral to high-risk prenatal care units. The length of the treatment varied widely, from 4 days to 224 days, with an average of 43.7 days. Spirampycin (S) was the most used drug, prescribed to33 (41.8%) pregnant women, followed by sulfadiazine (SDZ), pyrimethamine (P), folinic acid (FA) prescribed to 7 (8.9%) pregnant women and the alternating association of SDZ+P+FA/S were prescribed to 6 (7.6%). Figure 1 shows the flowchart of the management of mothers with suspected toxoplasma infection, therapeutic management, and the child's outcome.
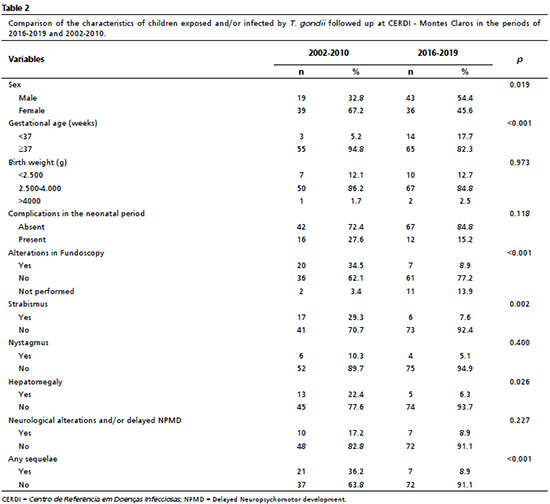
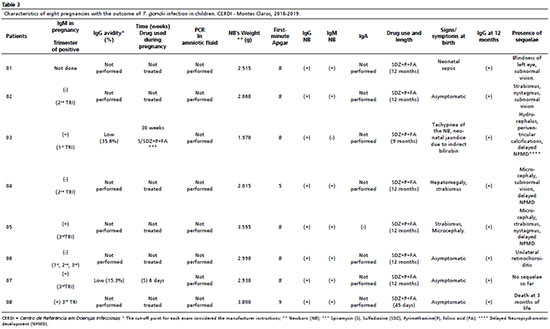
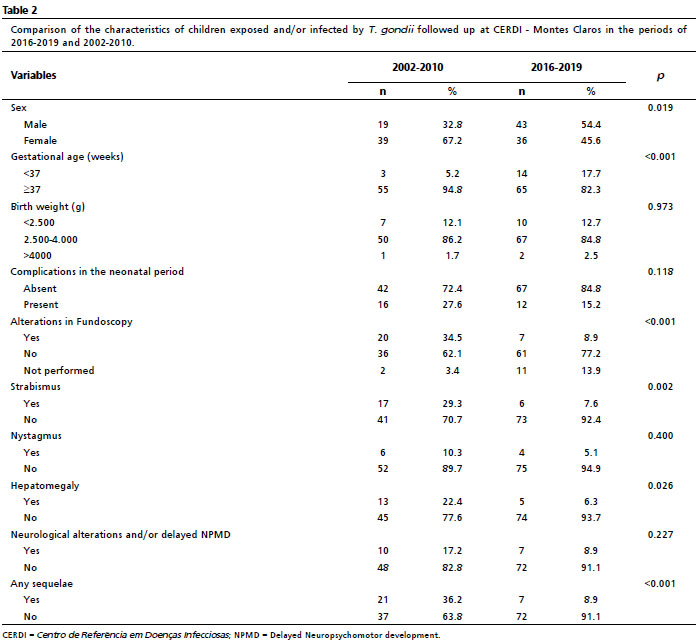
Between 2016 and 2019, 79 binomials were accompanied, and most of the children assisted were asymptomatic (82.3%). There was a slight predominance of males (54.4%) and 69 neonates (87.3%) had the appropriate weight (more than 2,500g) at birth. It was observed a high percentage of the children accompanied were preterm (82.3%), which represented a significant increase compared to the percentage found in the previous study. In relation to the previous study, there was also a higher proportion of male children. Table 2 presents the characteristics of the children accompanied compared to the group previously evaluated. As for clinical aspects, the findings showed fewer changes in fundoscopy, strabismus, hepatomegaly, and the presence of sequelae in the group most recently accompanied, with statistically significant differences. The characteristics of children in eight pregnancies with the outcome are presented in the Table 3.
Physical examination at birth showed some abnormality for 12 children (15.2%), with overlap of some manifestations registered. Hepatomegaly was present in 5 (6.3%) children, strabismus in 3 (3.8%), microcephaly in 2 (2.5%), respiratory disorders in 5 (6.3%) and neonatal septicemia in 8 (10.1%).
Ophthalmological examination was performed in 68 (86.1%) children at birth and 11 (13.9%) had performed the exam only after the outpatient follow-up started. Some ocular lesion was identified in 7 (8.9%) children until the third month of life, being bilateral retinochoroiditis the most common lesion, present in four pairs of eyes.
Regarding the investigation of the central nervous system, 32 (40.5%) children underwent transfontanellar ultrasound with alterations found in 4 (12.5%) ultrasounds,1 microcephaly, 1 calcification, 1 intravascular hemorrhage and 1 hydrocephalus. 27 (34.2%) children underwent cephalic segment TC scan with alterations found in 6 (22.2%) scans, microcephaly in 2, calcification in 2 and hydrocephalus in 2. 17 (21.5%) infants underwent lumbar puncture with CSF study, being hyperproteinorraquia the most common alteration found in 3 (3.8%) tests.
IgG resulted completely negative up to the sixth month of life for 54 (69.0%) children. 8(10.1%) children had a confirmed diagnosis of the disease with 7 (8.9%) presenting at least one sequela.
DiscussionBy comparing the two studies, it is possible to observe a positive advance concerning the care for the mother-child binomial affected by
T. gondii. The comparison of maternal characteristics in the two periods has shown no difference between the origin and place of residence of the mothers. However, regarding maternal age, there was a lower number of pregnant adolescents with the disease and an increase in the number of women over 30 years of age infected with toxoplasma.
10 The results show that the service has been gaining visibility with an increase in prenatal screening, considering the higher number of patients in four years, compared to the number registered during the eight years of the previous study.
The higher number of mothers screened, with significant differences also seen in relation to the number of exams performed during prenatal care, led to a greater number of mothers being diagnosed. Regarding to the period of diagnosis, the data demonstrates a tendency towards earlier diagnosis, although there is still a delay in recognizing and treating the infected mothers, perhaps due to delay in scheduling the exams or the late returns of the patients with the requested tests.
No national studies evaluating the management of toxoplasmosis during pregnancy in an evolutionary way, considering such distinct periods, have been identified. In Rio de Janeiro, between 2014 and 2017, the follow-up of a group of infected pregnant women revealed that there are still important barriers to coping with the problem, such as late referral to specialized services or inadequate management in prenatal services, in addition to social issues involving the persistent occurrence of cases of congenital toxoplasmosis.
11 Similar findings were also seen in a study in Minas Gerais State, in which the prevalence was related to worse hygiene rates, difficulty in accessing health care and worse school performances of the pregnant women, highlighting the need for wide surveillance of the disease and associated risk factors.
4Despite the increase in serological testing for toxoplasmosis during pregnancy, it was observed that most mothers were tested less than twice, a number lower than what is recommended by the Ministry of Health.
2 It was also observed that it is not a regular practice for healthcare professional to request other markers indicative of acute phase. IgA dosage for the disease was occasional and very few pregnant women had it done associated with IgM dosage. That association could improve the sensitivity of acute phase markers to predict recent infection and thus enable earlier treatment.
12,13 It is relevant to highlight that the avidity test is a good marker of the acute phase and, when performed until the 16
th week of gestation, can indicate the period of possible maternal contamination, but it is not performed by SUS in the city of the study. Many times, the time between the request of the first exams and the delivery of the results exceeds 16 weeks of gestation. Still, it is not possible to rule out the ignorance of the validity of this test by health professionals in the city.
Regarding amniocentesis and the study of amniotic fluid, fewer tests were carried out compared to the previous study. A negative PCR test does not rule out the diagnosis of toxoplasmosis, but, when positive, it has a high positive predictive value for inferring fetal involvement close to 100%.
5,14 However, it is worth mentioning, due to logistical and cost issues, although the collection of the exam is conducted by the SUS in the high-risk services of the maternity hospitals of the municipality, the exam can only be performed through the SUS via the Ezequiel Dias Foundation - Belo Horizonte, PCR test was restricted to the private laboratories in the period 2017-2019.
Although the FHS network in the city where the study was conducted is currently three times larger compared to the previous study, a significant number of pregnant women did not receive any prophylactic counseling on the disease. This is a relatively simple measure with potential impact. Countries in which the disease is systematically addressed such as France and Belgium have even reported a decrease in the risk of infection by up to 63% due to health education.
15,16A recent multicenter study conducted in France pointed out a tendency of lower transmission of the disease to the fetus when the pregnant woman was treated with the Sulfadiazine/Pyrimethamine regimen compared to Spiramycin.
7 In the present study as well as in the previous one, the number of untreated pregnant women remained high due to the lack of knowledge on the part of professionals or resistance to prescribing the combined regime. It could be reversed since the drugs cross the placental barrier and treat the fetus.
16 It is worth noting that the combined regime requires close supervision because of the risks of adverse events.
7,17Regarding accompanied children a proportionally higher number of preterm babies was also observed and, although the disease itself increases the risk for prematurity
5, only 4(28.6%) out of 10 children had the final diagnosis of congenital toxoplasmosis. It is possible that the number of preterm births increased owing to other obstetric reasons or complications specific to pregnant women. Considering that the current study was not intended to analyze this aspect, this relation should be further investigated in future studies.
As found in other studies, most children were asymptomatic at birth and there was a lower proportion of children affected with some sequelae, which represented a drop of about 75%. Still comparing to the group of children in the first study, a lower proportion of hepatomegaly, strabismus and changes in the fundoscopy examination was registered .
9 This is a relevant finding. Although this study did not show a statistically significant difference between the groups treated in the two periods, it was observed that the number of affected children among the untreated mothers was twice as high as that of mothers treated during pregnancy, which may indirectly represent an improvement in the management of pregnant women exposed to
T. gondii. There is consensus about the benefits of the early start of maternal treatments once it can prevent fetal involvement or more severe cases from occurring.
7,17-19Of the ocular lesions, bilateral retinochoroiditis prevailed in both studies, and subnormal vision was found in nearly 50% of the affected children. This result is in line with the literature regarding the presence of more severe and more frequent ocular lesions in Brazil when compared to Europe.
20One limitation for the study lies in the process of inclusion of the children followed up. Although all children referred to CERDI -Montes Claros were included, it is possible that some of them did not return for follow-up due to the fact that there is no control in the flow among the maternity hospitals and the specialized service. There is also the fact that many pregnant women come to Montes Claros exclusively for childbirth and do not return for follow-up, making it difficult to notify children affected by the disease. In other words, it is possible that the group evaluated represents the reality only in part, once for a large number of patients the diagnosis is established only in the follow-up of the child and for the families it is often difficult to understand the prospect of a latent disease in face of a seemingly "normal" baby. Another limitation is the fact that the mandatory testing for toxoplasmosis at birth for pregnant women who remained susceptible to the disease during pregnancy is not yet established at the maternity hospitals.
Despite the limitations, this study has revealed that the reference service has been able to gradually sensitize primary healthcare agents in the management of gestational toxoplasmosis. There was an increase in the number of cases followed up between the two periods, which translates into a greater prominence and recognition of the service. In the first study, the reality of the disease in the city was unknown; since then, the service has grown, it has become a reference for the care of these children and, for the last five years, educational workshops on the disease have been offered to health professionals from the ESF and hospitals. The fact that the same professional conducted the data collection and follow-up of children in the two periods studied also represents a positive aspect of the study, ensuring greater reliability to the data registered.
The results represent a warning to managers and health professionals. There is still a long way to go to make toxoplasmosis a common knowledge of the population. In this sense, the goal of health managers should include actions such as intensifying prophylactic measures in communities, broadening the understanding of the disease among health professionals, health surveillance agents and even professionals from administrative sectors and educators. These measures have the potential to prevent unfavorable outcomes of the disease and improve the quality of assistance for the infected binomials (mother-child).
References1. Ministério da Saúde (BR). Secretaria de Vigilância das Doenças Transmissíveis. Boletim Epidemiológico. Doenças Tropicais negligenciadas. Brasília (DF); Ministério da Saúde; 2021. [access in 2022 abr 3]. Available from:
https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/especiais/2021/boletim_especial_doencas_negligenciadas.pdf2. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância das Doenças Transmissíveis. Protocolo de Notificação e Investigação: Toxoplasmose gestacional e congênita. Brasília (DF); Ministério da Saúde; 2018. [access in 2022 abr 3]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/protocolo_notificacao_investigacao_toxoplasmose_gestacional_congenita.pdf3. Wallon M, Peyron F. Congenital Toxoplasmosis: A Plea for a Neglected Disease. Pathogens. 2018 Feb;7 (1): 25.
4. Carellos EV, Caiaffa W, Andrade GMQ, Abreu M, Januário JN. Congenital toxoplasmosis in the state of Minas Gerais, Brazil: a neglected infectious disease? Epidemiol Infect. 2014; Mar; 142 (3): 644-55.
5. Maldonado YA, Read JS. Diagnosis, Treatment, and Prevention of Congenital Toxoplasmosis in the United States. Pediatrics. 2017 Feb; 139 (2): e20163860.
6. Wallon M, Peyron F, Cornu C, Vinault S, Abrahamowicz M, Kopp CB,
et al. Congenital toxoplasma infection: monthly prenatal screening decreases transmission rate and improves clinical outcome at age 3 years. Clin Infect Dis. 2013 May; 56 (9): 1223-31.
7. Mandelbrot L, Kieffer F, Sitta R, Laurichesse-Delmas H, Winer N, Mesnard L,
et al. Prenatal therapy with pyrimethamine þ sulfadiazine vs spiramycin to reduce placental transmission of toxoplasmosis: a multicenter, randomized trial. Am J Obstet Gynecol. 2018 Oct; 219 (4): 386.e1-e9.
8. McLeod R, Boyer K, Karrison T, Kasza K, Swisher C, Roizen N,
et al. Outcome of treatment for congenital toxoplasmosis, 1981-2004: the National Collaborative Chicago-Based, Congenital Toxoplasmosis Study. Clin Infect Dis. 2006; 42 (10): 1383-94.
9 Soares JA, Carvalho SF, Caldeira AP. Profile of pregnant women and children treated at a reference center for congenital toxoplasmosis in the northern state of Minas Gerais, Brazil. Rev Soc Bras Med Trop. 2012; 45 (1): 55-9.
10. Moura FL, Amendoeira MR, Bastos OM, Mattos DP, Fonseca AB, Nicolau JL,
et al. Prevalence and risk factors for Toxoplasma gondii infection among pregnant and postpartum women attended at public healthcare facilities in the City of Niteroi, State of Rio de Janeiro, Brazil. Rev Soc Bras Med Trop. 2013; 46 (2): 200-7.
11. La Fuente Villar BB, Neves ES, Louro VC, Lessa JF, Rocha DN, Gomes LHF,
et al. Toxoplasmosis in pregnancy: a clinical, diagnostic, and epidemiological study in a referral hospital in Rio de Janeiro, Brazil. Braz J InfectDis. 2020; 24 (6): 517-23.
12. Olariu TR, Blackburn BG, Press C, Talucod J, Remington JS, Montoya JG. Role of Toxoplasma IgA as Part of a Reference Panel for the Diagnosis of Acute Toxoplasmosis during Pregnancy. J Clin Microbiol. 2019; 57 (2): e01357-18
13. Murata FH, Ferreira MN, Camargo NS, Santos GS, Spegiorin LC, Silveira-Carvalho AP, et al. Frequency of anti- Toxoplasma gondii IgA, IgM, and IgG antibodies in high-risk pregnancies, in Brazil. Rev Soc Bras Med Trop. 2016; 49 (4): 512-4.
14. Montoya JG, Remington JS. Management of Toxoplasma gondii infection during pregnancy. Clin Infect Dis. 2008; 47 (4): 554-66.
15. Picone O, Fuchs F, Benoist G, Binquet C, Kieffer F, Wallon M,
et al. Toxoplasmosis screening during pregnancy in France: Opinion of an expert panel for the CNGOF. J Gynecol Obstet Hum Reprod. 2020; 49 (7): 101814.
16. Foulon W, Naessens A, Derde MP. Evaluation of the possibilities for preventing congenital toxoplasmosis. Am J Perinatol. 1994; 11 (1): 57-62.
17. Peyron F, L'Ollivier C, Mandelbrot L, Wallon M, Piarroux R, Kieffer F,
et al. Maternal and Congenital Toxoplasmosis: Diagnosis and Treatment Recommendations of a French Multidisciplinary Working Group
. Pathogens. 2019 Feb; 18; 8 (1): 24.
18. Strang AGGF, Ferrari RG, Rosário DK, Nishi L, Evangelista FF, Santana PL,
et al. The congenital toxoplasmosis burden in Brazil: Systematic review and meta-analysis. Acta Trop. 2020 Nov; 211: 105608.
19. Olariu TR, Press C, Talucod J, Olson K, Montoya JG. Congenital toxoplasmosis in the United States: clinical and serologic findings in infants born to mothers treated during pregnancy. Parasite. 2019; 26: 13.
20. Gilbert RE, Freeman K, Lago EG, Bahia-Oliveira LM, Tan HK, Wallon M,
et al. Ocular sequelae of congenital toxoplasmosis in Brazil compared with Europe. PLoS Negl Trop Dis. 2008; 2 (8): e277.
Received on June 16, 2022
Final version presented on September 18, 2022
Approved on September 21, 2022
Associated Editor: Alex Sandro Rolland
Authors' contribution: Soares JAS: design and execution of the project, collection, analysis and interpretation of data, writing of the manuscript. Holzmann APF, Alves BBS and Lima CFQ: collection, analysis and interpretation of data. Caldeira AP: coordination, design and execution of the project, collection, analysis and interpretation of data, writing of the manuscript.
The authors approved the final version of the article and declare that there is no conflict of interest.


 ; Ana Paula Ferreira Holzmann2
; Ana Paula Ferreira Holzmann2






 Ler em português
Ler em português