ABSTRACT
OBJECTIVES: to assess the supply of human milk exclusively to prematures in a Neonatal Intensive Care Unit and the influence of external and organizational contexts on the degree of implementation of this intervention.
METHODS: this is an implementation evaluation with analysis of the external context (sociodemographic situation of mothers, support network and industry marketing) and organizational context (belonging to the hospital unit). To define the degree of implementation, the Analysis and Judgment Matrix was used, considering the compliance dimension, and the availability and technical-scientific quality sub-dimensions. The data used were obtained through interviews, semi-structured questionnaires and analysis of documents from the institution.
RESULTS: the degree of implementation of the intervention was 80.74%, proving to be satisfactory, with emphasis on the technical-scientific quality sub-dimension.
CONCLUSIONS: the success in the supply of human milk is linked to public policies, the support and guidance offered to mothers in the hospital unit, presence of a support network, knowledge of mothers about the benefits of breastfeeding, adequate infrastructure and availability of supplies. The prematures being hospitalized in a child-friendly hospital contributed to the implementation of the intervention.
Keywords:
Human milk, Premature newborn, Neonatal intensive care unit, Maternal-child health services, Health evaluation
RESUMO
OBJETIVOS: avaliar o fornecimento de leite humano de forma exclusiva aos prematuros em uma Unidade de Terapia Intensiva Neonatal e a influência dos contextos externo e organizacional no grau de implantação dessa intervenção.
MÉTODOS: trata-se de uma avaliação de implantação com análise dos contextos externo (situação sociodemográfico das mães, rede de apoio e marketing da indústria) e organizacional (pertencente à unidade hospitalar). Para definir o grau de implantação, foi utilizada a Matriz de Análise e Julgamento, considerando a dimensão conformidade, e as subdimensões disponibilidade e qualidade técnico-científica. Os dados utilizados foram obtidos por meio de entrevistas, questionários semiestruturados e análise de documentos da instituição.
RESULTADOS: o grau de implantação da intervenção foi de 80,74%, mostrando-se satisfatório, com destaque para a subdimensão qualidade técnico-científica.
CONCLUSÕES: o sucesso no fornecimento de leite humano está atrelado às políticas públicas, ao apoio e orientações oferecidos às mães na unidade hospitalar, disponibilidade de rede de apoio, conhecimento das mães acerca dos benefícios do aleitamento materno, infraestrutura adequada e disponibilidade de insumos. Os prematuros estarem internados em hospital amigo da criança contribuiu para a implantação da intervenção.
Palavras-chave:
Leite humano, Recém-nascido prematuro, Unidade de terapia intensiva neonatal, Serviços de saúde materno-infantil, Avaliação em saúde
IntroductionExclusive breastfeeding (EBF) is recognized worldwide as a practice that provides the greatest benefits to premature babies, defined as those born before 37 weeks of gestation, and is the natural way to supply essential nutrients for healthy growth and development.
1-3Studies show that low birth weight prematures fed on breast milk have shorter hospitalization, better prognosis for neurological development, lower risk of developing enterocolitis, decrease weight loss, and increase survival, compared to those breastfed with nutritional formulas.
4In view of the benefits of human milk (HL) and in order to reduce infant mortality rates in the country, several actions have been developed in order to promote, protect, and support breastfeeding, such as the creation of the
Normas Brasileiras de Comercialização de Alimentos para Lactentes (NBCAL) (Brazilian Standards for the Commercialization of Foods for Infants), through Law No. 11. 265/2006,
5 creation of the
Rede Brasileira de Bancos de Leite Humano (rBLH-BR) (Brazilian Network of Human Milk Banks),
Iniciativa Hospital Amigo da Criança (IHAC) (Child-Friendly Initiative Hospital),
Implantação do Método Canguru, (Implementation of the Kangaroo Method) publication of Ordinance No.930/2012,
6 guaranteeing free access to parents with the hospitalized newborn (RN), during 24 hours, among others.
7Despite the importance of breastfeeding, the birth of a premature newborn (PMNB) can impose several barriers on this practice. The delay in the beginning of milk production, difficulties in extraction techniques, lack of support from health professionals, and separation from the binomial are noteworthy.
8,9 Other factors such as the woman's socioeconomic status, infrastructure of the unit, the organization of the services on health work process, and the infant food industry's marketing may also contribute to early weaning in the Neonatal Intensive Care Unit (NICU).
10,11Thus, strategies to strengthen breastfeeding should be implemented and monitored by the institution through the evaluation of work processes and services provided.
In the public health, the main purpose of evaluation is to support the decision-making processes within the
Sistema Único de Saúde (SUS) (Brazilian Public Health System), subsidizing to identify problems and reorient actions and services developed by the institution.
12Evaluation consists fundamentally of making a valued judgment about an intervention or about any of its components with the purpose of helping in the decision making process. In the implementation analysis, it is possible to measure the influence of contextual factors on the effects and the degree of implementation of the intervention.
13Given the above, as the factors that may contribute to early weaning are known, more effective interventions can be targeted to mitigate such factors, favoring the success of breastfeeding (BF). The objective of this research is to evaluate the provision of exclusive HM to premature babies in a NICU and the influence of the external and organizational contexts on the degree of implementation of this intervention.
MethodsThis is an implementation of an evaluation withanalysis of the external and organizational contexts, whose design is a single case study, with a single level of analysis, cross-sectional and with data triangulation, combining qualitative and quantitative data collection methods and sources.
For the case selection, the sample was convenience and the inclusion criterion was to be accredited by IHAC. As the main researcher already performed her activities at the
Hospital Materno Infantil de Brasília (HMIB), this unit was chosen for the development of this study.
Data collection was carried out in the NICU at the HMIB, a unit accredited by the IHAC since 1996, from October 1, 2020 to November 30, 2020 using a semi-structured instrument. According to the rBLH-BR, the Federal District is nationally recognized for its capacity to collect HM, being the only place in the world with 100% coverage of milk banks and collection stations in public and private health units with NICUs, making it a reference in collection and distribution of HM.
14The degree of implementing the intervention was assessed using the analysis and judgment matrix (AJM), whose indicators were drawn from the logic model of the intervention and the compliance dimension, with the subdimensions availability and technical and scientific quality, to assess the implementation of the available structure and the actions aimed at the exclusive supply of HM. The logic model, represented in Figure 1, was built based on the technical and regulatory material of the intervention (Table 1).
Two AJMs were prepared, one for each subdimension, and the total of the matrices served as the basis for calculating the judgment of the degree of implementation, obeying the following cut-off points: ≥80% implemented; 40-79.9% partially implemented; ≤39.9% critical implementation. The percentage of adequacy of each indicator was calculated from the formula: (PA x 100) / PE, where PA represents the score achieved and PE to the expected score.
The data used in this research to answer the AJMs were collected from primary sources (interview and semi-structured instrument), in addition to the analysis of the documents of the institution.
The participants' selection was carried out according to the following inclusion criteria: health professionals who work in the NICU at the HMIB and perform activities related to the care of prematures; head of the Human Milk Bank (HMB) and the Nutrition sector; prematures with gestational age less than 37 weeks, with admission to the NICU in the first 48 hours of life and a minimum hospitalization of 48 hours in the unit; mothers aged ≥18 years and who are with their child admitted to the NICU. Exclusion criteria were: professionals who refused to participate in the study and who did not provide direct assistance to the prematures; PMNBs who had malformation, were abandoned or died during hospitalization; the mother's refusal to participate in the study and maternal death.
The data collection instrument included four phases, with the first three phases taking place in October, 2020, and the fourth phase in November, 2020:
Phase IConsultation of diet charts of 53 PMNBs admitted to the NICU, including the following data from medical records: sex; gestational age; birth weight; breastfeeding onset (<24h, 24 to 48h or >48 hours from birth); nutritional therapy (HM, infant formula and fortifier); via administration; justification for the use of infant formula.
Phase IISemi-structured interviews with the mothers of PMNBs, of which 11 were nursing mothers and nine were daily nurse-mothers. The nursing mothers were considered as those who could get a bed in the unit for 24 hours/day, while the daily nurse-mothers spent the day in the unit and returned to their homes at the end of the day. Each mother who authorized the recording of the interview was identified with the letter M and the interview number (M1, M2, M3. . . ) to maintain the participants' anonymity.
The variables collected in the interviews were: sociodemographic data (age, marital status, schooling, family income, and profession); prenatal care; availability of support network; information on breastfeeding (guidance, extraction techniques, difficulties and facilities during breastfeeding/extraction, skin-to-skin contact, access to the NICU, and type of infant feeding); unit infrastructure (place for milk extraction, food provided to mothers, physical space, and accommodations).
Phase IIIAn online instrument was applied to 51 health professionals at the NICU, and the head of the MBH and Nutrition using the Google Forms tool, through a link sent by WhatsApp, whose quantitative results were automatically generated. Of all NICU health professionals who answered the questionnaire, 31.4% were physicians, 25.5% nursing technicians, 21.6% nurses, 11.8% physical therapists and 9.8% speech therapists.
The NICU health professionals were questioned about the infrastructure conditions for accomdating mothers, skin-to-skin contact, free access of mothers to the NICU as provided in the Ordinance No.930/2012,6 knowledge of the breastfeeding policy of the HMIB, whether they had already been trained by the IHAC course, facilitators and barriers to breastfeeding prematures in the unit, actions to provide guidance and encourage breastfeeding, difficulties in prescribing HM, and reasons for prescribing infant formula, according to the recommendations of the World Health Organization (WHO).
15The head of Nutrition responded to the instrument regarding the food provided to mothers of PMNBs and the presence of infant formula and fortifier in the unit. The head of the MBH responded regarding the presence of HM; infrastructure; difficulties in keeping stocks stored; and guidance on breastfeeding/extraction. They were also asked about the impact of the COVID-19 pandemic on HM storage.
Phase IVAn analysis of the documents from the institution was carried out, which included the analysis of the records on HM, fortifier, and infant formula; and analysis of the NICU's breastfeeding policy.
Quantitative data collected in the interviews and consultation of diet charts were compiled in an Excel spreadsheet, version 2007. Regarding qualitative data, the recorded interviews were transcribed and grouped by subject, and the mothers' statements were used to confirm and clarify the quantitative findings. The answers to the open questions were classified by category, and content analysis was performed.
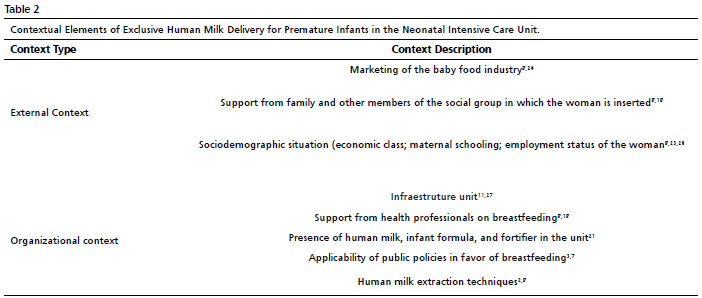
16The analysis of the external and organizational context was performed as shown in Table 2. The external context was described from the interviews with the mothers, being possible to identify the facilities and barriers in the breastfeeding process, sociodemographic aspects such as schooling, marital status and womean's employment status and availability of family support network. The industry marketing was evaluated by applying the online instrument with the NICU prescribing physicians.
The organizational context was described based on aspects related to the physical structure of the unit, such as a private place for breast milking, adequate food during the stay in the unit, and accommodations for the mothers' 24-hour stay in the hospital; presence of HM, fortifier, and infant formula; training of health professionals; professionals' knowledge regarding the practices aimed for the promotion, protection, and support of EBF; and actions for breastfeeding guidance and encouragement.
This study was approved by the Research Ethics Committee of the
Escola Nacional de Saúde Pública (CAAE: 35533320.6.0000.5240) and of the
Fundação de Ensino e Pesquisa em Ciências da Saúde (CAAE: 35533320.6.3001.5553).
ResultsThe implementation degree of exclusive supply of HM for premature infants was 80.7%, a satisfactory percentage, with emphasis on process indicators.
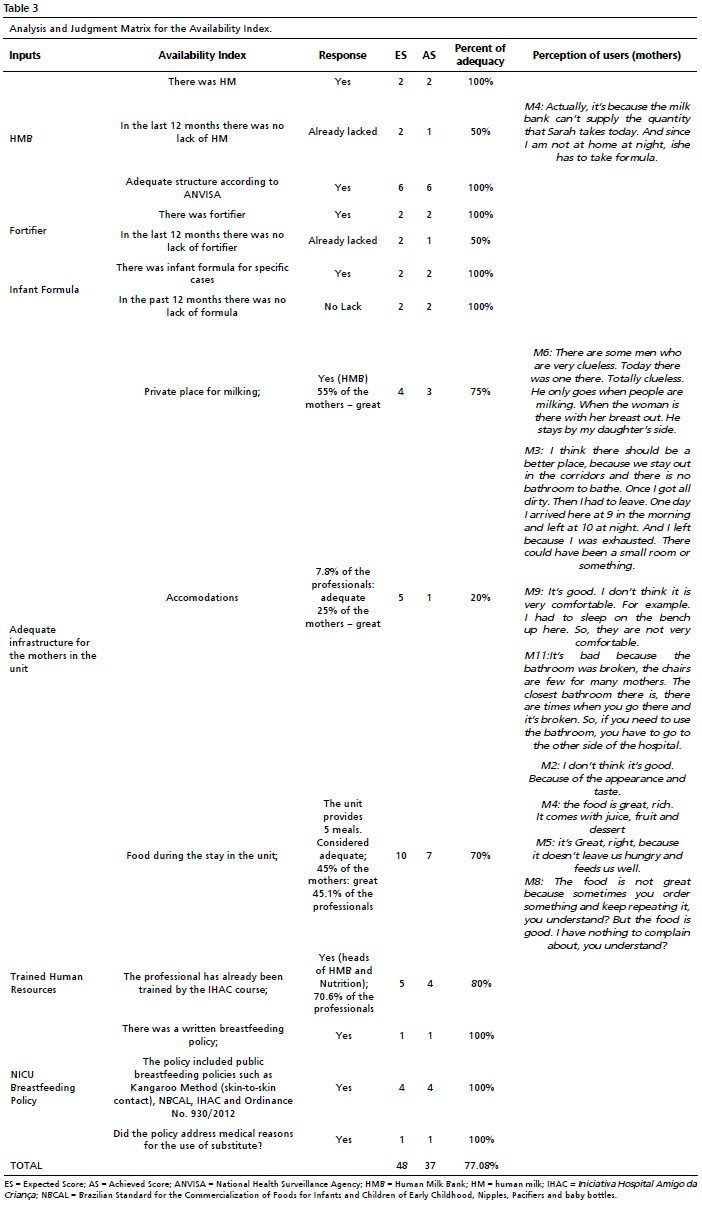
The first set of results refers to the characterization of the degree of implementation for the availability subdimension, which takes into account the structure indicators (input component), as shown in Table 3. The implementation of the input component was 77.0%, considered partially implemented. The availability of HM from the HMB and fortifier, and the infrastructure for the mothers' reception with a focus on accommodations were the inputs that presented the lowest percentages of adequacy (50% and 20%, respectively).
At the time the questionnaire was applied, stocks of HM, fortifier, and infant formulas were stored. However, in the last 12 months, there was a shortage at some point or a critical period of lack of fortifier and HM. In the absence of HM, it was recommended that "
Infants with 25ml of prescribed diet per schedule, weighing more than 1850 grams, use formula for premature infants. "
Among the difficulties encountered in keeping the HM stored, the head of the HMB reported lack of equipment maintenance and lack of human resources. Although the stocks were stored, PMNBs did not receive all the volume of HM they needed. This statement is confirmed by the NICU mother's speech in which her baby used formula.
Regarding accommodations, this item, which was considered only 20% implemented, was evaluated by both mothers and NICU professionals. Of all mothers, 25% considered the accommodations as great; 50% reported them as good and 25% as poor. The main complaints/ dissatisfactions of nursing mothers were related to the beds they occupied: inadequate cleanliness, size and lack of ventilation, in addition to the absence of a laundry room to wash and dry the mothers and babies' clothes.
The daily nursing-mothers pointed out inadequacies in the bathrooms (lack of private bathroom, bad aspect, broken bathrooms and far from the NICU), chairs (broken and in insufficient quantity) and lack of place for bathing and resting.
The mothers' age ranged from 18 to 41 years, with a mean of 29 years (standard deviation = 7.7); 50% of them were "housewives"; 40% had completed high school; 75% were married or in a stable union, with a mean family income of one to two minimum wages. Regarding the current pregnancy, all of them had prenatal care, with an average of 8 consultations. The mothers who were interviewed, reported having a support network to help them with the baby and other children's care; 100% could count on at least one family member and 10% could also count on friends.
According to the professionals, only 7.8% considered the physical space and accommodations appropriate and sufficient to meet all mothers of premature babies in the NICU.
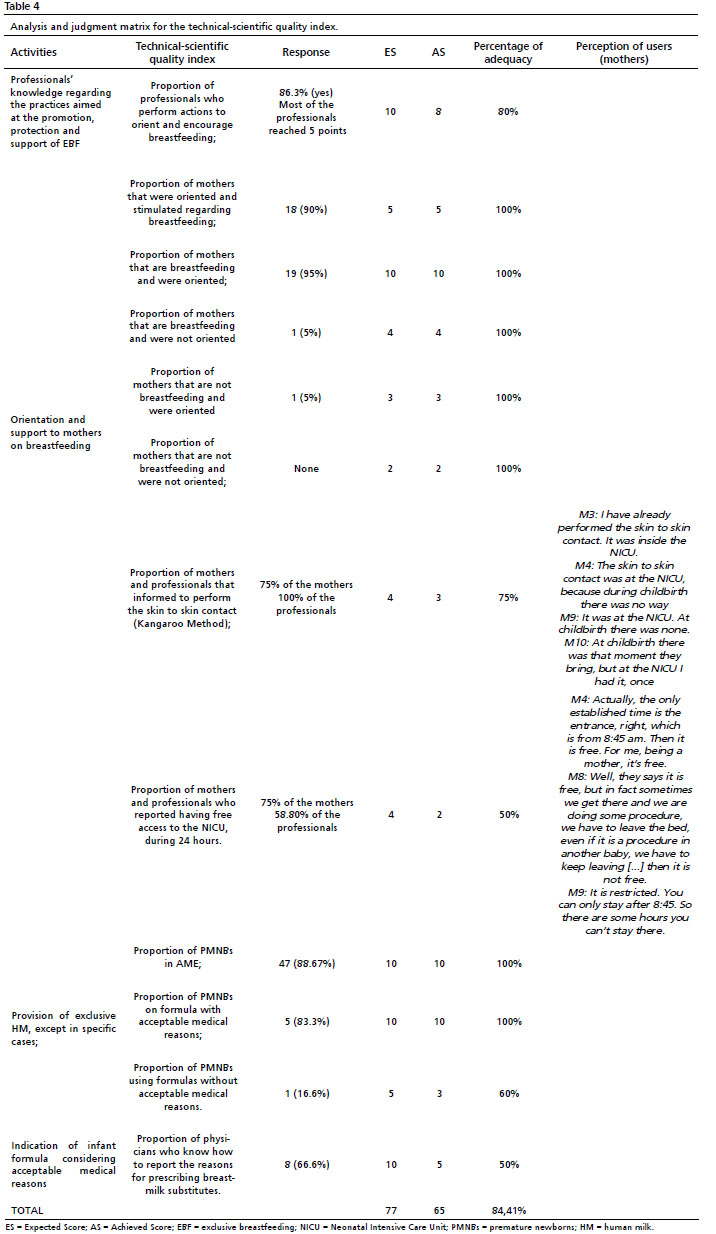
Regarding the characterization of the degree of implementation for the Technical-Scientific Quality index, the process indicators (activities component) were taken into account, as shown in Table 4.
The implementation of the activity component was 84.4%, being considered adequate. Only two items presented values ≤50% of adequacy.
Free access to the NICU was reported by 75% of the mothers and 58.8% of the health professionals, showing divergences between the answers.
Of the main reasons for prescribing infant formula in the NICU, physicians reported the lack of milk in the HMB and the pathologies that preclude the use as intolerance, inborn error of metabolism, cow's milk protein allergy and surgical NB; 66.7% were able to report at least three acceptable medical reasons for the use of formula.
The high volume of HM demanded per child was reported as one of the reasons for prescribing infant formula and one of the main difficulties in prescribing HM from HMB, in addition to staff misinformation, lack of guidance in management and durability of milk (8.3% each).
The predominant nutritional therapy throughout hospitalization was exclusive breast milk/HM, totaling 88.6%.
Regarding infrastructure, the unit provided eight beds for the mothers to stay in the unit for 24 hours and food during hospitalization. However, the lack of beds available for mothers accounted for 75% of the difficulties in staying in the unit full time for 24 hours. The place for milking (inside the NICU) was assessed as great by 55% of the mothers, and the main complaint was about privacy (66.6%).
Regarding feeding, 45% of the mothers reported it as optimal, 35% good and 20% poor. In the reports, optimal feeding was associated as being healthy, balanced, rich, and distributed at regular times. Bad eating was associated with little variety, appearance, taste, and not following food preferences.
The support of health professionals for breastfeeding was reported by 90% of the mothers. The most predominant form of help was information associated with practical help (77.3%), where the professional orients the mother verbally and helps her place the premature baby in the breast. Among the guidelines received, the extraction techniques accounted for 90%, followed by diet schedules (55%), breast preparation (45%), and the advantages of breastfeeding (40%).
When asked about breastfeeding, 95% were breastfeeding/extracting breast milk; 60% had difficulties in the BF process, especially extracting (50%). As for the aspects that have contributed to the breastfeeding process, 35% reported the importance of milk for the baby's health and 50% reported the support from health professionals and the BLH.
The applicability of public policies in favor of breastfeeding was verified through the practice of skin-to-skin contact, being reported by 100% of professionals and 75% of mothers. This practice is carried out in the unit mainly during the diet (37.25%) and according to the clinical condition/stability of the NB (27.45%).
The unit's breastfeeding policy included the BFHI's ten steps for successful breastfeeding; woman-friendly care; permanence of parents and free access to the NB. The annex also included the acceptable medical reasons for the use of LM substitutes and the NBCAL.
According to the NICU health professionals, the facilitators of breastfeeding premature infants are: staff encouragement and guidance (50.9%); free access/mother's presence (25.4%); Kangaroo Method/skin-to-skin contact (15.9%); mother and child interaction/ bond (11.7%); early initiation/stimulation (7.8%); RN conditions (5.8%); desire of the mother (5.8%); training of professionals (3.9%); correct technique/delivery (3.9%); adequate number of professionals at the NICU (3.9%); more nursing mother beds (1.9%); nipple (1.9%); mother's psychological (1.9%) and baby's readiness (1.9%).
Among the difficulties in BF, the professionals highlighted: clinical conditions of the NB (25.4%); absence of the mother (23.5%); lack of guidance/stimulus/support of professionals (19.6%); emotional stress/fear/anxiety/insecurity of mothers (17.6%); lack of information (13.7%); lack of structure/nursing mother beds (7.8%); lack of bonding of the binomial (3.9%). The others represented only 1.9%, and they were: lack of skin-to-skin contact; resistance of the team to wake the baby; length of hospitalization; low production; lack of privacy and maintenance of lactation.
DiscussionDespite the high degree of implementation found and its adequacy according to the parameters established in this research, some aspects that were not adequate and are related to the external and organizational context may compromise the proper implementation of the intervention.
Regarding the external context, the facilities in the breastfeeding process found in this study were related to the mother's age group, education, marital status, availability of a support network, and the mothers' knowledge about the importance of milk for the baby. The study by Moura
et al.
17 showed that the recognition of the advantages of LM for the premature baby was the main reason given by mothers for breastfeeding their babies, even in the face of various situations of insecurity, discomfort, and discomfort experienced by them in the context of hospitalization.
With regard to the mother's level of education, many studies have shown that this factor affects the motivation to breastfeed. Mothers with a higher level of education tend to breastfeed for longer, perhaps because of the possibility of greater access to information about the advantages of breastfeeding.
18 Moreover, most were in a stable union. This result is positive, since the support of a partner has a statistically positive relationship with the maintenance and duration of breastfeeding.
19Industry marketing was described as a hindering factor in the breastfeeding process evidenced in the external context. Some professionals reported feeling pressured by marketing companies to prescribe infant formula.
A study conducted in eight countries by WHO showed that health professionals were reported as the main source of education on infant feeding practices, influencing the decision about breastfeeding. Thus, the systematic marketing of infant formula companies seeks to influence health professionals' understanding of BF, convince them of the need for formulas, and use them as marketing channels.
20Regarding the Organizational Context, the presence of LH and of the fortifier is essential for the supply to occur in an exclusive way, ensuring better development and ponderal gain of PIs.
1 In this study, the LH stocks were stocked, but babies with high volumes what are babies with high volumes? (> 30ml/hour) tend to receive formula routinely, which can be corroborated with the justifications of the NICU physicians. This shows that, even though LH is present, it is not supplied in sufficient quantity, constantly, for all PIs.
In very low birth weight PIs, the use of fortificants provides increased growth and weight gain rates.
21 However, in the absence of fortificants, premature formulas are used and can be interspersed with HL.
22 Therefore, the lack of fortificants in the unit may compromise the exclusive supply of HL, favoring the increased use of formulas.
According to the global standards and the Compliance Criteria related to the Exclusive Supply of LM to Infants described in the BFHI strategy, the observation of the neonatal ward should confirm that at least 80% of the babies are being fed only LM or BLH milk, or, if they received something else, it was for acceptable medical reasons.
15 Thus, the results of this study show that the supply of LH is in accordance with what is established by the BFHI.
Research has shown that, although it may vary according to the social and cultural contexts in which the woman is inserted, formal support from professionals positively influences the initiation and duration of breastfeeding, and practical help seems to be the most effective means for health professionals to support breastfeeding.
23The presence of beds for mothers of PIs enables their permanence in the unit, favoring the provision of LH for the baby. However, the number of beds was not sufficient to meet all mothers of PIs, a factor that compromised the implementation of the structural input component.
In the study by Uema
et al. ,
24 professionals reported that the lack of infrastructure in the neonatal unit is partly responsible for the failure of breastfeeding. The lack of accommodations and the mother's difficulty in staying in the unit were also pointed out as decisive factors by these authors, which reinforces the need for attention to this aspect by HMIB. Thus, the presence of a room with beds for mothers in proportion to the number of NICU beds is extremely important for the promotion of breastfeeding in the unit.
The training of health professionals on BFHI was quite significant, where the vast majority had already been trained by the BFHI and were aware of the breastfeeding policy printed in the unit. This can be seen as a positive factor, since studies show a lower rate of adherence to Step 2 of the BFHI (training the entire health care team in the practices necessary to implement this policy).
25 The BFHI course schedule is available annually in the hospital, which takes place every month, with a workload of 20 and 40 hours, and it is recommended that each professional should attend the course at least every five years.
Given the data presented, the main difficulties of the organizational context that interfere in the breastfeeding process are related to the volume of milk coming from the HLB and low stocks, the unit's infrastructure such as the lack of beds available for 24-hour stay, inadequate place for daily mothers to rest in the unit, lack of privacy in the extraction of the HL in the NICU, and the extraction techniques. The study by Gianni
et al.
2 also identified extraction as one of the factors hindering breastfeeding in premature infants.
The facilities identified were support and guidance from NICU and BLH professionals, the presence of LH and fortifier, free access to the NICU, skin-to-skin contact, food provided on site, training of professionals and knowledge of the unit's breastfeeding policy, in addition to the unit being accredited by the BFHI and following the ten steps.
One of the limitations of this study was that it was carried out during the pandemic of COVID-19, which made it difficult to apply the data collection instrument and indirectly affected the stocks of HL, since mothers did not go to the unit for the donation of HL and even those with their PIs admitted to the NICU did not stay daily in the unit for extraction.
Given this scenario, we chose to apply the instrument with health professionals in order to reach a larger number of them, which proved to be right considering that there were 51 respondents. This instrument, however, had limitations, since interviews would have provided more in-depth information on the provision of LH.
The supply of LH to preterm infants was satisfactory, and breastfeeding was possible for most preterm infants, despite the challenges inherent to prematurity. The fact that preterm infants were admitted to a child-friendly hospital was a contributing factor to the implementation of the intervention. Thus, it can be considered that success in breastfeeding practices is influenced by public policies.
Health service evaluations, developed with the involvement of users and health professionals, are an important tool in identifying weaknesses in order to seek improvements in the implementation of services. Within this context, knowing the experience of mothers, professionals, and the organization of the institution's work regarding the provision of LH during hospitalization is essential for the promotion of interventions that favor the health of women, children, family, and society.
References1. Lima APE, Castral TC, Leal LP, Javorski M, Sette GCS, Scochi CGS,
et al. Aleitamento materno exclusivo de prematuros e motivos para sua interrupção no primeiro mês pós-alta hospitalar. Rev Gaúcha Enferm. (Porto Alegre) 2019; 40: 8.
2. Gianni ML, Bezze EN, Sannino P, Baro M, Roggero P, Muscolo S,
et al. Maternal views on facilitators of and barriers to breastfeeding preterm infants. BMC Pediatrics. 2018; 18 (238): 7.
3. World Health Organization (WHO). Guideline: protecting, promoting and supporting breastfeeding in facilities providing maternity and newborn services. Geneva: WHO; 2017. [access in 2022 mar 5]. Available from:
https://www.who.int/publications/i/item/97892415500864. Gomes ALM, Balaminut T, López SB, Pontes KAES, Scochi CGS, Christoffel MM. Aleitamento materno de prematuros em hospital amigo da criança: da alta hospitalar ao domicílio. Rev Rene. 2017; 18 (6): 810-7.
5. Brasil. Lei n°. 11265, de 3 de janeiro de 2006. Regulamenta a comercialização de alimentos para lactentes e crianças de primeira infância e também a de produtos de puericultura correlatos. Brasília (DF): DOU de 4 jan 2006. [access in 2020 jun 8]. Available from::
https://www.planalto.gov.br/ccivil_03/_ato2004-2006/2006/lei/l11265.htm6. Ministério da Saúde (BR). Gabinete do Ministro. Portaria nº 930, de 10 de maio de 2012. Define as diretrizes e objetivos para a organização da atenção integral e humanizada ao recém-nascido grave ou potencialmente grave e os critérios de classificação e habilitação de leitos de Unidade Neonatal no âmbito do Sistema Único de Saúde (SUS). [access in 2020 ago 30]. Available from:
https://bvsms.saude.gov.br/bvs/saudelegis/gm/2012/prt0930_10_05_2012.html#:~:text=Define%20as%20diretrizes%20e%20objetivos,%C3%9Anico%20de%20Sa%C3%BAde%20(SUS).
7. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Bases para a discussão da Política Nacional de Promoção, Proteção e Apoio ao Aleitamento Materno Brasília (BR): Ministério da Saúde, 2017. [access in 2020 ago 17]. Available from::
https://bvsms.saude.gov.br/bvs/publicacoes/bases_discussao_politica_aleitamento_materno.pdf8. Nyqvist KH, Häggkvist AP, Hansen MN, Kylberg E, Frandsen AL, Maastrup R,
et al. Expansion of the Ten Steps to Successful Breastfeeding into Neonatal Intensive Care: Expert Group Recommendations for Three Guiding Principles. J Hum Lact. 2012 Aug; 28 (3): 289-96.
9. Bujold M, Feeley N, Axelin A, Cinquino C, Dowling D, Thibeau S. Expressing human milk in the NICU. Adv Neonatal Care, 2018; 18 (1): 38-48.
10. Cruz MR, Sebastião LT. Amamentação em prematuros: conhecimentos, sentimentos e vivências das mães. Distúrbios Comun. (São Paulo) 2015; 27 (1): 76-84.
11. Benoit B, Semenic S. Barriers and Facilitators to Implementing the Baby-Friendly Hospital Initiative in Neonatal Intensive Care Units. JOGNN, 2014; 43 (5): 614-24.
12. Oliveira AEF, Reis RS. Gestão pública em saúde: os desafios da avaliação em saúde. São Luís: Edufma, 2016. 57 p. [access in 2022 nov 14]. Available from:
https://ares.unasus.gov.br/acervo/html/ARES/7411/1/GP5U2.pdf13. Hartz ZMA. Avaliação em Saúde: dos modelos conceituais à prática na análise da implantação de programas [
online]. Rio de Janeiro: Editora FIOCRUZ; 1997. [access in 2022 nov 14]. Available from:
https://books.scielo.org/id/3zcft14. Moura R. Bancos de leite do DF viram referência para os Brics. Rio de Janeiro (RJ): Fiocruz; 2019. [access in 2020 jul 2]. Available from:
https://rblh.fiocruz.br/bancos-de-leite-do-df-viram-referencia-para-os-brics15. Fundo das Nações Unidas para a Infância, Organização Mundial da Saúde (OMS). Iniciativa Hospital Amigo da Criança: revista, atualizada e ampliada para o cuidado integrado. Módulo 2: fortalecendo e sustentando a iniciativa hospital amigo da criança: um curso para gestores. Brasília (DF): Ministério da Saúde; 2009. [access in 2020 jul 2]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/iniciativa_hospital_amigo_crianca_modulo2.pdf16. Souza JR, Santos SCM. Análise de conteúdo em pesquisa qualitativa: modo de pensar e de fazer. Pesq Debate Educ. 2020; 10 (2): 1396-1416.
17. Moura LP, Oliveira JM, Noronha DD, Ribeiro JD, Torres V, Oliveira KCF,
et al. Percepção de mães cadastradas em uma Estratégia Saúde da Família sobre aleitamento materno exclusivo. Rev Enferm UFPE. 2017; 11 (Supl. 3): 1403-9.
18. Muller FS, Silva IA. Representações sociais de um grupo de mulheres/nutrizes sobre o apoio à amamentação. Rev Latino-am Enferm. 2009; 17 (5): 8.
19. Santiago LA, Hissayassu SAY, Comuni PMD. Principais Fatores de Risco para a Manutenção do Aleitamento Materno Exclusivo no Brasil e EUA. Rev Contexto Saúde. 2019; 19 (37): 11-9.
20. World Health Organization (WHO). How the marketing of formula milk influences our decisions on infant feeding; 2022. [access in 2022 nov 14]. Available from:
https://www.who.int/publications/i/item/978924004460921. Filho JVB, Pereira RJ, Castro JGD. Efeitos do uso de fortificante do leite humano em recém-nascidos pré-termo de muito baixo peso. Ciênc Cuid Saúde. 2016; 15 (3): 429-35.
22. Gonçalves AB, Jorge SM, Gonçalves AL. Comparação entre duas dietas à base de leite humano em relação ao crescimento e à mineralização óssea de recém-nascidos de muito baixo peso. Rev Paul Pediatr. 2009; 27 (4): 395-401.
23. Pinto SL, Barruffini ACC, Silva VO, Ramos JEP, Junqueira IC, Borges LL,
et al. Avaliação da autoeficácia para amamentação e seus fatores associados em puérperas assistidas no sistema público de saúde no Brasil. Rev Bras Saúde Mater Infant. 2021; 21 (1): 97-105.
24. Uema RTB, Tacla MTGM, Zani AV, Souza SNDH, Rossetto G, Santos JCT. Insucesso na amamentação do prematuro: alegações da equipe. Semina Ciênc Biol Saúde. 2015; 36 (1): 199-208.
25. Jesus PC, Oliveira MIC, Fonseca SC. Repercussão da capacitação de profissionais de saúde em aleitamento materno sobre seus conhecimentos, habilidades e práticas hospitalares: uma revisão sistemática. J Pediatr (Rio J. ) 2016; 92 (5): 436-50.
26. Gaíva MA, Scochi CGS. A participação da família no cuidado ao prematuro em UTI Neonatal. Rev Bras Enferm. 2005; 58 (4): 444-8.
27. Serra SOA, Scochi CGS. Dificuldades maternas no processo de aleitamento materno de prematuros em uma UTI neonatal. Rev Latino-Am Enferm. 2004; 12 (4): 597-605.
Received on June 24, 2022
Final version presented on December 14, 2022
Approved on December 31, 2022
Associated Editor: Luciana Dubeux
Acknowledgments: To the professional master's degree in health evaluation at ENSP/Fiocruz and to the professionals, managers, and users of HMIB involved in the research.
Authors' contribution: Reis MMP: data collection and analysis, interpretation, and initial draft of the manuscript. Barros DC and Vitorino SAS: study design and coordination, and critical revision of the manuscript. All authors approved the final version of the article and declare no conflict of interest.


 ; Denise Cavalcante Barros2
; Denise Cavalcante Barros2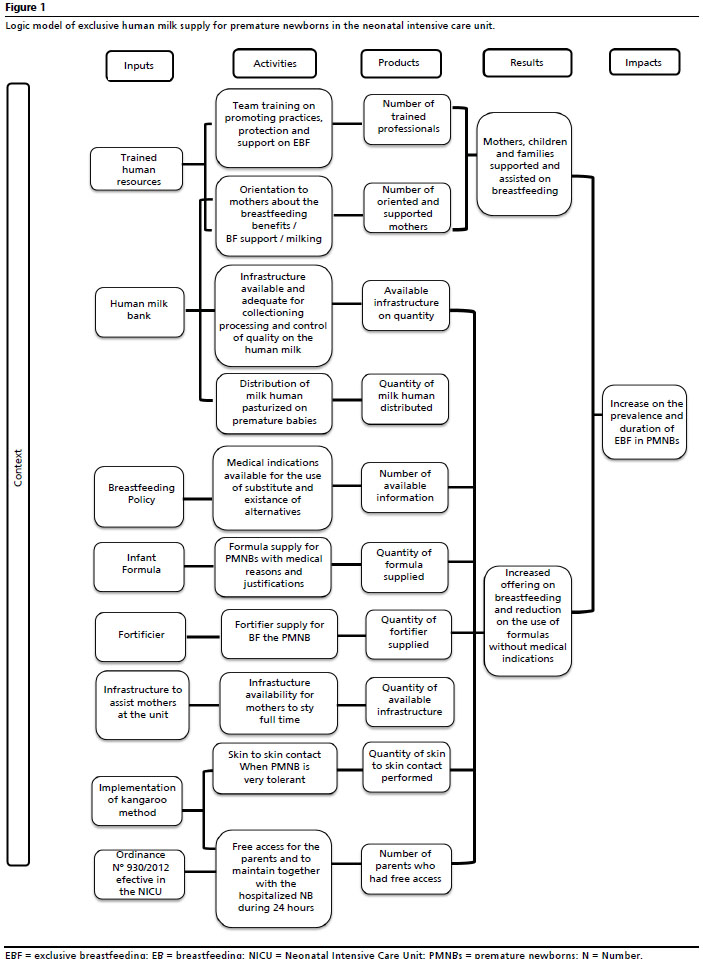







 Ler em português
Ler em português