ABSTRACT
OBJECTIVES: to identify puerperal women's knowledge attending the housing unit at a teaching hospital about newborn body hygiene after receiving routine guidance from the nursing team.
METHODS: cross-sectional study, carried out with 207 puerperal women from a teaching hospital in the Minas Gerais State between December 2018 and May 2019. For data collection, an instrument was built and validated following three phases and descriptive statistics and linear correlation were used of Spearman's, with a confidence level of 95% for knowledge analysis.
RESULTS: 207 puerperal women participated in the study, with a mean age of 27 ± 6.3 years. Inadequate knowledge was observed, mainly regarding the sequence of cleaning the face and scalp, adequate products and hygiene of the nose, ear and mouth. The domain "before the bath" presented the highest average percentage of correct questions (94.0%±10.1), including care with the environment, temperature and intimate hygiene.
CONCLUSION: the identification of inadequate knowledge about the newborn's body hygiene raises the need for constant and more effective guidelines, with the use of active methodologies starting in prenatal care.
Keywords:
Baths, Infant, newborn, Mothers, Knowledge
RESUMO
OBJETIVOS: identificar o conhecimento de puérperas assistidas em uma unidade de alojamento conjunto de um hospital de ensino acerca da higiene corporal do recém-nascido após receberem as orientações de rotina pela equipe de enfermagem.
MÉTODOS: estudo transversal, realizado com puérperas de um hospital de ensino do estado de Minas Gerais entre dezembro de 2018 e maio de 2019. Para coleta de dados foi construído e validado um instrumento seguindo três fases e empregou-se a estatística descritiva e a correlação linear de Spearman´s, com nível de confiança de 95% para análise do conhecimento.
RESULTADOS: participaram do estudo 207 puérperas, com média da idade de 27 ±6,3 anos. Conhecimentos inadequados foram observados, principalmente quanto à sequência da limpeza da face e couro cabeludo, produtos adequados e higiene do nariz, orelha e boca. O domínio "antes do banho" foi o que apresentou o maior percentual médio de questões acertadas (94,0%±10,1), incluiu cuidados com ambiente, temperatura e higiene íntima.
CONCLUSÃO: a identificação de conhecimentos inadequados sobre a higiene corporal do recém nascido suscita a necessidade de orientações constantes e mais efetivas, com uso de metodologias ativas com início no pré-natal.
Palavras-chave:
Banhos, Recém-nascido, Mães, Conhecimento
IntroductionThe newborn's (NB) body hygiene is challenging, perceived as a source of doubt and anxiety, mainly related to the fragility of the baby, the difficulty in how to hold it, reactions to the bath, and the steps to be followed.
1,2 Thenurse, as a health education agent has the role of preparing women to care for the NB and the process of motherhood, offering updated and safe information to care at home.
2The period of prenatal care and to stay in a housing are opportune moments for the incorporation of educational activities, so that the mothers and their families can develop good quality care, however, it is observed in the professional practice that the actions developed in these spaces are fragmented and focused especially on breastfeeding.
3,4 Guidance about bathing in maternity wards was considered superficial by mothers and family members, awakening feelings of insecurity and inability to perform the baths and care for the umbilical stump at home.
3,5It is observed that even though they have received information based on the best evidence by health professionals, the influence of the mothers, mothersin-law, and grandmothers' knowledge, in the young and primiparous women, on the NB's care is remarkable. Inadequate practices are perceived in the family context regarding body hygiene and the umbilical cord.
3,6 Therefore, the affective involvement present in family relationships favors the transmission of intergenerational care and, culturally, parental relationships influence the children's behavior even when they are adults, through trust, respect or authority.
6Then, the personal experiences of each family should be valued by the health professional, so that there is closeness and bonding, however, the risk posed to the NB must be assessed.
6 One must invest in pedagogical approaches that consider the family's reality, aiming at autonomy and safety at home, providing a space for dialogue about the doubts and individual demands.
5Verifying the puerperal women's knowledge about the newborn's body hygiene is a strategy for planning and evaluating the scope of health education on the nursing team. This study aimed to identify the puerperae knowledge assisted in a housing unit in a teaching hospital about the newborn's body hygiene after receiving routine guidance by the nursing staff.
MethodsThis was a cross-sectional study
7 carried out with puerperal women assisted in the H wards in a teaching hospital in Minas Gerais State. Convenience sampling was used, considering the maximization of sample size as a criterion. We adopted the recommendations of the STROBE Statement (Strengthening the Reporting of Observational Studies in Epidemiology Statement) for cross-sectional studies.
Inclusion criteria to participate in the study were: women in the immediate puerperal period, at least 12 hours postpartum; age 18 years or older; received routine guidance from the nursing team about the NB's first bath, whose bath was performed after six hours of life. Puerperae with NBs hospitalized in intermediate or intensive care units were excluded from the study.
The interviews with the puerperae were conducted according to the availability of the participants, on the ward itself, respecting their privacy and individuality, in the period between December 2018 and May 2019. The instrument was applied after 6 to 12 hours of the nursing team's routine orientations.
The construction and validation content of the instrument for the knowledge assessment of about the puerperal women NB's body hygiene was performed, following the three phases of the elaboration of the measurement instrument: theoretical (construc from the construction, including item development and validity content), empirical (techniques for applying the pre-test or semantic analysis), and analytical (statistical analyses).
8 The final version of the instrument contains 30 questions about knowledge of the NB's body hygiene, with yes (correct knowledge) and no (incorrect knowledge) answer options, and one open question, divided into six domains: before bathing, during bathing, after bathing, general care, and attitudes about bathing the baby (Figure 1). The construct was developed based on the literature survey conducted in August 2018.
Nine nurse-doctoral judges participated in the validation content process, in three rounds of evaluation to adjust the suggestions and obtain agreement by the
Índice de Validade de Conteúdo (Content Validity Index) above 80% of all items. After changes, semantic validation was performed for the adequacy of intelligibility with six puerperae from different extracts (Figure 1).
The data were stored in a database in Excel
® format, by double entry for later validation. Then imported into the Statistical Package for Social Sciences (SPSS) version
21.0 for processing and analysis. The categorical variables were analyzed from absolute and percentage frequencies and the numerical variables from measurements of centrality and dispersion. The variable knowledge about NB's hygiene was subjected to a descriptive analysis from the determination of the absolute quantity and percentage of puerperae who answered correctly or incorrectly each question. In addition, for this variable the percentage of questions answered correctly in each domain was calculated for each puerpera and analyzed from the mean and standard deviation. In each domain, the correlation between the percentage of questions answered correctly and the socio-demographic variables was verified using Spearman's linear correlation coefficient. The significance level of inferential procedures was 5%.
The research was approved in 2018 by the Research Ethics Committee of the
Universidade Federal do Triângulo Mineiro, under the opinion no. 2,944,893. CAAE: 94273018.6.0000.8667
ResultsA total of 207 puerperae participated in the study, with a mean age of 27 ± 6.3 years. Regarding the sociodemographic profile it was found that 143 (69.1%) of the puerperae had a partner, 73 (35.3%) had completed high school, 04 (1.9%) had higher education, with a minimum time of study of 02 (4.1%) ±3.3 years and 139 (67.1%) had a paid job (Table 1).
As for the obstetric profile, it was observed that 59 (28.5%) were primiparous and 148 (71.5%) were multiparous, with a mean of 2.0±1.2 children. In the current pregnancy all NB were term and one (0.4%) puerpera had twin pregnancy. Regarding the family support network, 188 (90.8%) mentioned that they would have someone to help with the baby care at home, and the puerpera's mother was the person most often mentioned. All of them had prenatal care, with a mean of 8.0±3.1 consultations (Table 1).
When asked whether they had received information on thebaby's hygiene care and bathing of the during of prenatal care, only 15% of puerperae reported having received guidance. As for the professionals' responsibilties for the information in the basic health unit, 27 (13%) indicated the nursing team and 04 (2%) the medical team. Among the main information received, both prenatally and in the maternity unit, the most cited were: care with water temperature, positioning of the baby, bath sequence, cleaning the umbilical stump, number of daily baths, and used of products such as soap and perfume.
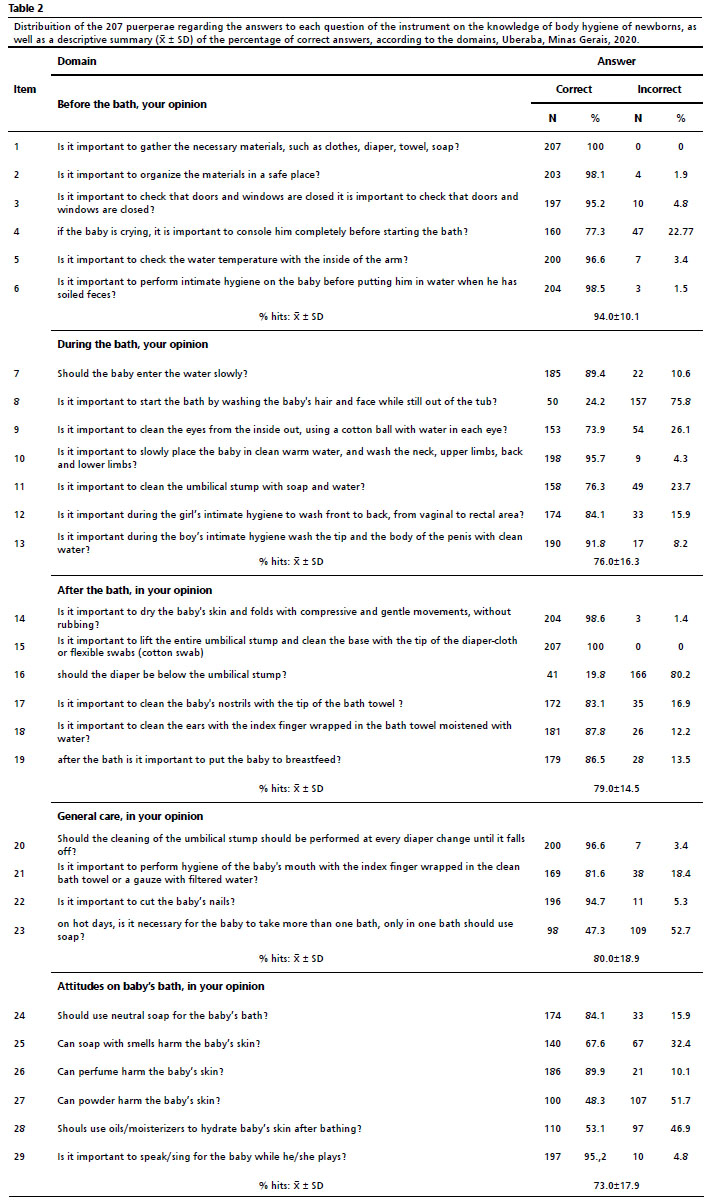
In the knowledge assessment, most of the questions (79.3%) had more than 70% of correct answers. The domain "before bathing" was the one with the highest average percentage of correct answers (94.0% ± 10.1). All puerperae answered corretly the question about the organization of materials and preparation of the bath, and 77.3% (160) puerperae answered right the question about whether the baby should be comforted when crying.
In the domain "during the bath", less than half of the puerperae (24.2%) knew that it was important to wash the face and scalp before putting the baby in the tub, and in the domain "after the bath", 41 puerperae (19.8%) knew that they should close the diaper below the umbilical stump. In the domain about general care, 109 puerperae (47.3%) were correct in stating that if it was necessary for the baby to take more than one bath a day, they would use soap in all of them. In the domain "attitudes about bathing the newborn," 186 (89.9%) were correct in believing that perfume can harm the newborn's skin and 174 (84.1%) were correct in saying that they would use mild soap (Table 2).

Question 30 "What should be applied and or placed on top of the umbilical stump after leaving the hospital?" from the last domain, after grouping, obtained four types of answers: cleaning with alcohol, swab and gauze 20 (9.7%); cleaning with alcohol only or gauze only 173 (83.6%), use of bandage 12 (5.8%) and use of olive oil 2 (1%).
The percentage of correct answers for each domain when compared to the sociodemographic variables did not show a strong correlation (
p>0.005). Age, dichotomized in <25 years and >25 years, when associated with the percentage of correct answers in the general care domain showed a value of
p=0.005, those >25 years had 76.1% of correct answers, representing 154 (74.3%) of the sample, showing the influence of this variable on the knowledge of these puerperae.
DiscussionThe present study found a predominance of young women, with a partner, multiparous, and who had attended elementary and high school, characteristics similar to other studies.
9,10 Puerperae demonstrated to have adequate knowledge about bathing the newborn, especially in the domain before the bath. The sequence of cleaning the face and scalp, appropriate products and hygiene of the nose, ear and mouth showed higher percentages of incorrect answers.
In this study, there was a significant association of age with the domain general care, which included hygiene of the mouth, nose, ear, umbilical stump, and soap use, showing the influence of this variable on knowledge of puerperae who were over 25 years old. Young and primiparous mothers are often influenced by family knowledge, following empirical traditions.
1,3-4 By forgetfulness due to the little dirt, fear of touching, with the umbilical stump, or lack of knowledge, these cares are omitted at bath time. It is believed that the performance of this care with greater autonomy and safety depends on the guidance received during pregnancy and puerperium.
11Most of the puerperal women reported that they would have someone to help them take care of the baby at home, a relevant aspect in the group studied, since dysfunctional and unsupported family dynamics are risk factors for the development of postpartum depression, difficulties in breastfeeding, and mother-baby bond.
12Educational activities on hygiene care with newborns are part of prenatal care, however, only 31 (15%) said they had received this information during this period. It is observed that the intervention strategies developed in prenatal care for the newborn focus on breastfeeding.
13Fragilities in maternal preparation are identified in the literature, mothers report that they did not have the opportunity to give or observe the bath in the hospital and at home they had difficulties when they found themselves alone. The complaints increased in mothers of low birth weight NBs, preterm and twins, where hospitalization in neonatal units is almost always necessary due to physiological immaturity. The separation of the binomial, added to the lack of structure for maternal permanence are barriers in the guidance of neonate's care.
14 The maternal preparation with the possibility of clarifying doubts and demonstrating practical skills at different times minimized the insecurities to perform the care at home and made practice safer.
15In the domain "before bathing", puerperae showed adequate knowledge. Studies evaluating the puerperae knowledge who stayed at housing found similar results.
16,17 The bath time, besides hygiene, is important for the baby's relaxation and to build a bond between the binomial. The crying can trigger or potentiate distressing feelings, as it makes mothers worried that they are doing something wrong that is hurting their child.
18 Therefore, it is recommended to calm the baby before putting him/her in the water, meeting his/her needs.
11In the domain "during bathing", most puerperae (71.5%) indicated that it is not important to start the bath by the face and scalp. However, it is recommended that the face be cleaned before placing the NB in the water, so that the face is not washed after the bathtub water contains soap and, also, so that it adapts to the water temperature and that the scalp hygiene is performed before bathing, or at the end, avoiding the loss of heat, caused by exposure of the cephalic segment to evaporation for a prolonged time.
19 Wrapping the NB in a cloth diaper during facial and scalp hygiene minimizes the effects of heat loss and contributes to the state of relaxation and minimizes handling reactions such as stress, crying, and agitation, the so-called humanized bath.
20 This technique is familiar in the care of premature NB, but it is recommended for all NB and should be encouraged by the nursing team.
21When cleaning the umbilical stump during the bath, few puerperae (14.9%) reported that there was no need and that it was only important to apply 70% alcohol. The application of alcoholic substances should be associated with correct washing for effective protection.
22 In this study, cultural practices were mentioned to a lesser extent, such as the use of olive oil and the use of a cloth diaper covering the periumbilical region. In the domain "after bathing", most (75.9%) believe that the cloth diaper should cover the umbilical stump, contrary to the recommendations for proper healing.
22Cleaning ears and nostrils was considered important among puerperal women, however, when asked if it should be done with the tip of the towel-diaper, they mentioned that they would use cotton swabs. A study evaluating the knowledge of pregnant women about baby care identified the fear of getting water in the ear and nose during bathing, but did not address the issue of cleaning.
10The domain "general care" included routine care and use of products. As for the NB's oral hygiene, some puerperae (13.5%) responded that they did not know the importance or did not know that it should be performed with gauze and filtered water. Similar results were found in a study carried out with Portuguese mothers.
23About the number of daily baths and soap use, it is known that in tropical climates, such as in Brazil, the newborn is allowed to take more than one bath a day, without harming the skin condition, as long as soap is used in only one of them. Excessive use of soap may cause irritation and increased sensitivity.
2About the use of soap, powder and perfumes after bathing, puerperal women believe that it is important to use neutral soap and that soaps with fragrance, perfumes and powder can harm the NB's skin. Some infant products contain inappropriate and toxic substances, so one should avoid those containing perfume, dye, alkaline pH, and aggressive surfactants. The application of substances in powder form is not indicated because of the risk of accidental inhalation, triggering other aggravating factors.
24Skin care, such as cleaning and drying without rubbing and not removing the caseous vernix, should be reinforced during orientation in order to preserve skin integrity to avoid possible irritation and physical, chemical, mechanical aggression and infection. In general, neonates have greater vulnerability and risk of skin aggression, which is more accentuated in premature babies.
19,21Excessive handling during bathing can produce several reactions in newborns, especially in preterm infants, such as stress, withdrawal behavior, crying, increased or decreased saturation, and hypothermia. Thus, care with the bath must consider the gestational age, weight, and clinical conditions of the neonates. For those admitted to Neonatal Intensive Care Units, hygiene should be restricted to the eye, oral cavity, and perineum.
21Proper care of the NB's body hygiene is essential for lower risk of infection, less skin barrier breakdown and reduction of a disorganized behavioral state. The mother as the main promoter of this care should be encouraged and guided based on the best available evidence, being the competence of health professionals, especially nurses in this context, the constant updating and training of the team. Studies that provide situational diagnosis of maternal frailties contribute to improve care, directing the health actions of the nursing team and allow the elaboration of institutional protocols and public policies aimed at the real needs of this public.
25As a limitation in this study, we consider the fact that the validated instrument evaluates the knowledge in hits (yes) and misses (no), which made it impossible to create scores and the fact that the time between the orientations and the interview was not evaluated, which may generate a recall bias in the answers.
It was concluded that puerperal women had adequate knowledge about the issues of the NB's body hygiene in all domains investigated, which suggests a good evaluation of the guidance provided by the nursing staff of the unit evaluated. Inadequate knowledge was observed, especially regarding the sequence of cleaning the face and scalp, appropriate products and hygiene of the nose, ear and mouth.
The investigation of care from the maternal perspective allowed us to assess the guidance provided, identify the gaps to be repaired, and offer subsidies to guide the planning of maternal preparation during prenatal and housing.
We emphasize the need for constant and more effective guidance, with the use of active methodologiesrelated to newborn's bathing. In addition, the beginning of the preparation for these practices should occur in the prenatal period, so that there is time for puerperal women to clarify doubts and feel safer when performing this care.
Referências1. Vasconcelos ML, Pessoa VLMP, Chaves EMC, Pitombeira MGV, Moreira TM, Cruz MR,
et al. Cuidado à criança menor de seis meses no domicílio: experiência da mãe primípara. Esc Anna Nery. 2019; 23 (3): e20180175.
2. Sousa LB, Braga HFGM, Alencastro ASA, Silva MJND, Oliveira BSB, Santos LVFD,
et al. Effect of educational video on newborn care for the knowledge of pregnant and postpartum women and their families. Rev Bras Enferm. 2021; 75 (Suppl. 2): e20201371.
3. Queiroz VC, Andrade SSC, César ESR, Brito KKG, Costa CBA, Oliveira SHS. Conhecimentos, atitudes e práticas sobre aleitamento materno entre puérperas em alojamento conjunto. Rev Enferm. Centro-Oeste Mineiro. 2021; 11: e4162.
4. Simsek A, Balkan E, Caliskan E. Determination of mothers’ thoughts and adaptation behaviors regarding the infant: A descriptive study. Pediatr Neonatol. 2022 May; 63 (3): 276-82.
5 Duarte FCP, Góes FGB, Rocha ALA, Ferraz JAN, Moraes JRMM, Silva LF. Preparo de alta para o cuidado domiciliar de recém-nascidos de baixo risco. Rev Enferm UERJ. 2019; 27: e38523.
6. Silva CS, Carneiro MNF. Pais pela primeira vez: aquisição de competências parentais. Acta Paul Enferm. 2018; 31(4): 366-73.
7. Polit DF, Beck CT. Fundamentos de pesquisa em enfermagem: avaliação de evidências para a prática da enfermagem. 9ª ed. Porto Alegre: Artmed; 2019.
8. Pasquali L. Instrumentação psicológica: Fundamentos e práticas. Porto Alegre: Artmed; 2010.
9. Furlan BG, Araujo JP, Lago MTG, Pinto KRTF, Ferrari RAP, Zani AV. Newborn care and guidance to postpartum women in rooming-in. RSD. 2021; 10 (16): e547101624065.
10. Dias EG, Novaes CCM, Santos IR, Silva SX, Alves JCS. Conhecimento de gestantes de uma unidade de saúde sobre os cuidados com o recém-nascido. Rev Inova Saúde. 2019; 9 (1): 176-90.
11. Lima RO, Estevam LD, Leite FMC, Almeida MVS, Nascimento L, Amorim MHC,
et al. Intervenção de enfermagem-primeiro banho do recém-nascido: estudo randomizado sobre o comportamento neonatal. Acta Paul Enferm. 2020; 33: e-APE20190031.
12. Kazal HR, Flanagan PJ, Mello MJ, Monteiro K, Goldman RE. Birth Stories, Support, and Perinatal Emotional Health among Minority Adolescent Mothers: A Mixed Methods Study. J Pediatr Adolesc Gynecol. 2021 Dec; 34 (6): 847-56.
13. McCarter D, Law AA, Cabullo H, Pinto K. Scoping Review of Postpartum Discharge Education Provided by Nurses. J Obstet Gynecol Neonatal Nurs. 2022 Jul; 51 (4): 377-87.
14. Silva RMM, Zilly A, Toninato APC, Pancieri L, Furtado MCC, Mello DF. Vulnerabilidades para a criança prematura: contextos domiciliar e institucional. Rev Bras Enferm. 2020; 73 (Supl. 4): e20190218.
15. Priyadarshi M, Balachander B, Gupta S, Sankar MJ. Timing of first bath in term healthy newborns: A systematic review. J Glob Health. 2022 Aug; 12: 12004.
16. Ayete-Nyampong J, Udofia EA. Assessment of knowledge and quality of essential newborn care practices in La Dade Kotopon Municipality, Ghana. PLoS One. 2020 Aug; 15 (8): e0237820.
17. Singh DR, Harvey CM, Bohara P, Nath D, Singh S, Szabo S, Karki K. Factors associated with newborn care knowledge and practices in the upper Himalayas. PLoS One. 2019 Sep; 14 (9): e0222582.
18. Liang YC, Wijaya I, Yang MT, Cuevas Juarez JR, Chang HT. Deep Learning for Infant Cry Recognition. Int J Environ Res Public Health. 2022 May; 19 (10): 6311.
19. Freitas P, Munhoz MMB, Costa P, Kimura AF. Efeito de duas técnicas de banho de imersão na temperatura axilar de recém-nascidos pré-termos: estudo piloto. Texto Contexto Enferm. 2018; 27 (1): e0580016.
20. Çaka SY, Gözen D. Effects of swaddled and traditional tub bathing methods on crying and physiological responses of newborns. J Spec Pediatr Nurs. 2018 Jan; 23 (1).
21. Ministério da Saúde (BR). Atenção humanizada ao recém-nascido: Método Canguru: manual técnico. Brasília (DF): Ministério da Saúde; 2017 3ª ed. [acesso em 2022 mar 16]. Disponível em:
https://bvsms.saude.gov.br/bvs/publicacoes/atencao_humanizada_metodo_canguru_manual_3ed.pdf.
22. Kadiroğlu T, Güdücü Tüfekci F. Effect of Infant Care Training on Maternal Bonding, Motherhood Self-Efficacy, and Self-Confidence in Mothers of Preterm Newborns. Matern Child Health J. 2022 Jan; 26 (1): 131-8.
23. Cardoso AMR, Marín HF. Lacunas de conhecimentos e habilidades de mães portuguesas associados à saúde do recém-nascido. Rev Latino-Am Enferm. 2018; 26: e2997.
24. Blume-Peytavi U, Lavender T, Jenerowicz D, Ryumina I, Stalder JF, Torrelo A,
et al. Recommendations from a European Roundtable Meeting on Best Practice Healthy Infant Skin Care. Pediatr Dermatol. 2016; 33 (3): 311-21.
25. Rodrigues VCC, Lopes GF, Silveira GEL, Sousa IB, Sena MM, Lopes TSS,
et al. Fatores associados ao conhecimento e atitude de adolescentes quanto ao uso de preservativo masculino. Rev Bras Enferm. 2021; 74 (Supl. 4): e20190452.
Received on May 25, 2021
Final version approved on November 16, 2022
Approved on December 12, 2022
Associated Editor: Leila Katz
Authors' contribution: Silva MPC, Fonseca LMM, Ruiz MT, Rocha JBA, Contim D: conception, analysis, interpretation of results, writing and critical revision of the manuscript. Araújo GP: conception, analysis, interpretation of results, critical revision of the manuscript. All authors approved the final version of the article and declare no conflict of interest.


 ; Luciana Mara Monti Fonseca2
; Luciana Mara Monti Fonseca2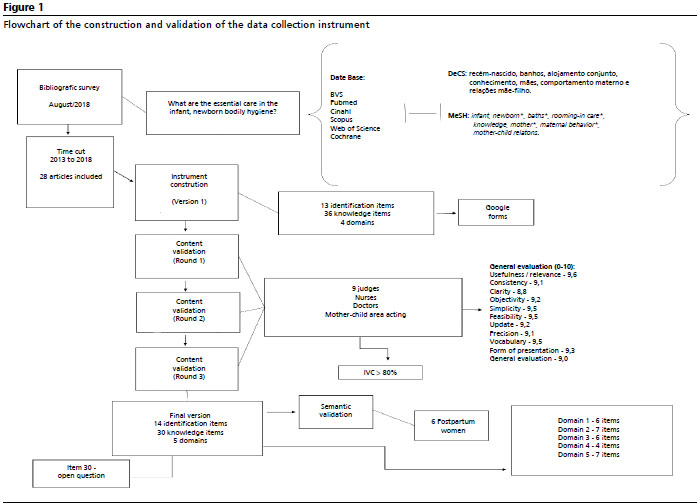







 Ler em português
Ler em português