ABSTRACT
OBJECTIVES: to estimate the prevalence of perceived stress and verify the associated factors in pregnant women assisted by Family Health teams in Montes Claros, Minas Gerais - Brazil.
METHODS: epidemiological, cross-sectional, and analytical study, nested in a population-based cohort. Sociodemographic and obstetric characteristics and physical and mental health conditions were assessed. The stress level was estimated by the Perceived Stress Scale (PSS-14). Descriptive and bivariate analyses were conducted, followed by the Poisson Regression model with robust variance.
RESULTS: a total of 1,279 pregnant women participated. The prevalence of high-stress levels was 23.5% (CI95%=20.8%-26.2%). The outcome was more prevalent among pregnant women aged above 35 years (PR=1.38; CI95%=1.09-1.74) and less than or equal to 19 (PR=1.41; CI95%=1.13-1.77); without a partner (PR=1.33; CI95%=1.09-1.62); with low social support (PR=1.42; CI95%=1.181.70); multiparous (PR=1.30; CI95%=1.02-1.66); with current unplanned pregnancy (PR=1.23; CI95%=1.00-1.52); urinary tract infection (PR=1.35; CI95%=1.12-1.62); high level of anxiety symptoms (PR=1.42; CI95%=1.18-1.71); severe (PR=4.74; CI95%=3.60-6.26) and moderate (PR=3.19; CI95%=2.31-4.39) symptoms of depression; and neurological complaints (PR=1.77; CI95%=1.27-2.47).
CONCLUSION: there was a significant prevalence of high perceived stress among pregnant women, an outcome associated with sociodemographic, clinical, obstetric, and emotional factors, which demonstrates the need for comprehensive care of pregnant women's health.
Keywords:
Pregnancy, Pregnant women, Stress psychological, Primary health care, Health surveys
RESUMO
OBJETIVOS: estimar a prevalência de estresse percebido e verificar os fatores associados em gestantes assistidas por equipes da Saúde da Família de Montes Claros, Minas Gerais - Brasil.
MÉTODOS: estudo epidemiológico, transversal e analítico, aninhado a uma coorte de base populacional. Avaliaram-se características sociodemográficas, obstétricas, condições de saúde física e mental. O nível de estresse foi estimado pela Escala de Estresse Percebido (Perceveid Stress Scale, PSS-14). Foram conduzidas análise descritiva e bivariada, seguidas do modelo de Regressão de Poisson com variância robusta.
RESULTADOS: participaram 1.279 gestantes. A prevalência do nível de estresse elevado foi de 23,5% (IC95%=20,8%-26,2%). O desfecho foi mais prevalente entre gestantes com idade acima dos 35 anos (RP=1,38; IC95%=1,09-1,74) e menor ou igual a 19 (RP=1,41; IC95%=1,13-1,77); sem companheiro(a) (RP=1,33; IC95%=1,09-1,62); com baixo apoio social (RP=1,42; IC95%=1,181,70); multíparas (RP=1,30; IC95%=1,02-1,66); com gravidez atual não planejada (RP=1,23; IC95%=1,00-1,52); infecção urinária (RP=1,35; IC95%=1,12-1,62); alto nível de sintomas de ansiedade (RP=1,42; IC95%=1,18-1,71); sintomas graves (RP=4,74; IC95%=3,60-6,26) e moderados (RP=3,19; IC95%=2,31-4,39) de depressão; e queixas neurológicas (RP=1,77; IC95%=1,27-2,47).
CONCLUSÃO: houve expressiva prevalência de elevado estresse percebido entre gestantes, desfecho associado a fatores sociodemográficos, clínicos, obstétricos e condições emocionais, o que demonstra a necessidade de atenção integral à saúde da gestante.
Palavras-chave:
Gravidez, Gestantes, Estresse psicológico, Atenção primária à saúde, Inquéritos epidemiológicos
IntroductionStress is related to the individual's capacity for adaptation and coping in the management of internal and external stress factors. When it exceeds human resistance and alters the body's homeostasis, it can cause deleterious effects on physical and mental health. The way each individual perceives stress is unique and several factors can trigger it, reducing their quality of life and social well-being.
1-3The gestational period is permeated by physical, emotional, and sometimes social changes and adaptations typical of this phase, which can lead to stress in women.
2-5 Its high levels can generate a variety of adverse outcomes to maternal and child health. There is an increased risk of miscarriage, preterm labor, low birth weight, short-term neonatal morbidities, long-term complications, preeclampsia, and psychiatric comorbidities.
2-4 Stress can also contribute to the adoption of behavioral patterns of health risks by pregnant women.
1,6 After birth, during the child's childhood, there is the possibility of developmental abnormalities such as growth retardation, behavioral problems, and neurodevelopmental disorders.
2-4Another aspect to be considered is the fear of fetal malformations, commonly observed in pregnant women. Upon receiving a poor fetal prognosis, parents seem to lose self-confidence in how to care for their child and may develop feelings of hopelessness, lack of control, and fantasies of death and resurrection. A condition that poses risk to the pregnancy can lead the pregnant woman to feel inferior to other women, which compromises her self-esteem and can damage the emotional bond with the fetus. Therefore, there are several disorders and consequences that the news of fetal malformation entails,
7 including increased stress.
The prevalence of gestational stress is significant in the international
2-4 and national
5,8 scenarios. The main risk factors for stress during pregnancy are multiparity, mental disorders, financial difficulties, alcoholism, smoking, sedentary lifestyle, low education, unemployment, lack of social support, addiction to illicit substances, domestic violence, presence of comorbidities, unplanned pregnancy, and non-acceptance of pregnancy,
1,2,4 besides the fear of fetal malformations.
7The prevalence of stress during pregnancy and its harmful effects in this period show the importance of early detection of this condition, to establish actions to prevent and control this health problem.
4 The Family Health Strategy (FHS), through prenatal care, can contribute to minimizing the impact of stressors on health and unsatisfactory psychosocial outcomes during pregnancy.
9,10Pregnant women assisted by the FHS, to a certain extent, may experience social and health situations that presumably provide vulnerability, which enhances the effects of stress in this population. The literature on prenatal stress in the sociocultural context of developing countries is scarce,
2,4,5 indicating the need for epidemiological research on this theme for a better understanding of its predictive factors.
Therefore, this study aimed to estimate the prevalence of perceived stress and verify the associated factors in pregnant women assisted by Family Health teams in Montes Claros, Minas Gerais (MG) - Brazil.
MethodsThe present study is part of the research entitled "Estudo ALGE - Avaliação das condições de saúde das gestantes de Montes Claros - MG: estudo longitudinal". This is a population-based observational epidemiological survey, with cross-sectional and analytical design, nested within the ALGE cohort.
11The municipality where this study was carried out is located in the northern region of the state of MG Brazil. It is a hub in the region where it is located and has a population of 417.478 inhabitants. It is a reference in the service, commerce, education, and health sectors. The Montes Claros FHS services were implemented in the 1990s and are currently organized in 15 poles. These poles contained a total of 135 family health teams at the time of the research (2018-2019), making coverage of 100% of the population.
The population of this research consisted of 1,661 pregnant women registered in the ESF teams, in the urban area of the municipality of Montes Claros, in the year 2018. For logistical reasons and access difficulties, it was not possible to include pregnant women living in rural areas.
The sample size was established aiming to estimate population parameters with a prevalence of 50% (to maximize the sample size and due to the original project contemplating several events), a 95% confidence interval (CI95%), and an accuracy level of 2.0%. A correction was made for a finite population (N=1,661 pregnant women) and an additional 20% was also established to compensate for possible non-responses and losses. The calculations showed the need for the participation of at least 1.180 pregnant women, distributed among the 15 FHS poles in the municipality. The number of pregnant women defined for the sample of each center was proportional to its representativeness in the total population of registered pregnant women. At first, all the pregnant women registered in the poles were invited to participate in the study, and then there was a simple random draw.
We inform you that the sample interviewed in this research included 1,279 pregnant women, a quantity higher than the minimum quantity indicated in the sample calculation. Therefore, most of the population was analyzed, which ensured greater sample representativeness.
The collection took place between October 2018 and November 2019, in the ESF health units or the homes of the participants, according to their availability. A multi-professional team formed by health professionals and undergraduate students was responsible for the interviews, which occurred face-to-face at a previously defined place and time with the pregnant woman, with an average duration of one hour.
As for the inclusion and exclusion criteria, we included pregnant women who were registered in the urban area FHS team, at any gestational age. The exclusion criterion was being pregnant with twins and/or presenting some cognitive impairment, as informed by the family and/or the FHS team.
Before data collection, interviewers were trained, as well as a pilot study with pregnant women registered in an FHS unit (who were not included in the study analysis), to standardize the research procedures.
For data collection, a structured questionnaire with questions elaborated by the authors and with validated instruments was used, which contemplated sociodemographic and obstetric characteristics, physical and mental health conditions, besides complaints during the gestational period.
In the present investigation, the following sociodemographic characteristics of pregnant women were analyzed age range (up to 19 years, 20 to 35 years, over 35 years); marital status (lives without or with a partner); education (elementary school, high school, and college); family income (up to two minimum wages or more than two minimum wages); receives assistance from the
Bolsa Família Program - a federal government program conditioned to transfer income to families, to help combat social vulnerability (no or yes);
12 family functioning (dysfunctional or functional family); social support (high social support or low social support).
To examine the pregnant woman's perception of family functioning, we applied the instrument named APGAR Family,
13 which signals the fulfillment of basic parameters defined by the acronym APGAR: A - Adaptation (Adaptação); P - Participation (Participação); G - Growth (Crescimento); A - Affection (Afeição); R - Resolution (Resolução). The questionnaire presents five questions with three possible answers each, and scores ranging from zero to two points - never (0), sometimes (1), and always (2). Thus, the sum of zero to ten points is given, and the higher the score, the better the participant's satisfaction. A categorization into "functional family" (scores of 7-10) and "dysfunctional family" (<6) was performed.
13The presence of social support was measured using the Brazilian version of the Medical Outcome Study (MOS) Social Support Scale,
14 composed of 19 questions comprising five dimensions: material, affective, emotional, positive social interaction, and information. For each item, the participant indicates how often he/she considers each type of support, using a Likert-type scale: never (1), rarely (2), sometimes (3), almost always (4), and always (5). The closer the final score is to 100, the better the perceived social support. The overall score of the scale was calculated by the total sum of the 19 items and a score above 66, which corresponds to the second tertile, was considered high social support.
14The obstetric characteristics investigated were gestational trimester (1
st, 2
nd, and 3
rd), current pregnancy planning (yes or no), and parity (nulliparous, primiparous, or multiparous). The following self-reported health conditions were ascertained: urinary tract infection, gestational diabetes, anemia, hemorrhage, pregnancy hypertensive syndromes (PGS), and migraine. The presence of the main complaints during pregnancy was also investigated: sleep-related; cardiovascular (edema, epistaxis, hemorrhoids, palpitation, bleeding gums, varicose veins); cutaneous (chloasmas, stretch marks); gastrointestinal (constipation, abdominal pain, eructation, nausea, heartburn, vomiting, salivation); breast (mastalgia); musculoskeletal (cramps, low back pain); neurological (headache, paresthesias); respiratory (shortness of breath, nasal obstruction); weakness, dizziness, and fainting. Such conditions and complaints were addressed for being among the main risk conditions in pregnancy, based on recommendations of the Brazilian Ministry of Health for low-risk prenatal care in Primary Health Care (PHC).
15The mental health conditions examined were anxiety symptoms (low or high level), depression symptoms (no symptoms, moderate symptoms, or severe symptoms), and stress level (low level and high level). To analyze the anxiety level we used the short version of the Brazilian State-Trait Anxiety Inventory (STAI) - "
Inventário de Ansiedade Traço-Estado" (IDATE) in its Brazilian Portuguese validated version.
16 To track depressive symptoms we used the Center for Epidemiologic Studies Depression Scale (CES-D), also validated in Brazil.
17The STAI provides a reliable measure for two components of anxiety: state and trait. In the IDATE state the person describes how he/she feels "now, right now" regarding six items presented on a four-point Likert scale: 1. absolutely not; 2. a little; 3. a lot; 4. very much. In the STAI-trait the participant responds how he/she "usually feels" for the remaining six items, which are arranged according to a new four-point Likert scale: 1. rarely; 2. sometimes; 3. frequently; 4. almost always. The scores of the positive questions are reversed, ie, 1, 3, and 5 in the STAI-state and 1, 3, and 6 in the STAI-trait. The scores are obtained by the sum of the answers, where 6 is the minimum score and 24 is the maximum, both for state and trait.
16 Since there is no cutoff point for the reduced form, and because the mean and median of the STAI-trait, in the present study, have approximate values, this variable was dichotomized by the median, because it is an integer. Those pregnant women with a value below it were classified as "low anxiety level" and above as "high anxiety level".
The CES-D is composed of 20 items, of which four are positive, in which the respondent reports the frequency of occurrence of symptoms in the last week. Each response can involve four increasing degrees of intensity on a Likert scale - never or rarely, sometimes, often, and always - with scores corresponding to 0, 1, 2, and 3. The score of the four positive items is inverted and added to the scores of the others, giving a final result ranging from zero to 60 points. We proceeded to categorize into: absent/light depressive symptoms (score<16), moderate (score ≥16 or ≤21), and severe symptoms (score ≥22).
17The level of stress (outcome variable) was ascertained through the Perceived Stress Scale (PSS-14),
18 translated and validated for the Brazilian population, which identifies situations in the individual's life assessed as stressful, establishing levels of intensity. This scale is composed of 14 items that evaluate the frequency in which certain feelings and thoughts occurred in the last month, with answers ranging from zero (never) to four (always). The PSS-14 scale score is obtained by reversing the scores of the positive items and summing the responses of the 14 items, with the total score ranging from zero (no stress symptoms) to 56 (symptoms of extreme stress). To classify pregnant women regarding their level of perceived stress, the PSS-14 scale scores were dichotomized into <28 and ≥28, with the cutoff point defined by the 75
th percentile. Pregnant women with scores <28 were classified with low-stress levels and those with scores ≥28 with high stress level.
18The data collected were typed, organized, and analyzed in the Statistical Package for the Social Sciences (SPSS) statistical software, version 23.0 for Windows
®. Descriptive analyses were performed through absolute and relative frequency of all categorical variables, as well as descriptive measures (mean, standard deviation, minimum and maximum) of the PSS-14 scale scores and histogram construction.
The association between the outcome variable (level of stress) and the independent variables (sociodemographic and obstetric characteristics, physical health conditions, anxiety, and depression symptoms) was measured using the chi-square test. Variables that presented a descriptive level (
p-value) up to 0.20 were selected for multiple analyses. The Poisson regression model with robust variance was adopted in the multiple analysis. Prevalence ratios (PR) with their respective CI95% were estimated. The backward stepwise method was used to adjust the model; in this step, the significance level adopted was
p≤0.05. The Deviance test was used to verify the quality of the model adjustment.
The study was approved by the Research Ethics Committee of the University of Montes Claros through the consubstantiated opinions no. 2.483.623/2018 and 3.724.531/2019 of November 25,2019 (CAAE 80957817.5.0000.5146). Authorization was obtained for conducting the research in the ESF teams, through the Institution's Term of Agreement for Participation in Research and Letter, signed by the Coordination of PHC of the Municipal Health Secretariat of Montes Claros. Participants aged 18 years or older signed the Informed Consent Form (ICF); those younger than 18 years and their guardians signed, respectively, the Informed Consent Form (TALE) and the ICF.
ResultsFigure 1 shows the flowchart of the intake of the pregnant women participating in the study.
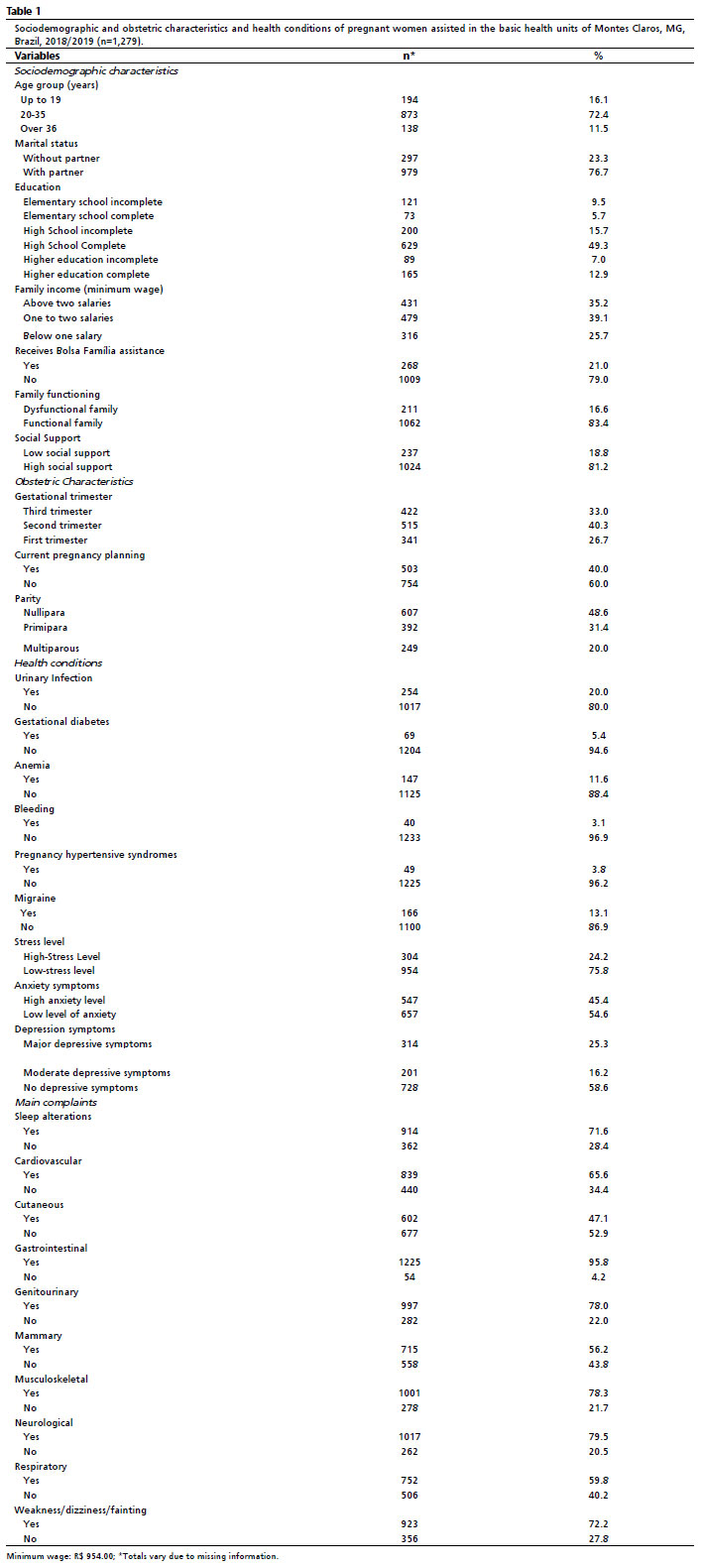
A total of 1,279 pregnant women participated in the study, and the majority (40.3%) were in the second gestational trimester, aged 20 to 35 years (70.9%), lived with a partner (77.2%) and had complete high school education (63.6%). The other sociodemographic and obstetric characteristics, health conditions, and complaints during pregnancy are described in Table 1.
The prevalence of high-stress levels was estimated to be 23.5%, with CI95%= 20.8%-26.2%. The overall mean of the PSS-14 Scale scores in the sample was 24.0, ranging from one to 56 and with a standard deviation of ±8.6 (Figure 2).
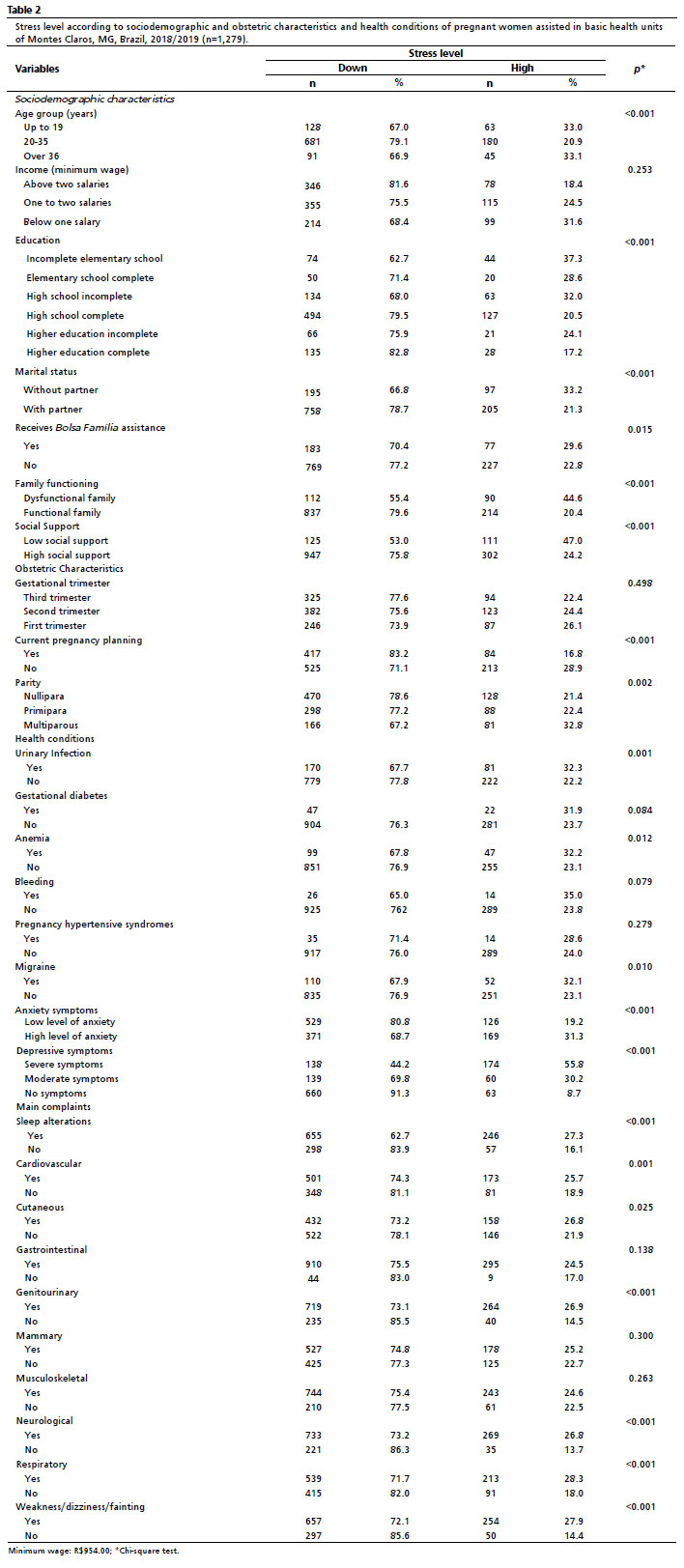
Table 2 shows the results of the bivariate analysis between stress level and the independent variables evaluated. The variables that presented statistical evidence of association with the outcome, at a 0.20 level, were: age group, education, marital status, receiving Bolsa Família Program, family functioning, social support, current pregnancy planning, parity, urinary infection, anemia, migraine, anxiety symptoms, depression symptoms, sleep alterations, cardiovascular, genitourinary, neurological, respiratory complaints, weakness, dizziness, and fainting.
The results of the multiple analysis are described in Table 3. The Deviance test indicated that the model showed an adequate quality of fit (
p=0.840). The high-stress level was more prevalent among pregnant women aged above 35 years (PR=1.38; CI95%=1.09-1.74) and less than or equal to 19 (PR=1.41; CI95%=1.13-1.77); without a partner (PR=1.33; CI95%=1.09-1.62); with low social support (PR=1.42; CI95%=1.18-1.70); multiparous (PR=1.30; CI95%=1.02-1.66) with current unplanned pregnancy (PR=1.23; CI95%=1.00-1.52); urinary infection (PR=1.35; CI95%=1.12-1.62); high level of anxiety symptoms (PR=1.42; CI95%=1.18-1.71); severe (RP=4.74; CI95%=3.60-6.26) and moderate (RP=3.19; CI95%=2.31-4.39) symptoms of depression; and neurological complaints (RP=1.77; CI95%=1.27-2.47).
DiscussionThis study showed that approximately one-fourth of the pregnant women analyzed presented a high level of stress, an outcome that was associated with sociodemographic factors (age group, marital status, social support), obstetric factors (unplanned pregnancy, multiparity), health problems during pregnancy (urinary tract infection, anxious and depressive symptoms) and gestational complaints (neurological).
In the international scenario, it was observed that in Germany the prevalence of stress was 95% of the surveyed pregnant women,
19 in China at 91.86%,
20 in Thailand at 23.6%
21, and in Ethiopia at 11.6%.
2 In Suriname, high perceived stress occurred in 27.2% of the participants during the first/second trimester and in 24.7% during the third trimester.
4 In Brazil, the prevalence of stress in pregnant women from Santa Catarina was 93%
4 and 78% in those from São Paulo.
22 It must be considered that the differences in the prevalence of stress levels in the populations may be related to different methodological criteria used in the screening of this condition, and also to ethnic, demographic, social, economic, and cultural specificities.
Given the expressive prevalence of high levels of stress perceived among the women surveyed, it is worth pointing out that pregnancy demands from women a series of adaptations and experiences that propitiate a greater emotional vulnerability to psychosocial conditions.
2,10 Stress emerges in everyday life and can be identified in daily relationships. It is linked to the changes of pregnancy itself and the different confrontations related to the roles played socially, with greater overload and maternal responsibility in the pregnancy cycle. Added to daily stress are the tensions about pregnancy and childbirth, the need to plan the tasks of caring for the unborn baby, in addition to the difficulty to perform work, domestic, and social activities.
10 Therefore, family health professionals need to pay attention to the screening of stress during pregnancy, to reduce the probability of worsening the clinical picture and to avoid compromising mental health,
1,2,5,10 recognizing that pregnancy goes beyond the biological dimension.
As for the factors associated with high-stress levels, age was positively associated with the occurrence of this outcome: it was more prevalent among pregnant women aged less than or equal to 19 years and over 35 years. A study conducted in Iran found higher stress scores in older women.
23 Pregnancy after 35 years of age is considered high-risk, which possibly causes women to experience this period with worry, fear, and stress.
24 As for younger pregnant women, among whom are the adolescents in this survey, a possible explanation for the relationship with the researched event stems from the challenges faced in pregnancy during adolescence. It is worth noting that teenage pregnant women may present greater emotional, socioeconomic, and family vulnerability,
11,25 which favors the occurrence of stress during a phase of greater accountability because of the challenges and new demands of the transition to motherhood. Adolescence is a critical phase of the life cycle in which several social, physical, biological, and psychological changes occur, as well as the pregnancy period. Pregnant adolescents may experience feelings of shame and stigmatization, which result in loneliness, school dropout, and lack of family and social support.
25The highest prevalence of high levels of stress was seen among pregnant women living without a partner. In Thai pregnant women, stress symptoms were found to be significantly associated with divorce and separation from a spouse.
21 Research in Nigeria also found that marital status was associated with stress during pregnancy among adolescents.
25 A possible explanation is related to stigmatization and negative feelings that women experience due to cultural values in this condition.
25 Moreover, in the absence of a partner, there is a lack of material, social and emotional support that a partner can offer. With a partner present during pregnancy, the woman can feel supported against adverse situations, which provides a greater bond and emotional support.
10Low social support for pregnant women has been associated with the presence of high-stress levels. A study conducted with Chinese pregnant women observed that women with low or moderate levels of social support were more likely to suffer prenatal stress than those with high levels of social support.
20 A study conducted in the interior of São Paulo also observed a moderate and inverse correlation between the variables stress and social support.
8 Social support is a dynamic process and consists of all the support provided by family and friends to provide the pregnant woman with a feeling of support, care, and help in her needs. The pregnancy phase is marked by transformations in the physical, emotional, social, and economic status, therefore the presence of social support can contribute to the necessary comfort for the pregnant woman's wellbeing.
5,8,10A higher prevalence of perceived stress has been verified in multiparous women. Research conducted with pregnant women in Pakistan showed that an increase in the number of children was associated with a higher score on the PSS-14.
26 After experiencing previous pregnancies, women experience pregnancy with less enthusiasm, and become more concerned with problems related to family dynamics, child-rearing, and financial repercussions.
26The high level of stress was statistically associated with the absence of pregnancy planning. A similar result was found in a previous study.
26 Lower stress scores were observed in Iranian pregnant women with planned pregnancies.
23 Unplanned pregnancy may leave women with excessive worry and discontent due to restructuring and the need to adapt, anxiety about the health care required at this stage, financial expenses, and lack of social support.
23,26The occurrence of UTIs in the pregnant women studied was associated with a high level of stress. The UTI can affect the physical conditions and cause discomfort to the pregnant woman, such as dysuria, increased frequency, and urgency to urinate, lower abdominal pain, chills, and lower back pain. Moreover, the woman, upon learning that UTI may constitute one of the main risk factors for miscarriage and premature birth, may become fearful and develop stress.
27Another important intervening factor in the high level of stress was the presence of anxiety symptoms, as also verified in previous studies in China
20 and Brazil.
8 It must be considered that gestational changes, apprehensions about income, and issues related to pregnancy development and the postpartum phase may cause emotional changes and increased stress, configuring a situation that favors the emergence of anxious symptoms in prenatal care.
20Similar to other investigations,
1,4,8 another factor associated with high-stress levels was the presence of severe and moderate depressive symptoms. Perceived stress is an important risk factor for depression during pregnancy.
4 Depression is one of the disorders that can develop during pregnancy, with symptoms that affect the pregnant woman's self-care and adherence to prenatal care. The transition to motherhood, since pregnancy and childbirth can be stressful situations, in addition to socioeconomic, psychosocial, and hormonal determinants, can compromise the biopsychosocial well-being of pregnant women and contribute to the emergence of depressive symptoms. When this occurs, early diagnosis and longitudinal follow-up are necessary.
5,8 It is recommended that the FHS teams establish a more humanized and welcoming relationship in the process of preparing pregnant women and their families for prenatal care and the formation of healthier bonds, going beyond the technical approach to women. With this, the aim is maternal well-being and mental health.
5,10This study also showed that the presence of neurological complaints (headaches and paresthesia) during pregnancy was positively associated with the occurrence of a high level of stress. Previous research conducted with women followed by family health teams verified the association between migraine and stress.
28 A systematic review with meta-analysis revealed that a history of migraine presence is associated with an increased risk of adverse pregnancy outcomes, such as preeclampsia and low birth weight.
29Therefore, early diagnosis of this condition is important for the life of the mother and fetus,
30 so it should be screened, monitored, and treated in prenatal care in PHC.
29 Preventive medication options are limited, and it may be best to consider the safest interventions, which are lifestyle changes and behavioral treatment for stress control.
30The knowledge and awareness about the factors that influence the occurrence of gestational stress are essential for the planning and implementation of measures to prevent, identify, monitor, and control this condition during prenatal care, due to the peculiar characteristics of this period and based on regional and cultural characteristics in which the woman is inserted.
22 The screening of perceived stress should be applied in routine prenatal care, considering the associated factors among pregnant women. The articulated action of family health teams together with families in prenatal care is a strategy for the prevention, early detection, and follow-up of pregnant women with a greater need for qualified listening and mental health care.
4,5,8One should consider as a limitation of the study the use of self-report, which may be influenced by memory bias. The validated instruments were used to minimize this situation. The non-inclusion of pregnant women living in rural areas is a limitation. The results obtained are valid only for the population of pregnant women assisted in the ESF units of Montes Claros, so extrapolations for other populations are not possible. However, the findings of this study allow a discussion on the theme, which is still incipient in the national scenario. Additionally, this is a population-based survey that provided relevant epidemiological evidence for further research and the promotion of health among pregnant women. It was conducted with a significant sample size, which strengthened the associations found.
It was concluded that the occurrence of perceived stress was identified in a representative part of the pregnant women assisted by the ESF teams in the city of Montes Claros. Pregnant women over 35 years old and younger than or equal to 19 years old, without a partner, with low social support, multiparous, whose current pregnancy was not planned, with urinary infection, with symptoms of anxiety and depression, and with neurological complaints presented higher prevalences of high levels of stress.
References1. Saur AM, Santos MA. Risk factors associated with stress symptoms during pregnancy and postpartum: integrative literature review. Women Health. 2021 Aug; 61 (7): 651-67.
2. Engidaw N, Mekonnen AG, Amogne FK. Perceived stress and its associated factors among pregnant women in Bale zone Hospitals, Southeast Ethiopia: a cross-sectional study. BMC Res Notes. 2019; 12: 356.
3. Goletzke J, Kocalevent RD, Hansen G, Rose M, Becher H, Hecher K, et al. Prenatal stress perception and coping strategies: insights from a longitudinal prospective pregnancy cohort. J Psychosom Res. 2017 Nov; 102: 8-14.
4. Gokoel AR, Wahid FA, Zijlmans WC, Shankar A, Hindori-Mohangoo AD, Covert HH, et al. Influence of perceived stress on prenatal depression in Surinamese women enrolled in the CCREOH study. Reprod Health. 2021 Jun; 18 (1): 136.
5. Gomes FCS, Aragão FBA, Serra LLL, Chein MBC, Cunha JHS, Pires FK, et al. Factors associated with women’s psychosocial profile during prenatal. Medicina (Ribeirão Preto). 2022; 55 (1): e-183396.
6. Pakzad M, Dolatian M, Jahangiri Y, Nasiri M, Dargah FA. The correlation between islamic lifestyle and pregnancy-specific stress: a cross-sectional, correlational study. Open Access Maced J Med Sci. 2018 Jun; 6 (6): 1163-7.
7. Souza GFA, Souza ASR, Praciano GAF, França ESL, Carvalho CF, Paiva Júnior SSL, et al. Apego maternofetal e transtornos psiquiátricos em gestantes com fetos malformados. J Bras Psiquiatr. 2022; 71 (1): 40-9.
8. Soncini NCV, Oliveira CM, Viviani JC, Gorayeb R. Aspectos psicossociais em mulheres brasileiras com gestações de alto e baixo risco. Psicol Saúde Doenças. 2019; 20 (1): 122-36. 9. Luz LA, Aquino R, Medina MG. Evaluation of the quality of prena-tal care in Brazil. Saúde Debate. 2018; 42 (Esp. 2): 111-26.
10. Gomes FCS, Aragão FBA, Serra LLL, Chein MBC, Santos JPF, Santos LMR, et al. Relação entre o estresse e a autoestima de gestantes durante o pré-natal. Medicina (Ribeirão Preto). 2020; 53 (1): 27-34.
11. Merchán-Hamann E, Tauil PL. Proposal for classifying the different types of descriptive epidemiological studies. Epidemiol Serv Saúde. 2021; 30 (1): e2018126.
12. Santos MCS, Delatorre LR, Ceccato MGB, Bonolo PF. Programa Bolsa Família e indicadores educacionais em crianças, adolescentes e escolas no Brasil: revisão sistemática. Ciênc Saúde Colet. 2019; 24 (6): 2233-47.
13. Smilkstein G. The family APGAR: a proposal for a family function test and its use by physicians. J Fam Pract. 1978; 6 (6): 1231-9.
14. Griep RH, Chor D, Faerstein E, Werneck GL, Lopes C. Validade de constructo de escala de apoio social do Medical Outcomes Study adaptada para o português no Estudo Pró- Saúde. Cad Saúde Pública. 2005; 21 (3): 703-14.
15. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Atenção ao pré-natal de baixo risco. Brasília (DF): Ministério da Saúde; 2012. [acesso em 2022 Fev 13]. Disponível em:
https://bvsms.saude.gov.br/bvs/publicacoes/cadernos_atencao_basica_32_prenatal.pdf16. Fioravanti-Bastos ACM, Cheniaux E, Landeira-Fernandez J. Development and validation of a short-form version of the Brazilian state-trait anxiety inventory. Psicol Reflex Crít. 2011; 24 (3): 485-94.
17. Radloff LS, Silveira DX, Jorge MR. Propriedades psicométricas da Escala de Rastreamento Populacional para Depressão CES-D em populações clínica e não-clínica de adolescentes e adultos jovens. Rev Psiquiatr Clin. 1998; 25 (5): 251-61.
18. Luft CDB, Sanches SO, Mazo GZ, Andrade A. Versão brasileira da Escala de Estresse Percebido: tradução e validação para idosos. Rev Saúde Pública. 2007; 41 (4): 606-15.
19. Eichler J, Schmidt R, Hiemisch A, Kiess W, Hilbert A. Gestational weight gain, physical activity, sleep problems, substance use, and food intake as proximal risk factors of stress and depressive symptoms during pregnancy. BMC Pregnancy Childbirth. 2019 May; 19 (1): 175.
20. Tang X, Lu Z, Hu D, Zhong X. Influencing factors for prenatal Stress, anxiety and depression in early pregnancy among women in Chongqing, China. J Affect Disord. 2019; 253: 292-302.
21. Thongsomboon W, Kaewkiattikun K, Kerdcharoen N. Perceived stress and associated factors among pregnant women attending antenatal care in urban Thailand. Psychol Res Behav Manag. 2020 Dec; 13: 1115-22.
22. Rodrigues OMPR, Schiavo R. Stress na gestação e no puerpério: uma correlação com a depressão pós-parto. Rev Bras Ginecol Obstet. 2011; 33 (9): 252-57.
23. Keramat A, Malary M, Moosazadeh M, Bagherian N, Rajabi-Shakib MR. Factors influencing stress, anxiety, and depression among Iranian pregnant women: the role of sexual distress and genital self-image. BMC Pregnancy Childbirth. 2021; 21 (1): 1-12.
24. Vieira VCL, Barreto MS, Marquete VF, Souza RR, Fischer MMJB, Marcon SS. Vulnerabilidade da gravidez de alto risco na percepção de gestantes e familiares. Rev Rene. 2019; 20 (1): e40207.
25. Olajubu AO, Omoloye GO, Olajubu TO, Olowokere AE. Stress and resilience among pregnant teenagers in Ile-Ife, Nigeria. Eur J Midwifery. 2021; 5: 1-9.
26. Waqas A, Zubair M, Zia S, Meraj H, Aedma KK, Majeed MH, et al. Psychosocial predictors of antenatal stress in Pakistan: perspectives from a developing country. BMC Res Notes. 2020; 13 (1): 1-6.
27. Pagnonceli J, Colacite J. Infecção urinária em gestantes: revisão de literatura. Rev Uningá Rev. 2016; 26 (2): 26-30.
28. Correia LL, Linhares MBM. Enxaqueca e estresse em mulheres no contexto da Atenção Primária. Psic Teor Pesq. 2014; 30 (2): 145-52.
29. Aukes AM, Yurtsever FN, Boutin A, Visser MC, Groot CJM. Associations between migraine and adverse pregnancy outcomes: systematic review and meta-analysis. Obstet Gynecol Surv. 2019; 74 (12): 738-48.
30. Negro A, Delaruelle Z, Ivanova TA, Khan S, Ornello R, Raffaelli B, et al. Headache and pregnancy: a systematic review. J Headache Pain. 2017; 18 (1): 106.
Received on May 11, 2022
Final version presented on September 5, 2022
Approved on September 21, 2022
Associated Editor: Alex Sandro Souza
Acknowledgments: We thank the
Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) and the
Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) for the financial support.
Authors' contribution: Lopes BCS, Lima CA, Ferreira TSB, Freitas WML, and Ferreira TB: conception and design of the study, data collection, drafting of the manuscript. Pinho L and Brito MFSF: conception and design of the study, supervision of data collection, data analysis and interpretation, critical revision of the manuscript. Silveira MF: conception and design of the study, statistical analysis, and interpretation of data, critical revision of the manuscript. The authors approved the final version of the article and declare no conflict of interest.


 ; Cássio de Almeida Lima2
; Cássio de Almeida Lima2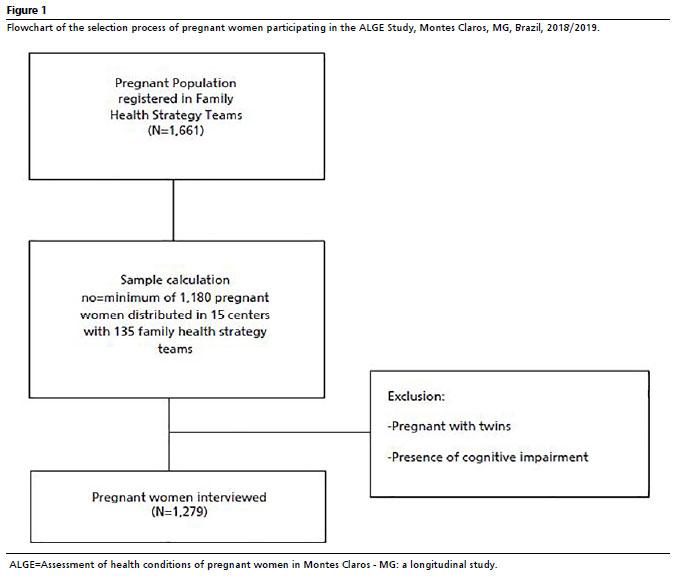








 Ler em português
Ler em português