ABSTRACT
OBJECTIVE: to assess the association between caregivers' mental disorders and schoolchildren's obesogenic eating behavior.
METHODS: cross-sectional study used a public school-based sample of children and their primary caregivers. Caregivers had to report depressive episodes or generalized anxiety disorder (GAD) during the Mini-International Neuropsychiatric Interview (MINI). Children's obesogenic eating behavior were assessed using food responsiveness (FR) and emotional overeating (EOE) subscales of the Children's Eating Behaviour Questionnaire (CEBQ). Bivariate analysis was conducted using the t-test, ANOVA, Pearson correlation, and adjusted linear regression model was used (including variables caregivers: sex, age, economic indicator, and schooling; schoolchildren: sex and nutritional status).
RESULTS: study includes 596 children-caregiver dyads (309 boys and 287 girls). Among caregivers, 24.7% had experienced current depressive episodes, 38.7% had past depressive episodes, and 17.2% had GAD. We observed, after adjusted analysis, that having a caregiver in a current depressive episode, increases schoolchildren's obesogenic behavior of, for FR at 0.235 points (β=0.235; CI95%=0.022-0.449;) and EOE at 0.337 points (β=0.337; CI95%=0.162-0.512).
CONCLUSION: caregivers' current depressive episodes were associated with higher averages of obesogenic eating behavior (caregiver-reported), both in consuming palatable food without feeling hungry (FR) and in increasing food intake in response to negative emotions (EOE).
Keywords:
Mental disorders, Obesogenic behavior, Schoolchildren, Caregivers, Eating behavior
RESUMO
OBJETIVOS: avaliar associação entre transtornos mentais do cuidador e comportamento alimentar obesogênico de escolares.
MÉTODOS: estudo transversal com amostra de crianças da rede pública de ensino e seu cuidador principal. Episódio depressivo atual e transtorno de ansiedade generalizada (TAG) do cuidador foi avaliado pela Mini-International Neuropsychiatric Interview (MINI). Comportamentos alimentares obesogênicos das crianças foi avaliado pelas subescalas resposta à comida (FR) e sobreingestão emocional (EOE) Children's Eating Behaviour Questionnaire (CEBQ). Análise bivariada foi realizada por meio de teste-T, ANOVA e correlação de Pearson. Modelo de regressão linear ajustado (incluiu variáveis cuidadores: sexo, idade, indicador econômico e escolaridade; escolares: sexo e estado nutricional).
RESULTADOS: foram avaliadas 596 díades crianças-cuidadores (309 meninos e 287 meninas). Entre os cuidadores, 24,7% apresentaram episódio depressivo atual, 38,7% episódio depressivo passado e 17,2% TAG. Observamos, após análise ajustada, que ter um cuidador em episódio depressivo atual aumenta o comportamento obesogênico dos escolares, em 0,235 pontos para FR (β=0,235; IC95%=0,022-0,449) e em 0,337 pontos para EOE (β=0,337; IC95%=0,162-0,512).
CONCLUSÃO: episódio depressivo atual do cuidador foi associado a maiores médias de comportamentos alimentares obesogênicos dos escolares, tanto no consumo de alimentos palatáveis mesmo sem fome (FR) quanto aumento da ingestão alimentar em resposta a emoções negativas (EOE).
Palavras-chave:
Transtornos mentais, Comportamentos obesogênicos, Alunos, Cuidadores, Comportamento alimentar
IntroductionEating behaviors are defined as attitudes and psychosocial factors related to the selection and decision regarding which food to eat, and are the result of a combination of genetic, biological, cultural, and environmental factors.
1,2 Eating behaviors that predispose an individual to eat for reasons other than hunger have been described as obesogenic and implicated in the etiology of childhood obesity.
3,4 Obesogenic eating behavior include emotional overeating (EOE), characterized by increased food intake to satisfy emotional needs, especially in response to negative emotions, and food responsiveness (FR), which refers to the urge of eating when smelling, seeing, or tasting palatable food, even without feeling hungry.
3,4 Both have been positively associated with excess weight gain and higher body mass index (BMI) across one's lifespan.
1,5,6Childhood obesity and children's eating behavior are multifactorial,
2,7 and the family environment is critical in the development of children's eating behavior.
1,8 The emotional quality of the parent-child relationship may play an important role in what is transmitted to the child within the family context, especially when it comes to feeding.
9 Within this context, the feeding practices used by parents were relevant. Research conducted by Lindsay
et al. 10 identified uninvolved and permissive feeding styles, feeding practices using instrumental feeding (e.g. , use of food as a reward), and pressuring children to eat, as most consistently associated with depressive symptoms. Maternal depressive symptoms were associated with uninvolved and permissive family mealtime practices.
10 It is worth highlighting that children are susceptible to the effects of parents' mental disorders,
11 and depressive and anxiety disorders are among the most prevalent mental disorders in the general population.
12 The presence of mental disorders contributes to a more chaotic family environment,
13 which may reflect the construction of obesogenic eating behaviors.
5 A population-based study that examined patterns of eating behaviors from ages 4 to 10 years old found that the offspring of mothers with more psychopathology symptoms were more likely to have an increasing EOE pattern.
5 However, FR was not consistently associated with maternal or paternal psychopathology symptoms.
5Understanding the etiology of children's eating behavior and identifying modifiable factors is extremely relevant for planning interventions to combat childhood obesity, especially between the ages of 4 and 10 years old, as the patterns of eating behavior solidify during this time, and are susceptible to several factors.
5 The relationship between childhood obesity and parental mental health has been widely identified in the literature.
14,15 Furthermore, regarding mental disorders, the relationship between children's eating behaviors and mothers' eating disorders has already been investigated.
16 Although most studies evaluate parents, especially mothers, it is also important to assess the views of the main caregiver, being the mother, father, grandmother, or aunt. However, we know that caregivers play a role similar to that of the mothers and are very important in the development of overweight children because they generally spend most of the time with the children.
17 However, few studies aim to understand the relationship between caregivers' mental disorders, especially depression and anxiety, and children's obesogenic eating behavior. Therefore, understanding the influence of caregivers' mental health is crucial. Therefore, the objective of this study was to assess the association between caregivers' mental disorders and schoolchildren's obesogenic eating behavior.
MethodsWe performed a cross-sectional study between August 2015 and November 2016, using a school-based sample in a city in the South of Brazil. We evaluated public school students and one of their primary caregivers (responsible for the child's care most of the time, not necessarily the father or mother).
The sample selection was performed using probabilistic sampling with public elementary schools as the primary sample units in the city. Twenty schools were selected by a systematic random sampling from a total of 40 schools in the urban area of Pelotas-RS, Brazil. The inclusion criteria were that the schoolchildren should be 7 or 8 years old and regularly enrolled in school. This study was part of a larger study in which the cognitive performance of schoolchildren was assessed; for this, it was necessary to be 8 years old or to complete 8 years of age in the year in which the data were collected. For caregivers, it was necessary to be primarily responsible for the care of schoolchildren and to be over 18 years old. The exclusion criteria were the inability to understand or respond to the instruments due to any clinical condition, or schoolchildren's severe disability or their caregivers. Data collection involved the following steps: (1) the identified school principals were contacted and the project presentation was made to them; (2) the eligible schoolchildren for the study were enlisted; (3) written informed consent was sent to caregivers to authorize their participation (two terms were signed, one for them and one for the children); (4) the authorized schoolchildren were evaluated in the school setting during school hours; and (5) caregivers were interviewed in their homes. The interviewers were healthcare students who had conducted the assessments after training with experienced professionals. Upon identification of mental health and/or nutritional problems, respondents immediately received a document with a referral to public health services.
Current and past depressive episodes, and generalized anxiety disorder (GAD) in caregivers were assessed using the Mini International Neuropsychiatric Interview (MINI), a brief standardized diagnostic interview based on criteria from the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV).
18 The psychometric characteristics of the Brazilian version of the MINI compared to Structured Clinical Interview for DSM Disorders (SCID) were satisfactory (major depressive episode:
kappa=0.84, sensibility=0.96, specificity=0.88; GAD:
kappa=0.70, sensibility=0.91, specificity=0.86).
19 The MINI is organized into independent diagnostic modules, designed to optimize the sensitivity of the instrument, despite a possible increase in false positives.
18 Each module assesses a set of symptoms through questions such as , "In the past two weeks, have you felt sad, discouraged, depressed, most of the day, almost every day?"; "Over the course of your life, have you had periods of two weeks or more when you felt depressed or uninterested in most things and during which you had the problems we have talked about?"; "During the past six months, have you felt excessively worried, restless, anxious about various problems in everyday life (work/school, home, family/friends), or had the impression or did anyone say you worry too much about everything?".
18 A personal, face-to-face clinical interview was conducted. All variables were classified as 'no' or 'yes'.
The Children's Eating Behavior Questionnaire (CEBQ) was created to study the eating behavior of children, aged 3 to 13 years old, in the context of obesity or risk. It may also be indicated for the investigation of eating styles in healthy children or children with atypical eating behavior. The CEBQ is a parent-reported psychometric measure of eight appetitive traits to distinguish differences in eating behavior that could contribute to high or low weight and is a widely used 35-item tool.
4 The CEBQ has been validated in different populations, translated, and validated for a sample of Portuguese children showing good psychometric properties (food responsiveness, α=0.88; emotional overeating, α=0.77).
20 To assess eating styles related to obesity risk, the CEBQ scales included in this study were FR (five items, e.g. , My child would eat most of the time if given the chance) and EOE (four items, e.g. , My child eats more when worried). The questionnaire used a five-point Likert scale (never, rarely, sometimes, often, and always; ranging from 1 to 5). Mean scores were calculated for each scale, with higher mean scores indicating a higher expression of that behavior.
Structured questionnaires were used to collect socio-demographic data. The following characteristics of schoolchildren were collected: sex (male or female) and age (years). Additionally, to evaluate the BMI, anthropometric measures of schoolchildren's height and weight were obtained as follows: the schoolchildren were weighed and measured barefoot, wearing light clothing, and their heights were measured in the standing position using a Cardiomed stadiometer (1mm accuracy) with an easily moveable horizontal headboard that could be brought into contact with the most superior part of the head. Weight was obtained using a properly calibrated Tanita digital scale (100g accuracy), considering a decimal digit of accuracy. Anthropometric measurements were collected by properly trained health students. BMI was calculated according to WHO parameters, which consider the child's weight, height, sex and age to generate BMI z-scores.
21Caregivers' characteristics were self-reported and included sex (male or female), age (years), schooling (≤8, 9-11 or ≥12 years), relationship with schoolchildren (biological mother/father or adoptive parent/grandparents/other), living with a partner (no or yes), currently working (no or yes), and economic indicators. Economic indicators were measured using the Brazilian National Wealth Index. This enables the calculation of scores (referred to as income quintiles) for households based on information on the ownership of a set of assets, household characteristics, and the household head'sschooling; however, in this study, terciles (lower, intermediate, or upper) were used. The economic level was presented in sample tertiles, with the first group (lower) referring to the least economically favored and the third (upper) to the most economically favored.
22 In addition, we included the caregivers' BMI (kg/m
2), calculated based on self-reported height and weight data.
Analyses were pre-specified and performed using Statistical Package for the Social Sciences version 21.0 (SPSS 21.0). Bivariate analysis was conducted using the t-test, Analysis of Variance (ANOVA), and Pearson's correlation, to describe the means of eating behaviors (FR and EOE) according to the exposure variables of the children and caregivers. Multiple linear regression analysis was used to verify the adjustment for possible confounding factors. The assumptions of normal distribution and homogeneity of residuals were ensured, and both were analyzed graphically (normal probability plot and residual graphs). The Levene test was used to assess homogeneity. For the student's t-test, used to compare the sample means of two independent groups when the variances were heterogeneous, the corrected
p-value for homogeneity was used. The assumption of residual independence was verified using the Durbin-Watson test. The assumption of the non-existence of multicollinearity between the covariates was guaranteed through the values of the correlations between the covariates of r<0.70. Outliers were identified graphically, based on information from the descriptive statistics of the residuals. After eliminating the outliers, the assumptions of multiple linear regression, previously described, were also guaranteed, resulting in the final data available in this article. The adjusted analyses included those variables with a
p<0.20 in the bivariate analysis. Thus, the initial model included variables about caregivers(sex, age, economic indicators, education, and BMI) and children's characteristics (sex and BMI).
23 The final model was reached using stepwise backward analysis of each variable with
p<0.05.
This study is part of a major project entitled, "Healthy Childhood in Context: A Multidisciplinary Investigation," approved by the Ethics Committee of the
Universidade Católica de Pelotas, Brazil, under protocol number 843.526 and CAAE 27696014.00005339.
ResultsA total of 723 schoolchildren were considered eligible for inclusion in this study. Of these, 34 (5%) did not attend school on the evaluation days, 80 (11%) declined participation by their caregivers, and 13 (1.8%) were not located or refused to participate in the study. Thus, 596 dyads were included in this analysis.
Among the schoolchildren assessed, 24.0% were obese, 51.9% were boys with a mean age of 7.5 years and an average BMI of 18.27kg/m
2. Among the caregivers assessed, 91.1% were female, with a mean age of 35 years old, and 50.9% had had up to eight years of schooling. Moreover, 53.1% were currently working, 73.1% lived with a partner, and 91.1% were biological mothers/fathers of the evaluated and had a mean BMI of 27.47kg/m
2. Regarding mental disorders among caregivers, 24.7% had experienced a current depressive episode, 38.7% had a past depressive episode, and 17.2% suffered from GAD (Table 1).
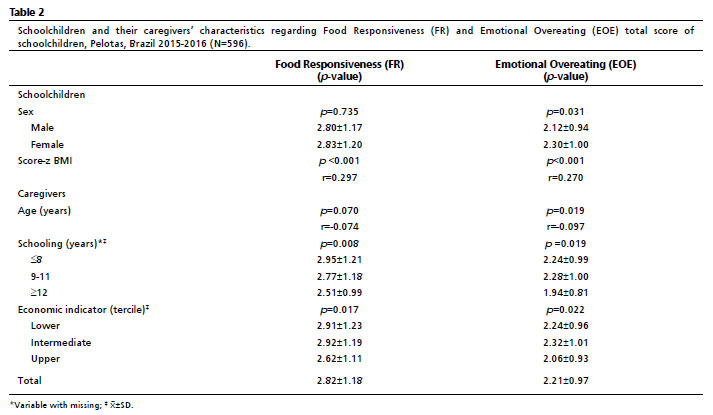
In crude analysis, a positive correlation was observed between FR and Score-Z BMI (r=0.297,
p<0.001). Regarding caregivers' variables, FR was associated with education (
p=0.008) and economic indicator (
p=0.017). EOE was associated with two variables among schoolchildren: sex and score-Z BMI. Higher averages of EOE were observed among girls (
p=0.031), and a positive correlation was observed between EOE and score-Z BMI (r=0.270,
p<0.001). Regarding caregivers' variables, a negative correlation was observed between EOE scores and caregivers' age (r=-0.097,
p=0.019). EOE also associated with caregivers'schooling (
p=0.019), and economic indicators (
p=0.022) (Table 2).
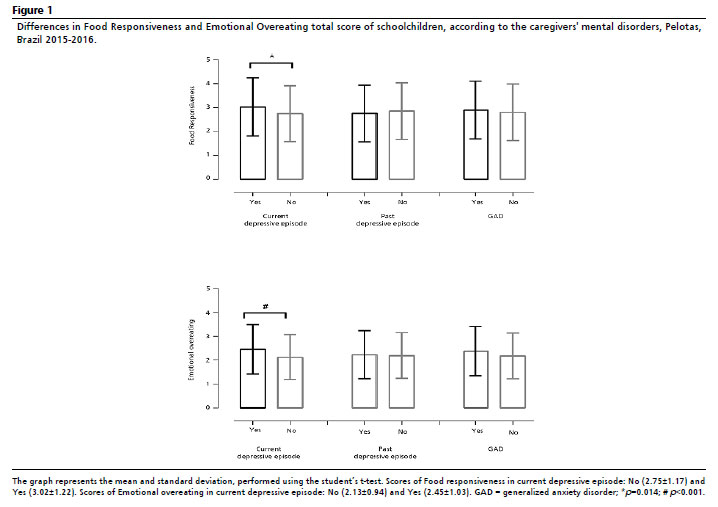
Regarding mental disorders, higher averages in FR (
p=0.014) and EOE (
p<0.001) were observed in schoolchildren whose caregivers had experienced current depressive episodes. Schoolchildren whose caregivers had GAD or past depressive disorders did not differ in terms of FR or EOE (Figure 1).
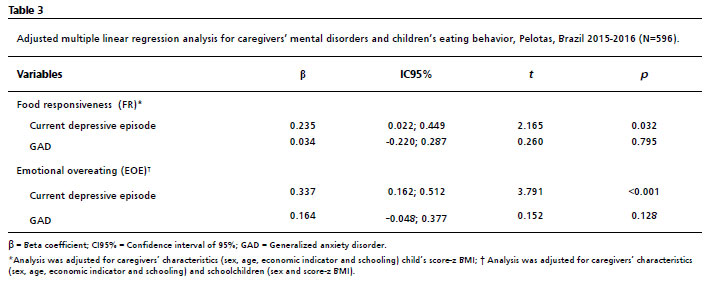
In the adjusted analysis (multiple linear regression), the model included sex, age, economic indicators, education, BMI and score-z BMI as showed in Table 3. GAD was not associated with FR and EOE. However, we found that current depressive episodes in caregivers remained associated with FR (β=0.235; CI95%=0.022-0.449;
p=0.032) and EOE (β=0.337; CI95%=0.162-0.512;
p<0.001), even after adjusting for potential confounders. Thus, having caregivers in a current depressive episode increases students' obesogenic behavior for FR by 0.235 points and EOE by 0.337 points.
DiscussionThis study investigated the association between caregivers' mental disorders and the schoolchildren's obesogenic eating behavior. We found a relationship between caregivers' mental health and schoolchildren's eating behavior. Caregivers' current depressive episodes were associated with higher averages of obesogenic eating behavior: FR, that is, schoolchildren's susceptibility to external aspects of food, such as the appearance of food, consequently increasing food consumption even without feeling hungry; and EOE, that is, an increase in food intake in response to negative emotions such as anger and anxiety among schoolchildren.
A substantial body of literature aims to understand the influence of caregivers' feeding practices on children's food behavior,
24 and specific links on caregivers' feeding behaviors to child's self-regulation in eating.
25 However, little is known about the relationship between caregivers' mental disorders and children's eating behavior. This is one of the first studies to understand the relationship between caregivers' mental health and obesogenic behavior.
Our findings showed that caregivers' current depressive episodes were associated with FR in schoolchildren. In an Australian study of children aged 2-5 years old, FR was predicted only by parental stress, not depression or anxiety.
26 In contrast, Derks
et al. 5 found that maternal, but not paternal, psychopathology symptoms were associated with increased FR. Caregivers' depression can generate a stressful environment, and they may be unresponsive to the child's demands.
11 This can interfere with the child's interaction in different areas, including the relationship with food, especially in the formation of eating behavior. Early life stress can shape the development of certain obesogenic eating behavior during childhood, which may be a mechanism that links early life stress exposure with childhood obesity.
27 Additionally, current depressive episodes were associated with EOE. Derks
et al. 5 also identified parental predictors of offspring's emotional overeating patterns: offspring of mothers with more psychopathology symptoms were more likely to have emotional overeating patterns. Caregivers facing emotional difficulties can use food as a strategy to manage children's negative emotions.
28 Unlike most other appetitive traits that have strong genetic underpinnings, a study with twins showed that individual variation in EOE in childhood was largely explained by environmental influences, suggesting that EOE is largely learned in early life and that genetic effects play a minor role compared to the environment.
29Derks
et al. 5 found distinct patterns of FR and EOE throughout childhood, suggesting that, despite continuity and stability in most children, their developmental patterns may not be uniform and that EOE and FR are dynamic behaviors in the initial years of life, which can change after preschool age. In that study, the authors evaluated children aged 4-10 years old.
5 In our sample, the schoolchildren were evaluated in the age group of 7 to 8 years old; therefore, as per Derks
et al. ,
5 children belonging to this age group were still considered unstable in terms of the consolidation of eating behaviors.
5 Thus, children's eating behavior may be susceptible to the influence of different factors such as caregivers' mental disorders.
Most studies included the mother as the main caregiver, although we included other caregivers (parents, grandparents, others); even so, most caregivers evaluated were female, and most of them could be biological mothers.
17 Mothers are mostly and historically involved in their children's care, which adds to other attributions, generating a high burden.
30 In view of this, the importance of mental health assessment is highlighted, as well as the implementation of public policies aimed at meeting this demand.
This study has the following limitations: the cross-sectional design has a limitation regarding causal inference, as it is not possible to verify whether the assessed eating behaviors were determinants or consequences of excess weight. The non-inclusion of private schools in the sample limits the comparison. Most of the schools considered are located in areas with greater social vulnerability. This factor is strongly associated with a higher prevalence of mental disorders. The CEBQ, a questionnaire validated in a sample of Portuguese children, but not Brazilian ones, was answered by the principal caregivers; therefore, it is subject to the caregiver's perception and may be subject to a social desirability bias. It is noteworthy that caregivers experiencing a depressive episode may have a more negative perception of children's eating behavior due to the symptoms of mental disorders. Finally, only the mental disorders of one caregiver were evaluated. As a strength, we highlight the fact that the study presents innovative findings regarding the relationship between the caregivers' mental health and children's eating behavior, especially regarding obesogenic behavior. In addition, the findings may be representative of public schoolchildren aged 7-8 years old for a population with characteristics similar to the city of Pelotas.
In conclusion, the presence of mental disorders in caregivers was associated with schoolchildren's eating behavior. Current depressive episodes were associated with an increase in obesogenic eating behavior, both in consuming palatable food even without feeling hungry and in increasing food intake in response to negative emotions. As stated, these are obesogenic eating behavior and are related to higher weight status in children. Obesity harms physical and emotional health, both, during childhood, and in the long term. Thus, it is evident that it is important to include caregivers' mental health assessment in the management of eating behaviors that reflect actions for preventing childhood obesity.
References1. Freitas A, Albuquerque G, Silva C, Oliveira A. Appetite-Related Eating Behaviours: An Overview of Assessment Methods, Determinants and Effects on Children's Weight. Ann Nutr Metab. 2018; 73 (1): 19-29.
2. Scaglioni S, Arrizza C, Vecchi F, Tedeschi S. Determinants of children's eating behavior. Am J Clin Nutr. 2011; 94 (Supl. 6): S2006-11.
3. Webber L, Hill C, Saxton J, Van Jaarsveld CHM, Wardle J. Eating behaviour and weight in children. Int J Obes (Lond). 2009 Jan; 33 (1): 21-8.
4. Wardle J, Guthrie CA, Sanderson S, Rapoport L. Development of the Children's Eating Behaviour Questionnaire. J Child Psychol Psychiatry. 2001 Oct; 42 (7): 963-70.
5. Derks IPM, Bolhuis K, Sijbrands EJG, Gaillard R, Hillegers MHJ, Jansen PW. Predictors and patterns of eating behaviors across childhood: Results from The Generation R study. Appetite. 2019 Oct; 141: 104295.
6. Herle M, Stavola BD, Hübel C, Ferreira DLS, Abdulkadir M, Yilmaz Z, et al. Eating behavior trajectories in the first 10 years of life and their relationship with BMI. Int J Obes (Lond). 2020 Aug; 44 (8): 1766-75.
7. Jia P, Dai S, Rohli KE, Rholi RV, Ma Y, Yu C, et al. Natural environment and childhood obesity: A systematic review. Obes Rev. 2021 Feb; 22 (Supl. 1): e13097.
8. Scaglioni S, Salvioni M, Galimberti C. Influence of parental attitudes in the development of children eating behaviour. Br J Nutr. 2008 Feb; 99 (Supl. 1): S22-5.
9. El-Behadli AF, Sharp C, Hughes SO, Obasi EM, Nicklas TA. Maternal depression, stress and feeding styles: towards a framework for theory and research in child obesity. Br J Nutr. 2015 Jan; 113 (Supl. 1): S55-71.
10. Lindsay AC, Mesa T, Greaney ML, Wallington SF, Wright JA. Associations Between Maternal Depressive Symptoms and Nonresponsive Feeding Styles and Practices in Mothers of Young Children: A Systematic Review. JMIR Public Health Surveill. 2017 May; 3 (2): e29.
11. World Health Organization (WHO). Maternal mental health and child health and development in low and middle income countries. Geneva: WHO; 2008. [access in 2022 mar 10]. Available from:
https://www.who.int/publications/i/item/978924159714212. World Health Organization (WHO). Depression and Other Common Mental Disorders: Global Health Estimates. Geneva: WHO; 2017. [access in 2022 mar 10]. Available from:
https://apps.who.int/iris/handle/10665/25461013. Marsh S, Dobson R, Maddison R. The relationship between household chaos and child, parent, and family outcomes: a systematic scoping review. BMC Public Health. 2020 Apr; 20 (1): 513.
14. Hope S, Micali N, Deighton J, Law C. Maternal mental health at 5 years and childhood overweight or obesity at 11 years: evidence from the UK Millennium Cohort Study. Int J Obes (Lond). 2019 Jan; 43 (1): 43-52.
15. Marco PL, Valério ID, Zanatti CLM, Gonçalves H. Systematic review: Symptoms of parental depression and anxiety and offspring overweight. Rev Saúde Pública. 2020; 54: 49.
16. Martini MG, Barona-Martinez M, Micali N. Eating disorders mothers and their children: a systematic review of the literature. Arch Womens Ment Health. 2020 Aug; 23 (4): 449-67.
17. Reilly JJ, Armstrong J, Dorosty AR, Emmett PM, Ness A, Rogers I, et al. Early life risk factors for obesity in childhood: cohort study. BMJ. 2005; 330 (7504): 1357.
18. Amorim P. Mini International Neuropsychiatric Interview (MINI): validação de entrevista breve para diagnóstico de transtornos mentais. Rev Bras Psiquiatr. 2000; 22 (3): 106-15.
19. Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J,Weiller E, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I. ): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998; 59 (Suppl. 20): 22-33.
20. Viana V, Sinde S. O comportamento alimentar em crianças: Estudo de validação de um questionário numa amostra portuguesa (CEBQ). Análise Psicol. 2008; 26 (1): 111-120.
21. World Health Organization (WHO). Child growth standards. Geneva: WHO; 2008. [access in 2022 mar 10]. Available from:
https://www.who.int/childgrowth/software/en/22. Barros AJD, Victora CG. A nationwide wealth score based on the 2000 Brazilian demographic census. Rev Saúde Pública. 2005; 39 (4): 523-9.
23. Victora CG, Huttly SR, Fuchs SC, Olinto MT. The role of conceptual frameworks in epidemiological analysis: a hierarchical approach. Int J Epidemiol. 1997; 26 (1): 224-7.
24. Litchford A, Savoie Roskos MR, Wengreen H. Influence of fathers on the feeding practices and behaviors of children: A systematic review. Appetite. 2020 Apr; 147: 104558.
25. Wood AC, Blissett JM, Brunstrom JM, Carnell S, Faith MS, Fisher JO, et al. Caregiver Influences on Eating Behaviors in Young Children: A Scientific Statement From the American Heart Association. J Am Heart Assoc. 2020 May; 9 (10): e014520.
26. Boswell N, Byrne R, Davies PSW. Eating behavior traits associated with demographic variables and implications for obesity outcomes in early childhood. Appetite. 2018 Jan; 120: 482-90.
27. Miller AL, Gearhardt AN, Retzloff L, Sturza J, Kaciroti N, Lumeng JC. Early Childhood Stress and Child Age Predict Longitudinal Increases in Obesogenic Eating Among Low-Income Children. Acad Pediatr. 2018 Aug; 18 (6): 685-91.
28. Rodgers RF, Paxton SJ, McLean SA, et al. Maternal negative affect is associated with emotional feeding practices and emotional eating in young children. Appetite. 2014 Sep; 80: 242-7.
29. Herle M, Fildes A, Rijsdijk F, Steinsbekk S, Llewellyn C. The Home Environment Shapes Emotional Eating. Child Dev. 2018 Jul; 89 (4): 1423-34.
30. Craig L, Mullan K. How Mothers and Fathers Share Childcare: A Cross-National Time-Use Comparison. Am Sociol Rev. 2011; 76 (6): 834-61.
Received on April 19, 2022
Final version presented on October 17, 2022
Approved on October 31, 2022
Associated Editor: Lygia Vanderlei
Authors' contribution: Amaral PL, Mota JVS and Moreira FP: conception and design of the work; acquisition, analysis and interpretation of data, drafting and revising of the manuscript. Martins-Silva T and Jansen K: critical review of the content. Bach SL, Reyes AN and Silva RA: acquisition and analysis of the data. All authors approved the final version of the article and declare no conflicts of the interest.


 ; Karen Jansen2
; Karen Jansen2






 Ler em português
Ler em português