ABSTRACT
OBJECTIVES: to estimate the burden of parturients, fetuses and neonate's severe morbidity and mortality and investigate the association between maternal and their conceptus outcomes.
METHODS: retrospective cohort of 546 parturients and their conceptus in a university hospital, reference for high-risk pregnancy, in the metropolitan region II of Rio de Janeiro State from 2015 to 2017. We classified parturients according to obstetric morbidity (OM) in direct, indirect, or mixed, and their outcomes as: 1) no severity, 2) severe complication (SC), 3) critical intervention/Intensive Care Unit, and 4) greater severity -maternal near-miss (MNM) or death. We evaluated the conceptus as neonatal near-miss (NNM) and fetal and neonatal deaths. We estimated morbimortality indicators and associated factors (multinomial logistic regression).
RESULTS: OM was frequent: 29.3% indirect, 22.3% direct, and 15.8% mixed. There were eight cases of NMM, seven with direct MO. Among the conceptus: 7.5% were NNM cases and 4.4%, deaths. The risk of severe maternal outcomes was 16.8 and neonatal, 102.6/1000 live births. Mixed race, inadequate prenatal care, CG and NMM/death, were associated with NNM. Inadequate prenatal care and maternal NM/death were associated with conceptus deaths.
CONCLUSION: even in a reference unit, sociodemographic, and health care inequalities negatively affect mothers and, consequently, their children.
Keywords:
Pregnancy complications, Morbidity, Maternal and child health, Near miss, Prenatal care, Health status disparities
RESUMO
OBJETIVOS: estimar a carga de morbidade grave e mortalidade em parturientes, fetos e neonatos e investigar a associação entre os desfechos maternos e de seus conceptos.
MÉTODOS: coorte retrospectiva de 546 parturientes e seus conceptos no hospital universitário referência para gravidez de alto risco da região metropolitana II do estado do Rio de Janeiro (ERJ), de 2015 a 2017. Classificamos as parturientes segundo morbidade obstétrica (MO) em direta, indireta e mista, e seus desfechos como: 1) sem gravidade, 2) complicação grave (CG), 3) intervenção crítica/Unidade Terapia Intensiva e 4) maior gravidade-near miss materno (NMM) ou óbito. Avaliamos os conceptos quanto a near miss neonatal (NMN), óbitos fetais e neonatais. Estimamos indicadores de morbimortalidade, e fatores de associação (regressão logística multinomial).
RESULTADOS: MO foi frequente: 29,3% indiretas, 22,3% diretas e 15,8% mista. Ocorreram oito casos de NMM, sete com MO direta. Entre os conceptos,7,5% foram casos de NMN e 4,4%, óbitos. O risco de desfecho grave materno foi 16,8 e neonatal, 102,6 p/1000 nascidos vivos. Estiveram associados ao NMN: cor parda, pré-natal inadequado, CG e NMM/óbito; e ao óbito do concepto: pré-natal inadequado e NMM/óbito.
CONCLUSÃO: mesmo em situação de referência, desigualdades sociodemográficas e assistenciais afetam negativamente mães e, consequentemente, seus conceptos.
Palavras-chave:
Complicações na gravidez, Morbidade, Saúde materno-infantil, Near miss, Cuidado pré-natal, Desigualdades em saúde
IntroductionBetween healthy pregnancy and maternal death, there is a spectrum of morbid conditions, from mild to extremely severe.
1 Maternal death represents the tip of the iceberg of maternal dysfunctions resulting from the pregnancy-puerperal cycle: for each maternal death there is a larger number of women who, despite present severe clinical conditions, do not progress to death.
1 The World Health Organization (WHO) has proposed a classification of life-threatening conditions that may result in maternal survival - maternal near miss (MNM) - or death at the extreme end of the severity spectrum. Before constituting a threatening condition, severe maternal complications (of direct obstetric character), critical interventions, or intensive care unit admission should be monitored.
1The most current systematic review on MNM described a worldwide prevalence, between 2012 and 2018, of 18.6 cases of MNM per 1,000 live births (LB), with great variation between continents: 3.1 per 1,000 LB in Europe to 31.8 in Africa. Latin America had an intermediate value of 11.5 per 1,000 LB.
2A systematic review on MNM in Brazil from 2005 to 2016 identified high frequency and causes similar to those of maternal mortality: hypertensive diseases and hemorrhages.
3 The ratio of MNM varied among studies, highlighted those of national basis, with values between 9 and 10 cases per 1000 NL. Inequities, delay in health care, and the protective effect of adequate prenatal care were observed.
4Later studies show that MNM holds steady in the country. Hypertensive syndromes are the main cause and the most frequent associated factors are among mixed or black skinned, age (35 years and older), do not have a partner, low income, pre-existing diseases, absent or inadequate prenatal care, need to be transferred, lack of labor and/or cesarean section.
3,5-7 A time series, with national data from
Sistema de Internações Hospitalares do Sistema Único de Saúde (SIH-SUS) (Public Health System Hospital Admissions System) showed an increase in MNM in the country between 2010 and 2018, in addition to a higher frequency in the North and Northeast regions.
7The conditions that threaten maternal life in the gravidic-puerperal cycle can also impact the health of the conceptus, leading to the occurrence of serious outcomes such as neonatal near miss - NNM (neonate who presents a serious complication and survives the neonatal period)
8 and fetal and neonatal deaths.
9-17In low- and middle-income countries in Africa, Asia, and Latin America, higher rates of fetal, perinatal, and NNM death were observed in MNM cases.
10 A meta-analysis in high-income countries reported that women with severe maternal morbidities have a higher chance of perinatal death.
13 In both low- and high-income countries, unfavorable perinatal outcomes were more associated with bleeding complications.
11,13Also in Brazil, local and national studies corroborate the association of maternal near miss with negative perinatal outcomes (fetuses or neonates deaths), as well as newborn (NB) admitted to neonatal ICU.
14-17The present study estimated the burden of severe morbidity and mortality in parturient women and their conceptus and investigated the association between severe maternal outcomes and conceptus outcomes, in a public university hospital in metropolitan region II in Rio de Janeiro State, from 2015 to 2017.
MethodsThis was a retrospective cohort study of women admitted for childbirth and their conceptus at a maternity in a public university hospital, a reference for the metropolitan region II in Rio de Janeiro State. This is the only hospital in the region qualified at tertiary level for high-risk pregnancy (HRP).
18 All chldbirths that occurred from September 2015 to December 2017 were eligible, and multiple pregnancy deliveries were excluded from the analysis because they presented different risks of negative perinatal outcomes, especially for the second twin.
19 The follow-up period was from hospitalization for labor (mother) and birth (conceptus) until hospital discharge or death.The sample size was defined based on the study by Abalos et al.,
20 which used the following criteria to define the collection time: two months for locations with 6000 or more annual births, three months for locations between 6,000 and 3,000 annual births, and four months for locations with fewer than 3,000 annual births. In the years 2015, 2016, and 2017, 479, 402, and 402 childbirths occurred in HUAP, respectively, reaching a study population equal to 546 childbirths (mother and conceptus pairs).
Data on maternal and conceptus' medical history from the medical record, sociodemographic characteristics, reproductive history, pregnancy, childbirth and newborn history were from the Live Birth Declaration (LBD) or on the medical record (absence of DN for fetal death) were collected by the trained researchers. In cases of fetal, neonatal and maternal death, the causes of death were obtained from the Death Declaration (DD).
The maternal variables analyzed were: sociodemographic characteristics (age range: <20; 20-34 and ≥35 years; race/color: white, black, mixed, other and schooling: <8 and ≥8 years of schooling, has a partner: yes/no and paid occupation: yes/no), reproductive (no.of children had: 0, 1-3, ≥4), parity: primiparous/multiparous), morbidity pattern (direct and indirect obstetric morbidity) adequate prenatal care (yes/no)and type of childbirth (vaginal/cesarean). The adequacy of prenatal care considered the completion of the month of initiation, and the proportion of prenatal visits performed in relation to those recommended by gestational age
21 (adequate - adequate sum and more than adequate/inadequate - the others).
The pattern of maternal morbidity was defined according to Chou
et al.
22 These authors proposed to analyze maternal morbidity aligned with maternal mortality, classifying the condition as direct, indirect or combined obstetric.
Additionally, categories on maternal severity were created, adapting those proposed by WHO, according to Serruya
et al.
23Thus, maternal outcomes were classified in increasing order of severity: no severity (NS), severe maternal complication (SMC), critical intervention/ICU (IC/ICU), maternal near miss (MNM) and maternal death (MD).
1 When a woman developed more than one severe outcome, she was classified by the worst outcome.
Considering the low frequency of the maternal outcome according to the categories proposed by WHO,
2 the last three categories (IC/ICU, MNM and MD) represented outcomes of greater severity, for analysis, purposes were aggregated into a single category and contrasted with the category of lower risk (NS).
The fetuses and newborns' outcomes were ordered in increasing severity into: no serious outcome (NS), near miss (NM) and death (neonatal - N or fetal - F).
The validated definition of neonatal near miss was adopted (presence of at least one of three pragmatic criteria: 5th minute of Apgar score <7, birth weight <1500g and gestational age <32 weeks).
24The basic cause of death was assessed according to chapter and specific cause of the
Classificação Estatística Internacional de Doenças e Problemas Relacionados à Saúde 10a Revisão - CID 10 (WHO, 1995).
25 (International Statistical Classification of Diseases and Health-Related Problems 10th Revision). The presence of congenital anomaly in the MD and DD of neonatal and fetal's deaths was analyzed. Absolute frequencies of specific causes of deaths were calculated.
Absolute and relative frequencies of the study variables were described. Information incompleteness was assessed (excellent, <5; good, 5 to 10; regular, 10 to 20; poor, 20 to 50; and very poor, ≥50%).
26From the classification of the parturients according to the presence of obstetric morbidity, the absolute and relative percentage frequencies of occurrence of severe maternal and conceptus outcomes were calculated.
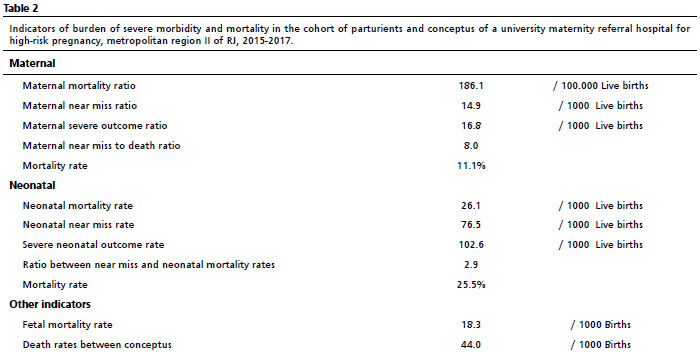
The following hospital indicators were calculated: Maternal Mortality Ratio, Maternal Near Miss Ratio, Severe Maternal Outcome Ratio, Ratio between Near Miss and Maternal Death, Maternal Mortality Rate, Neonatal Mortality Rate, Neonatal Near Miss Rate, Severe Neonatal Outcome Rate, Ratio between Near Miss and Neonatal Mortality Rates, Conceptus Mortality Index, Fetal Mortality Rate, and Conceptus Death Rate. The ratios of severe outcomes, were also calculated according to maternal characteristics.
Multinomial logistic regression models were used for severe maternal (main exposure: no morbidity/SMC/major severity) and conceptus (uncomplicated/ neonatal near miss /fetal and neonatal death) outcomes. For the choice of potentially confounding variables, in addition to literature,excellent completeness of information was considered.
26The selection of variables in the simple and multiple model, incorporating besides each covariate separately, the main exposure (severe maternal outcome, always present) followed the relevance in the outcome of natural history and/or the level of statistical significance less than 20%. In the multiple analysis with the variables selected previously, the level of statistical significance was less than 5%. To define the final multiple model, confounding variables were considered as those that caused changes greater than 10% in the magnitude of the odds ratio (OR) of the main exposure (severe maternal outcome).
Stata SE software (version 12) was used.
This study was approved by the Ethics Committee of the
Faculdade de Medicina da Universidade Federal Fluminense, opinion no. 1826053.
ResultsAmong the 546 parturients, 65% were from Niterói, 21.8% from São Gonçalo and 13.2% from other cities of the Metropolitan Region I and II. Women were predominantly 20-34 years old, mixed color, with 8 or more years of schooling, unmarried, unpaid and multiparous (Table 1). About 50% had an adequate prenatal care, and 60.4% had a cesarean delivery. Except for the variables, maternal schooling, paid occupation, and having a partner, the incompleteness of the information was excellent (<5%) (Table 1).
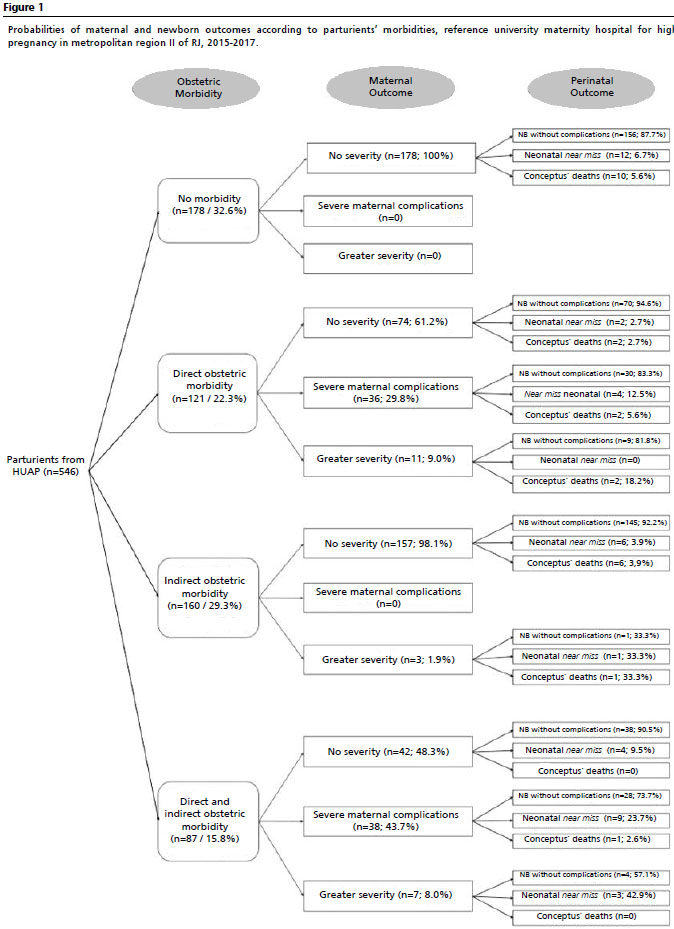
Figure 1 presents the classification of parturients regarding to obstetric morbidities and the conditional probabilities of serious maternal and perinatal outcomes.
Indirect obstetric morbidities were most frequent followed by direct (22.3%) and the combination of direct and indirect (15.8%). Among the direct ones, hypertensive syndromes of pregnancy predominated, followed by gestational diabetes (GD) and urinary tract infection (UTI). There were few cases of hemorrhage. In the presence of two or more direct morbidities, often the gestational hypertensive syndrome was one of the morbidities. As for the indirect ones, hypertension was the most frequent, and in the case of direct and indirect association, the superposition of gestational hypertensive syndrome to pre-existing hypertension was common.
All 178 women without morbidity evolved well. The occurrence of severe maternal complications was higher among women with direct and indirect obstetric morbidity (44.2%) and of more severe maternal outcomes among women with direct obstetric morbidity (9.8%). There were no cases of severe maternal complications among parturients with indirect obstetric morbidity. Four women required ICU admission, three for gestational hypertensive syndrome and one without obstetric morbidity, had Hodgkin's lymphoma, and passed away. Eleven women required hemotransfusion, including one case of NMM.
Eight cases of MNM were identified, seven with direct obstetric morbidity (five cases of gestational hypertensive syndrome) and one with chronic kidney disease. There was a predominance of clinical criteria (three cases of coagulopathy, one case of jaundice associated with gestational hypertensive syndrome and one of respiratory alterations). One maternal death (indirect cause) occurred during the study period, she had lymphoma.
Among the conceptus, 481 (88.1%) progressed without complications, 41 (7.5%) were classified as neonatal near miss, and there were 14 neonatal deaths (2.6%) and 10 fetal deaths (1.8%). Most conceptus of parturients without maternal morbidity and maternal outcome were without complications (87.6%). The occurrences of neonatal near miss and death were equal among the conceptus of mothers with higher severity outcome and indirect obstetric morbidity, and higher than the other categories (except NMN mixed obstetric morbidity and higher severity).
For every thousand live births there are about 15 cases of maternal near miss and 17 severe maternal outcomes (Table 2). Mortality among severe maternal outcomes was 11.1%. The rates of severe neonatal outcomes and conceptus mortality were 119 and 44 per 1,000 births, respectively. About three cases of neonatal near miss occurred for every neonatal death.
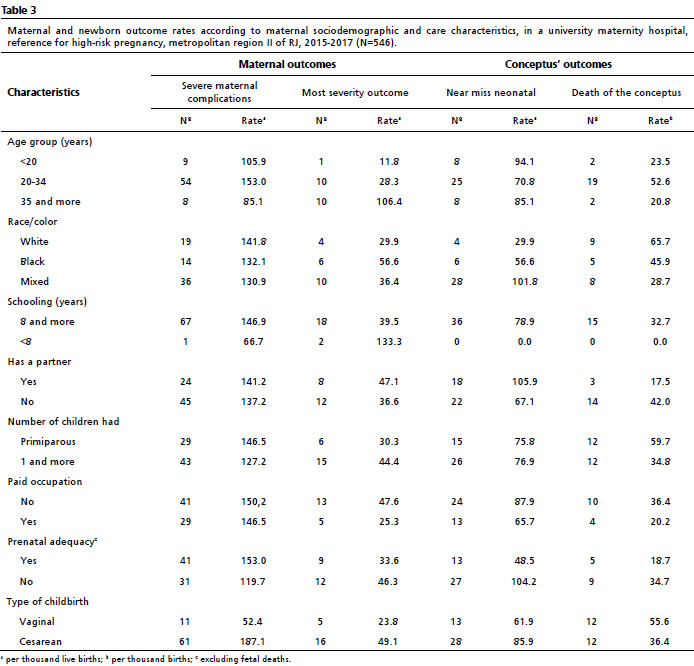
There was a higher risk of severe maternal complication (SMC) in women aged 20 to 34 years, white, with higher education, and primiparous, and for the outcome of greater severity (OGS), in those aged 35 years and older, black, with low education, and multiparous. Absence of paid occupation represented a higher risk for both maternal outcomes (Table 3). Women with inadequate prenatal care had higher rates of SMC, but not of OGS. Women who underwent cesarean section had higher rates of both outcomes (Table 3).
The highest rates of neonatal near miss occurred among conceptus of women 35 years or older, mixed color, unpaid, inadequate prenatal care, and cesarean section. The highest rates of death were among children of women 20 to 34 years old, white, primiparous, unpaid, inadequate prenatal care, and vaginal delivery (Table 3).
The parturient that evolved in maternal death, had unspecified Hodgkin's disease (code C81.9-ICD 10R) and other diseases and complicated disorders due to the pregnancy, childbirth and puerperium (code O99.8-ICD 10R), and this last cause, after coding and applying selection rules, was constant as underlying cause in the SIM.
As for the conceptus' deaths (n=28), three neonatal deaths were not found in the SIM, making it impossible to analyze them. Congenital malformations (Chapter XVII) predominated among neonatal deaths and did not occur as a basic cause among fetal deaths. All causes of fetal deaths were classified as Some Conditions Originating in the Perinatal Period (chapter XVI). As for specific causes, the most frequent underlying cause among conceptus was related to hypertensive syndromes of pregnancy (n=3), followed by underlying causes related to infectious and parasitic diseases of the mother and unspecified sepsis of the newborn.
In the simple regression model, only age group was not associated with the fetal outcomes. In the presence of severe maternal outcomes (main exposure), all covariates showed association with the outcome of the conceptus (
p<0.2): mixed color and inadequate prenatal care for both conceptus outcomes and age ≥35 years, only death and more severe maternal complications, only for neonatal near miss (Table 4). In the multiple model, only age group did not remain associated with conceptus outcome (
p≥0.05). Finally, mixed color mother, inadequate prenatal care, severe maternal complications, and severe maternal outcomes were associated with neonatal near miss; inadequate prenatal care and severe maternal outcomes were associated with conceptus death (Table 4).
DiscussionIn the cohort of parturients and their conceptus at the public university hospital in metropolitan region II in Rio de Janeiro State from 2015 to 2017, women with obstetric morbidities evolved more frequently to severe maternal outcomes that negatively impacted their conceptus' health.
Indirect obstetric morbidity was more frequent, an expected result, considering the referenced care of the university hospital, with high-risk prenatal care and several clinical specialties. Arterial hypertension stood out, as already shown for Latin America.
23The worst maternal outcomes (IC/ICU, MNM and MD) were more frequent among women with direct or combined obstetric morbidity. Pregnancy hypertensive syndromes were the most frequent morbidities in all severity categories. This result is in agreement with the national literature,
3-5,7 and is in line with that found for maternal mortality in Brazil.
27 In other low- and middle-income countries, bleeding disorders are more frequent causes of maternal death, with the exception of Latin America, where hemorrhage and hypertension are equivalent.
28The profile of causes of maternal death has been changing, reducing deaths from direct causes and increasing deaths from indirect causes, although this change is slow in the country.
27 Our assumption is that women were accompanied in the university hospital to have their pre-existing diseases well controlled, avoiding more unfavorable outcomes, while those with complications arose during the pregnancy may have been identified and/or referred late from the usual risk prenatal care to high-risk prenatal care.
The burden of severe maternal morbidity, expressed by the near miss rate of the analyzed hospital (14.9 p/1000 LB) was lower than another university hospital in Maceió, AL (54.8 p/1000 LB),
3 and higher than other places in the country where hospitals of different natures were included.
5,16,17 Two indicators that assess the quality of obstetric care - near miss/mortality ratio and mortality index - showed intermediate values when compared to other national studies.
3-5It should be emphasized that the only death that took place was a patient with cancer of unfavorable evolution, and this death cannot be attributed only to the poor quality of obstetric care. Therefore, these two indicators, which depend on the number of deaths, were impaired.
The high neonatal near miss rate found in the study, different from that found in six maternity hospitals in the states of Rio de Janeiro and São Paulo (TNNM between 6.2 and 35.9/1000 LB),
29 can be explained by the low frequency of births/year, as well as by being a reference unit for HRP. The severe neonatal outcomes rate was also high: 2.3 times the maximum rate found in the same study (50.3/1000 LB).
29Considering the relationship between mothers and their conceptus, severe maternal outcomes were associated with both neonatal near miss and infant deaths, while maternal complications were associated only with MNM. These results are similar to those found in the literature, but with more balance between fetal and neonatal deaths.
10,11,17 In these studies, the association with hemorrhagic complications and a greater impact on fetal deaths was emphasized, a fact not observed in the present study.
It is also noteworthy that there were no fetal deaths due to congenital malformation; however, deaths due to maternal conditions occurred among women with morbidity or who developed HRP. Among women without complications, deaths were from placental/ umbilical cord disorders. Although such conditions may be triggered by specific maternal conditions, such as hypertension, no maternal conditions that would classify them differently from "uncomplicated" were observed in the medical records. Therefore, it can be inferred that the death classification was adequate. Regarding neonatal death, the highest frequency was among women without complications, and all causes are related to the specific conditions of the newborn or to the malformation. Only among the women with morbidity, there were neonatal deaths related to maternal disorders, in addition to deaths due to malformation, which also occurred in this group of women. These results explain why the study observed a higher risk of death among conceptus in women without morbidity.
It is also worth noting the adequacy of prenatal care as a confounder of the association investigated. The relationship between prenatal care and negative outcomes for both women and fetuses is well documented.
3,4,6,10,14 In addition, maternal skin color was a confounder only for neonatal near miss: the chance of MNM among mixed color mothers was about four times higher than among white and black mothers, the latter without statistical significance.
29 The relationship between non-white color and occurrence of maternal near miss was described in a systematic review in national studies.
4The study of maternal and perinatal near miss has become increasingly necessary for public management, since its monitoring allows the timely to organize the health system.
1 Brazil has not incorporated the use of these markers in policies aiming at maternal and child health, as it occurred in Cuba.
30 However, there was the first recommendation for the incorporation of monitoring of maternal near miss criteria by health services in CIT Resolution Nº 1, March 30, 2021.
Although many public policies have been developed for the promotion of maternal and child health after the implementation of the
Sistema Único de Saúde (SUS) (Public Health System), there have been advances and setbacks throughout this period. Investing in women's health during the reproductive years is relevant not only for the women themselves, but for the impact on the health and development of the next generation. Furthermore, assertive policies will impact perinatal mortality rates and birth conditions in the country.
21This study has its limitations, we highlighted first, the low number of hospitalizations that occurred during data collection, caused by partial closure of the unit and that impaired the sample size. Additionally, regarding the quality of the information, two variables showed regular completeness: woman's schooling and occupation. These are variables that could broaden the understanding of socioeconomic conditions related to maternal death. The predominance of women with eight years or more of schooling was noteworthy, although many had no paid occupation. This result, different from that observed in other studies,
4 may be the result of bias information. Or perhaps the access to high-risk treatment, even mediated by vacancy regulation systems, reveals inequalities and women with higher educational levels find it easier to reach units such as the university hospital analyzed.
As a strength of the study, we point out the use of more expanded proposals for the classification of maternal morbidity, aligned to the classification of direct and indirect maternal deaths and the concept of severity gradient,
22,23 allowing deepening the knowledge of women's health and the impacts on child's health.
The results found corroborate socioeconomic, racial, and health care inequalities that negatively affect women's lives. The incorporation of the evaluation and monitoring, at least, of the near miss criteria by the health services, according to Resolution CIT No. 1, of 03/30/2021, will help future research. It is necessary that future studies consider the severity gradient and the classification of direct and indirect maternal morbidity. In conclusion, we reinforce the need for investments in women's health beyond reproductive health policies, ensuring healthy living conditions, redistribution of income, education, female empowerment, as well as equity in the health services.
References1. Organização Mundial da Saúde (OMS). Avaliação da Qualidade do Cuidado nas Complicações Graves da Gestação: A Abordagem do Near Miss da OMS para a Saúde Materna. Uruguay. OMS; 2011. [access in 2022 mar 2]. Available from:
https://www.paho.org/clap/dmdocuments/CLAP-Trad05pt.pdf2. Abdollahpour S, Heidarian Miri H, Khadivzadeh T. The global prevalence of maternal near miss: a systematic review and meta-analysis. Health Promot Perspect. 2019; 9 (4): 255-62.
3. Lima THB, Amorim MM, Kassar SB, Katz L. Maternal near miss determinants at a maternity hospital for high-risk pregnancy in northeastern Brazil: a prospective study. BMC Pregnancy Childbirth. 2019 Aug; 19 (1): 271.
4. Silva JMP, Fonseca SC, Dias MAB, Izzo AS, Teixeira GP, Belfort PP. Conceitos, prevalência e características da morbidade maternal grave e near miss materno no Brasil: uma revisão sistemática. Rev Bras Saúde Mater Infantil. 2018; 18 (1): 7-35.
5. Andrade MS, Bonifácio LP, Sanchez JAC, Oliveira-Ciabati L, Zaratini FS, Franzon ACA,
et al. Morbidade materna grave em hospitais públicos de Ribeirão Preto, São Paulo, Brasil. Cad Saúde Pública. 2020; 36 (7): e00096419.
6. Magalhães DMDS, Bernardes JM, Ruiz-Frutos C, Gómez-Salgado J, Calderon IMP, Dias A. Predictive Factors for Severe Maternal Morbidity in Brazil: A Case-Control Study. Healthcare (Basel). 2021; 9 (3): 335.
7. Herdt MCW, Magajewski FRL, Linzmeyer A, Tomazzoni RR, Domingues NP, Domingues MP. Temporal trend of near miss and its regional variations in Brazil from 2010 to 2018. Rev Bras Ginecol Obstet. 2021; 43 (2): 97-106.
8. Pileggi C, Souza JP, Cecatti JG, Faúndes A. Neonatal near miss approach in the 2005 WHO Global Survey Brazil. J Pediatr (Rio J). 2010; 86(1): 21-6.
9. Ronsmans C, Cresswell JA, Goufodji S, Agbla S, Ganaba R, Assarag B,
et al. Characteristics of neonatal near miss in hospitals in Benin, Burkina Faso and Morocco in 2012-2013. Trop Med Int Health. 2016 Apr; 21(4): 535-45.
10. Anggondowati T, El-Mohandes AA, Qomariyah SN, Kiely M, Ryon JJ, Gipson RF,
et al. Maternal characteristics, and obstetrical complications impact neonatal outcomes in Indonesia: a prospective study. BMC Pregnancy Childbirth. 2017; 17 (1): 100.
11. Tura AK, Scherjon S, van Roosmalen J, Zwart J, Stekelenburg J, van den Akker T. Surviving mothers and lost babies - burden of stillbirths and neonatal deaths among women with maternal near miss in eastern Ethiopia: a prospective cohort study. J Glob Health. 2020 Jun; 10 (1): 01041310.
12. Verschueren KJ, Kodan LR, Paidin RR, Samijadi SM, Paidin RR, Rijken MJ,
et al. Applicability of the WHO maternal near-miss tool: A nationwide surveillance study in Suriname. J Glob Health. 2020 Dec; 10 (2): 020429.
13. Mengistu TS, Turner JM, Flatley C, Fox J, Kumar S. The Impact of Severe Maternal Morbidity on Perinatal Outcomes in High Income Countries: Systematic Review and Meta-Analysis. J Clin Med. 2020 Jun; 9 (7): 2035.
14. Morse ML, Fonseca SC, Gottgtroy CL, Waldmann CS, Gueller E. Severe maternal morbidity and near misses in a regional reference hospital. Rev Bras Epidemiol. 2011; 14 (2): 310-22.
15. Oliveira LC, Costa AAR. Óbitos fetais e neonatais entre casos de near miss materno. Rev Assoc Med Bras. 2013; 59 (5): 487-94.
16. Dias MAB, Domingues RMSM, Schilithz AOC, Pereira MN, Diniz CSG, Brum IR,
et al. Incidência do Near Miss Materno no Parto e Pós-parto hospitalar: dados da pesquisa Nascer no Brasil. Cad Saúde Pública. 2014; 30 (Supl 1): S1-12.
17. Zanardi DM, Parpinelli MA, Haddad SM, Costa ML, Sousa MH, Leite DFB,
et al. Adverse perinatal outcomes are associated with severe maternal morbidity and mortality: evidence from a national multicentre cross-sectional study. Arch Gynecol Obstet. 2019 Mar; 299 (3): 645-54.
18. Secretaria de Estado de Saúde (RJ). Diagnóstico de Saúde da Região Metropolitana II. Rio de Janeiro; 2020. [access in 2022 mar 2]. Available from:
https://www.saude.rj.gov.br/comum/code/MostrarArquivo.php?C=MzUwNzU%2C19. Santana DS, Souza RT, Surita FG, Argenton JL, Silva CM, Cecatti JG. Twin Pregnancy in Brazil: A Profile Analysis Exploring Population Information from the National Birth E-Registry on Live Births. Biomed Res Int. 2018; 2018: 9189648.
20. Abalos E, Cuesta C, Carroli G, Qureshi Z, Widmer M, Vogel JP,
et al. Pre-eclampsia, eclampsia, and adverse maternal and perinatal outcomes: a secondary analysis of the World Health Organization Multicountry Survey on Maternal and Newborn Health. BJOG. 2014 Mar; 121 (Suppl. 1): 14-24.
21. Domingues RM, Hartz ZM, Dias MA, Leal MC. Avaliação da adequação da assistência pré-natal na rede SUS do Município do Rio de Janeiro, Brasil. Cad Saúde Pública. 2012; 28 (3): 425-37.
22. Chou D, Tunçalp Ö, Firoz T, Barreix M, Filippi V, von Dadelszen P,
et al. Constructing maternal morbidity - towards a standard tool to measure and monitor maternal health beyond mortality. BMC Pregnancy Childbirth. 2016 Mar; 16: 45.
23. Serruya SJ, Mucio B, Martinez G, Mainero L, Francisco A, Say L,
et al. Exploring the Concept of Degrees of Maternal Morbidity as a Tool for Surveillance of Maternal Health in Latin American and Caribbean Settings. Biomed Res Int. 2017; 2017: 8271042.
24. Kale PL, Jorge MHPM, Laurenti R, Fonseca SC, Silva KSD. Pragmatic criteria of the definition of neonatal near miss: a comparative study. Rev Saúde Pública. 2017; 51: 111.
25. Organização Mundial da Saúde (OMS). Classificação Estatística Internacional de Doenças e Problemas Relacionados à Saúde - 10ª Revisão. São Paulo: CBCD/ EDUSP; 1995. v I e II.
26. Romero DE, Cunha CB. Avaliação da qualidade das variáveis socioeconômicas e demográficas dos óbitos de crianças menores de um ano registrados no Sistema de Informações sobre mortalidade do Brasil (1996/2001). Cad Saúde Pública. 2006; 22 (3): 673-84.
27. Pacagnella RC, Nakamura-Pereira M, Gomes-Sponholz F, Aguiar RALP, Guerra GVQL, DCSG,
et al. Maternal Mortality in Brazil: ProposalsandStrategies for its Reduction. Rev Bras Ginecol Obstet. 2018; 40 (9): 501-6.
28. Say L, Chou D, Gemmill A, Tunçalp Ö, Moller AB, Daniels J,
et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014; 2 (6): e323-33.
29. Kale PL, Mello-Jorge MHP, Silva KSD, Fonseca SC. Neonatal near miss and mortality: factors associated with life-threatening conditions in newborns at six public maternity hospitals in Southeast Brazil. Cad Saúde Pública 2017; 33: e00179115.
30. Rodríguez MS, Mancha YZ. Informatización del sistema de vigilancia de la Morbilidad Materna Extremadamente Grave en Cuba. Rev Ciencias Médicas de Pinar del Río. 2018; 22 (1): 85-91.
Received on April 25, 2022
Final version presented on October 8, 2022
Approved on December 12, 2022
Associated Editor: Leila Katz
Authors' contribution: Silva JMP, Kale PL, Fonseca SC: Conceptualization (Equal), Data curation (Equal), Formal analysis (Equal), Research (Equal), Methodology (Equal), Software (Equal), Validation (Equal), Writing - original draft (Equal), Writing - review & writing (Equal). Nantes T, Alt NN: Data curation (Equal), Research (Equal), Software (Equal), Visualization (Equal).
The authors have approved the final version of the article and declare no conflict of interest.


 ; Pauline Lorena Kale2
; Pauline Lorena Kale2







 Ler em português
Ler em português