ABSTRACT
OBJECTIVES: to analyze the influence of breastfeeding duration on eating behavior in children aged two to six years.
METHODS: this review was conducted by PRISMA guidelines. SciELO, Lilacs, Embase, and PubMed databases were researched by using a specific syntax, for studies published from 2000 to 2020. The Joanna Briggs Institute Critical Appraisal checklist was used to assess the risk of study bias.
RESULTS: a total of 26,211 articles were identified, of which seven were included in the study. The results showed a significant association in four studies. All authors used their own questionnaires to assess breastfeeding exposure; there was no standard classification of exclusive and total breastfeeding duration. The breastfeeding duration was associated with reduced food neophobia, lower scores on the food responsiveness subscale, and lower 'picky eating' behavior. Validated instruments were predominantly used to assess the outcome of eating behavior; however, this assessment was not similar between studies.
CONCLUSION: a significant association was observed between breastfeeding duration and eating behavior in children aged two to six years. Further research should be conducted to describe the mechanisms involved in this association.
Keywords:
Breastfeeding, Eating behavior, Child, Systematic review
RESUMO
OBJETIVOS: analisar a influência da duração do aleitamento materno no comportamento alimentar em crianças de dois a seis anos.
MÉTODOS: esta revisão foi conduzida de acordo com as diretrizes PRISMA. As bases de dados SciELO, Lilacs, Embase e PubMed foram pesquisadas usando uma sintaxe específica, para estudos publicados de 2000 a 2020. O Joanna Briggs Institute Critical Appraisal checklist foi utilizado para avaliar o risco de viés do estudo.
RESULTADOS: foram identificados 26.211 artigos, dos quais sete foram incluídos no estudo. Os resultados mostraram associação significativa em quatro estudos. Todos os autores usaram seus próprios questionários para avaliar a exposição à amamentação; não havia uma classificação padrão de duração do aleitamento materno exclusivo e total. A duração do aleitamento materno foi associada à redução da neofobia alimentar, menores escores na subescala de responsividade alimentar e menor comportamento alimentar exigente. Instrumentos validados foram usados predominantemente para avaliar o resultado do comportamento alimentar, no entanto, essa avaliação não foi semelhante entre os estudos.
CONCLUSÃO: observou-se associação significativa entre a duração da amamentação e o comportamento alimentar em crianças de dois a seis anos. Mais pesquisas devem ser realizadas para descrever os mecanismos envolvidos nesta associação.
Palavras-chave:
Amamentação, Comportamento alimentar, Criança, Revisão sistemática
IntroductionThe eating behavior is defined as a complex interaction of physiological (e.g., hunger and satiety), psychological (e.g., learned food preferences, knowledge, and motivations), environmental (e.g., availability of food, the context in which food is provided, size of the plate or portions) and genetic (e.g., preference acquired in early life for sweet or salty flavors) factors.
1,2 Eating behavior is indirectly molded by observing others' influences,
2 for example, the family members' eating behavior serves as a model for the child's development and his/her eating behavior.
3Childhood is a critical period for establishing adequate eating habits. It is assumed that self-regulatory eating preferences and behaviors are influenced by infant feeding practices.
4 The first sensory experiences occur when there is a transfer of flavors in the amniotic fluid in the uterus, influenced by maternal feeding,
4-6 and the child continues experiencing flavors through human milk.
7 Because of the importance of human milk for a child's health, the World Health Organization (WHO) recommended that children should be exclusively breastfed for up to six months of life and that breastfeeding should be continued until two years of age or longer.
8 Later on, children who had received human milk had a better acceptance of certain foods, such as fruit and vegetables.
9,10 In the preschool stage, from two to six years of age, children generally have a more stable growth rate and nutrition has less influence on growth during this period,
11 occurring as an expected adaptive response to decreasing appetite.
12 In childhood, eating behavior traits are associated with important health outcomes, such as anthropometric indicators,
13 cardiometabolic risk biomarkers,
14 adiposity,
15 'picky eating' with lower vegetable consumption,
16 and eating disorders.
17The association of eating behavior in childhood with short- and medium-term health outcomes motivated the creation and validation of numerous instruments for assessing eating behavior in children.
18 Among these instruments are The Children's Eating Behavior Questionnaire (CEBQ),
19 Preschooler Feeding Questionnaire (PFQ),
20 Infant Feeding Questionnaire (IFQ),
21 Nutrition Screening Tool for Every Preschooler (NutriSTEP)
22 and Oregon Research Institute Child Eating Behavior Inventory (ORI-CEBI).
5The CEBQ, a self-administered questionnaire, contains 35 questions divided into eight subscales so that four subscales investigate behaviors that reflect the 'food approach' and the other four subscales reflect behaviors related to 'food avoidance', where parents report the occurrence of specific eating behavior in their children in Likert scale of five points, with the score ranging from one to five: never (1), rarely (2), sometimes (3), often (4) and always (5).
14 PFQ assesses children's nutrition during the preschool years and the questionnaire items were designed to explore constructs about infant feeding practices and overweight.
20 IFQ is a self-administered 28-item questionnaire that measures maternal dietary practices and beliefs and is used to assess infant feeding during early childhood.
21 NutriSTEP is a screening tool designed to identify children aged three to five years who are at nutritional risk.
22 Finally, the ORI-CEBI addresses the following constructs: interactions during child feeding times, child and parent affection during feeding, refusal to eat, selective feeding, restrictive feeding, overfeeding, and problematic eating behavior.
5Previous studies evaluating the impacts of eating behavior in children have shown that 'picky eating' behavior is associated with low micronutrient intake, increased risk of low weight and growth in the first years of life, and overweight and obesity in adolescents.
22 Additionally, a study conducted in Brazil with 335 children showed that the subscale of the questionnaire 'food approach', by CEBQ questionnaire, was associated with being overweight in childhood.
6The purpose of this systematic review was to analyze the influence of breastfeeding duration on eating behavior in children aged two to six years.
MethodsEating behavior is a complex term with several different focuses, thus, for this review, the expression was considered the set of actions or attitudes that are related to the act of eating, not being defined as a preference, habit, or acceptance of a particular food.
This systematic review was first conducted in November 2018 and updated in October 2020. The research protocol was previously registered in the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD42019118773 and conducted according to the Preferred Reporting Items for Protocol Systematic Reviews and Meta-Analysis (PRISMA).
23 This research was carried out using a search strategy with terms selected from Health Sciences Descriptors (DeCS) and Medical Subject Headings (MeSH): 'eating behavior', 'breastfeeding', and 'early childhood', that characterized the research question structured according to the population, exposure, comparison, and outcome (PECO) method (Table 1). A thorough literature search was performed in the following databases: Scientific Electronic Library Online (SciELO),
Literatura Latino-Americana e do Caribe de Ciências da Saúde (Lilacs), Embase, and PubMed.
The inclusion criteria were: (i) studies published from 2000 to 2020, (ii) clinical studies in humans and studies with children aged up to six years, and (iii) studies that relate exclusive and/or total breastfeeding duration with eating behavior - regardless of whether there was an association or not. While the exclusion criteria were: (i) studies published in languages other than Portuguese, English, or Spanish, and (ii) and studies with a population with comorbidities that affected eating behavior.
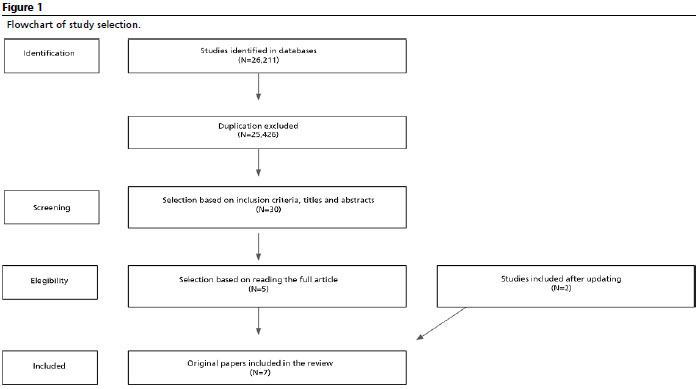
The study selection process consisted of four steps: identification and exclusion of duplicate articles, screening of articles (inclusion criteria and reading titles and abstracts), evaluating entire papers for eligibility, and selecting articles for inclusion in the review. The identified articles were independently assessed by three researchers (BCE, GLC and MBM). Any disagreements were resolved through discussion. A flowchart of the study selection process is presented in Figure 1.
The Joanna Briggs Institute (JBI) Critical Appraisal tools
24 were used to assess the methodological quality of the studies. Specifically, JBI critical appraisal checklist for cohort and cross-sectional studies were used (Table 2). In the JBI critical appraisal checklist, each question has four answer options: yes (Y), no (N), unclear (U), and not applicable (NA). The checklist for cohort and cross-sectional studies has 11 and eight items, respectively.
ResultsThe initial search yielded a total of 26,211 publications. After excluding duplicates, 25,426 remained. These were screened using the inclusion criteria of the present review by reading titles and abstracts. This screening resulted in the exclusion of 25,396 articles, resulting in 30 articles. The articles were read in full and subsequently, 25 were excluded for the following reasons: the article was a narrative review (n=1), the article was a conference summary (n=1), participants were younger or older than the specified age group (n=12), discordant exposure (n=3) and different outcomes (n=8), resulting in five studies for review. After updating the search, two publications were added, for a total of seven studies.
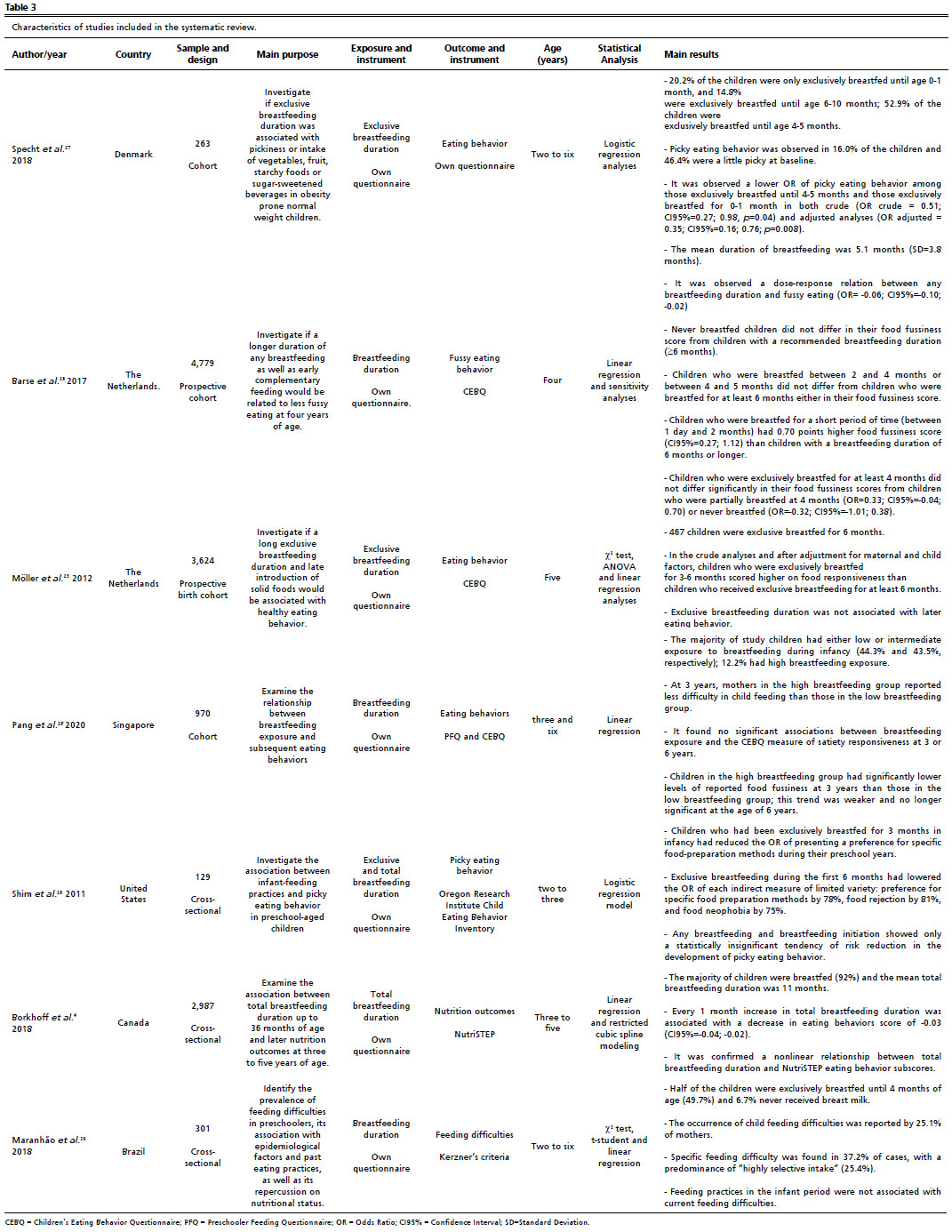
The seven studies included were reviewed and data were extracted (Table 3). The studies that met the inclusion criteria were published from 2011 to 2020 and included four cohort studies
25-28 and three cross-sectional studies.
4,29,30 The total number of study participants was 13,053, with a range of 129
30 to 4,779
26 children. The ages ranged from two to six years. Participants were evaluated from different countries, including Holland,
5,26 Denmark,
27 Brazil,
30 Canada,
4 the United States
29 and Singapore.
28 All authors developed their own questionnaires to assess breastfeeding duration,
4,28,29 and there was no standard classification of exclusive or total breastfeeding duration. Specht
et al. 27 categorized exclusive breastfeeding (EBF) as 0-1 month, 2-3 months, 4-5 months, and 6-10 months, Barse
et al. 26 categorized breastfeeding (BF) as 0-2 months, 2-4 months, 4-6 months, and ≥6 months, and EBF was categorized as never breastfed, partially breastfed, and exclusively breastfed. In the study by Shim
et al. ,
29 EBF was categorized for 3 months and 6 months. Borkhoff
et al. 4 evaluated the total duration of BF as a continuous variable and used the following cut off points for analysis: no breastfeeding, 0-6 months, 6-12 months, 12-18 months, 18-24 months, and 24-36 months. The duration of EBF, in Möller
et al. 25 study was categorized as no breastfeeding and <1, 1-2, 3-6, and ≥6 months. Pang
et al. 28 classified exposure to breastfeeding as low (EBF <3 months), intermediate (EBF 3-4 months), or high (EBF >4 months). Finally, Maranhão
et al. 30 categorized EBF into ≤6 months and >6 months.
The instruments validated to assess eating behavior were: CEBQ, PFQ, and Kerzner's criteria.
25,26,30 The other three studies used their own questionnaires,
4,27,29 and of these, two evaluated the outcome through 'picky eating' behavior
27,29 and the other used the NutriSTEP
4 eating behavior scale and subscale. Studies that used the CEBQ assessed eating behavior through the subscales: 'food fussiness',
25,28 and 'satiety responsiveness'.
25 All studies considered variables such as maternal age, maternal schooling, sex of the child, gestational age, and birth weight to perform adjustments to the statistical analyses.
4,25-30Given that a higher NutriSTEP score indicates greater nutritional risk, Borkhoff
et al. 4 demonstrated an association between eating behavior and (i) decreasing trend in NutriSTEP score for children who were breastfed for 0-6 months (β= -0.14; CI95%= -0.29; 0.004), (ii) significant decrease in NutriSTEP score for children breastfed for 6-12 months (β= -0.20; CI95%= -0.33; -0.07) and no significant change after 12 or more months of breastfeeding (β= 0.09; CI95%= -0.07; 0.24).
Shim
et al. 29 demonstrated that children who were breastfed exclusively for 6 months had lower odds of developing (i) food rejection odds ratio (OR)=0.19 (CI95%=0.06; 0.69) and (ii) food neophobia OR=0.25 (CI95%=0.07; 0.89).
Maranhão
et al. 30 study found no statistically significant association between BF, >6 months and ≤6 months (
p=0.58) and eating behavior. The researchers used a convenience sample and did not present statistical power in the methodology. In addition, EBF was assessed retrospectively, which increases the risk of recall bias as eating behavior was assessed in children aged two to six years.
However, Möller
et al. 25 found an association between EBF duration and the eating behavior of five-year-olds in the adjusted analysis. The authors observed that children who were EBF between 1-2.9 months had a lower 'food responsiveness' score β 0.03 (CI95%=0.01; 0.06).
Barse
et al. 26 observed the dose-response relation between any BF and 'fussy eating' β 0.06 (CI95%=-0.10; -0.02). However, never-breastfed children did not differ in their food agitation score from children with a recommended BF duration (≥6 months). The authors did not present the statistical power of the study as the original study was designed to assess other outcomes.
Specht
et al. 27 found a lower OR (OR adjusted = 0.35; CI95%=0.16; 0.76;
p=0.008) of picky eating behavior in children with EBF for 4-5 months in a sample at risk for overweight and mothers with low socioeconomic status. Additionally, 51% (n=280) of the original sample was excluded for having missing information, with 221 breastfeeding data and 59 for the outcome variable (picky eating behavior), and 41% for having missing data at the 15-month follow-up. The authors did not present the statistical power and report in the methodology that they classified children as picky and non-picky to analyze the main outcome.
Additionally, Pang
et al. 28 investigated the outcome in a cohort study that applied different questionnaires at follow-up. The adjusted analyzes showed a statistically significant lower difficulty in child feeding β -0.2 (CI95%=-0.4; 0.0) and 'food fussiness' β -0.38 (CI95%= -0.70; -0.06) at 3 years of age in children with EBF for 4 months and supplemented for 6 months.
Of the seven studies included, four of them demonstrated that EBF or BF duration had a positive effect on children's eating behavior, such as healthier eating behavior,
4 reduced food neophobia, lower scores on the 'food responsiveness' subscale
25 and lower 'picky eating' behavior.
27DiscussionThis systematic review identified seven studies that assessed the influence of breastfeeding duration on infant feeding behavior in children aged two to six years. Four studies demonstrated a positive association outcome such as healthier eating behavior,
4 reduced food neophobia, lower scores on the 'food responsiveness' subscale
25 and lower 'picky eating' behavior.
27Researchers differ in their definition of exposure to breastfeeding, and their assessment of this exposure. Specht
et al. 27 and Möller
et al. 25 evaluated EBF, whereas Shim
et al. 29 and Borkhoff
et al. 4 did not differentiate between EBF and non-EBF, and Borkhoff
et al. 4 assessed BF duration. However, it is important to highlight the risk of memory bias present in retrospective assessments.
Different methods of analyzing eating behavior outcomes were also used. Of the four studies that found a positive association, Möller
et al. 25 and Borkhoff
et al. 4 applied a validated instrument, respectively: the CEBQ, where only four of the eight scales were used, and the NutriSTEP, where only one scale was applied to assess the outcome, losing its validation. The other two studies used their own questionnaires, which depended on the parent's perception of their children's eating behavior.
27,29All the studies that found no association
25,28,30 evaluated EBF. Barse
et al. 26 and Pang
et al. 28 also evaluated the total BF duration, and exposure was assessed through regular interviews during the child's first year of life, without risk of memory bias, unlike Maranhão
et al. 30 study that measured the exposure retrospectively and did not clearly describe how this measurement was performed.
Eating behavior was assessed by the included studies using validated instruments. Barse
et al. 26 used the CEBQ, but only the food agitation scale. Pang
et al. 28 used the PFQ and CEBQ, but only two scales for each instrument (food difficulty and concerns about eating and response to satiety and food agitation, respectively). Maranhão
et al. 30 used the Krezner criteria. There is no variation in the criteria used to evaluate eating behavior in these studies, but two authors used fewer scales of validated instruments than studies that found an association between breastfeeding and eating behavior. It is important to mention that Barse
et al. 26 declared the existence of a conflict of interest due to a relationship with a company producing artificial milk substituted for human milk.
A critical analysis of the studies allowed the identification of several limitations. First, the use of different methods to assess exposure and outcome caused a lack of standardization among the studies. Second, there were differences in the sample sizes among the studies and a significant range in age at which the outcome was assessed. Third, the results of the studies might have been affected by memory bias for information collected retrospectively. And for last, there might have been flaws in the parental perception of children's eating behavior. In early childhood, there is a slowdown in growth and an adaptive food neophobia, and the child may not meet parental expectations, causing a distorted view of them in relation to feeding.
11,23 We believe that these limitations are not enough to disconsider the findings of this review, due to the importance of eating behavior in early childhood obesity prevention.
31Despite strong evidence of the benefits of BF in relation to short- and long-term health outcomes,
9 the results described above highlight the need for more research using validated questionnaires to assess feeding behavior, prospective research, and accurate measures of breastfeeding (exclusive and total) to understand the mechanisms involved. An important question is whether BF as a behavior-modifying factor can be weakened or canceled over time, especially after three years of age, by other environmental factors to which the child is exposed, such as parental care style, parents' food behavior, and the social environment. The development of eating behavior is a complex process of biological and cultural nature, which makes the study of this phenomenon challenging for researchers.
Most of the studies evaluated in this systematic review (four out of seven) showed a positive association (healthier eating behaviors, reduced food neophobia, lower 'food responsiveness', and lower 'picky eating' behavior) between BF duration and infant feeding behavior in children aged two to six years. There is a clear need for more homogeneous studies on this topic to understand the complexity of the mechanisms involved in this association.
References1. Birch LL. Development of food preferences. Annu Rev Nutr. 1999; 19: 41-62.
2. LaCaille L. Eating Behavior. In: Gellman MD, Turner JR (eds) Encyclopedia of Behavioral Medicine. New York: Springer; 2013. p. 641-2.
3. Yelverton CA, Geraghty AA, O'Brien EC, Killeen SL, Horan MK, Donnelly JM,
et al. Breastfeeding and maternal eating behaviours are associated with child eating behaviours: findings from the ROLO Kids Study. Eur J Clin Nutr. 2021 Apr; 75 (4): 670-9.
4. Borkhoff CM, Dai DWH, Jairam JA, Wong PD, Cox KA, Maguire JL,
et al. Breastfeeding to 12 mo and beyond: nutrition outcomes at 3 to 5 y of age. Am J Clin Nutr. 2018 Aug; 108 (2): 354-62.
5. Spahn JM, Callahan EH, Spill MK,
et al. Influence of maternal diet on flavor transfer to amniotic fluid and breast milk and children's responses: a systematic review. Am J Clin Nutr. 2019 Mar; 109 (Suppl. 7): S1003-26.
6. Forestell CA. Flavor Perception and Preference Development in Human Infants. Ann Nutr Metab. 2017; 70 (Supl. 3): 17-25.
7. Mennella JA, Reiter AR, Daniels LM. Vegetable and Fruit Acceptance during Infancy: Impact of Ontogeny, Genetics, and Early Experiences. Adv Nutr. 2016 Jan; 7 (1): S211-9.
8. World Health Organization (WHO). Recommendations on child health guidelines approved by the WHO guidelines review committee. Geneva: WHO; 2017. [access in 2022 Fev 10]. Available from:
https://apps.who.int/iris/handle/10665/2592679. Mennella JA, Daniels LM, Reiter AR. Learning to like vegetables during breastfeeding: a randomized clinical trial of lactating mothers and infants. Am J Clin Nutr. 2017 Jul; 106 (1): 67-76.
10. Beckerman JP, Slade E, Ventura AK. Maternal diet during lactation and breast-feeding practices have synergistic association with child diet at 6 years. Public Health Nutr. 2020 Feb; 23 (2): 286-94.
11. Benyi E, Sävendahl L. The Physiology of Childhood Growth: Hormonal Regulation. Horm Res Paediatr. 2017; 88 (1): 6-14.
12. Taylor CM, Emmett PM. Picky eating in children: causes and consequences. Proc Nutr Soc. 2019 May; 78 (2): 161-9.
13. Dalrymple KV, Flynn AC, Seed PT, Briley AL, O'Keeffe M, Godfrey KM,
et al. Associations between dietary patterns, eating behaviors and body composition and adiposity in 3-year-old children of mothers with obesity. Pediatr Obes. 2020 May; 15 (5): e12608.
14. Warkentin S, Santos AC, Oliveira A. Associations of appetitive behaviors in 7-year-old children with their cardiometabolic health at 10 years of age. Nutr Metab Cardiovasc Dis. 2020 May; 30 (5): 810-21.
15. Kininmonth A, Smith A, Carnell S, Steinsbekk S, Fildes A, Llewellyn C. The association between childhood adiposity and appetite assessed using the Child Eating Behavior Questionnaire and Baby Eating Behavior Questionnaire: A systematic review and meta-analysis. Obes Rev. 2021 May; 22 (5): e13169.
16. Sandvik P, Ek A, Eli K, Somaraki M, Bottai M, Nowicka P. Picky eating in an obesity intervention for preschool-aged children - what role does it play, and does the measurement instrument matter? Int J Behav Nutr Phys Act. 2019 Sep; 16 (1): 76
17. Herle M, Stavola B, Hübel C, Abdulkadir M, Ferreira DS, Loos RJF,
et al. A longitudinal study of eating behaviours in childhood and later eating disorder behaviours and diagnoses. Br J Psychiatry. 2020 Feb; 216 (2): 113-9.
18. D'avila HF, Cás S, Mello ED. Tools to evaluate eating behaviour of children and adolescents. DEMETRA. 2020; 15: e40131.
19. Wardle J, Guthrie CA, Sanderson S, Rapoport L. Development of the Children's Eating Behaviour Questionnaire. J Child Psychol Psychiatry. 2001 Oct; 42 (7): 963-70.
20. Baughcum AE, Powers SW, Johnson SB,
et al. Maternal feeding practices and beliefs and their relationships to overweight in early childhood. J Dev Behav Pediatr. 2001; 22 (6): 391-408.
21. Randall Simpson JA, Keller HH, Rysdale LA, Beyers JE. Nutrition Screening Tool for Every Preschooler (NutriSTEP): validation and test-retest reliability of a parent-administered questionnaire assessing nutrition risk of preschoolers. Eur J Clin Nutr. 2008 Jun; 62 (6): 770-80.
22. Taylor CM, Emmett PM. Picky eating in children: causes and consequences. Proc Nutr Soc. 2019; 78 (2): 161-9.
23. Shamseer L, Moher D, Clarke M,
et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation BMJ. 2015; 350: g7647. [published correction appears in BMJ. 2016; Jul 21; 354: i4086].
24. Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetcu R,
et al. Chapter 7: Systematic reviews of etiology and risk. In: Aromataris E, Munn Z (eds). JBI Manual for Evidence Synthesis. The Joanna Briggs Institute; 2017. [access in 2022 Fev 10]. Available from:
https://synthesismanual.jbi.global25. Möller LM, Hoog ML, van Eijsden M, Gemke RJ, Vrijkotte TG. Infant nutrition in relation to eating behaviour and fruit and vegetable intake at age 5 years. Br J Nutr. 2013 Feb; 109 (3): 564-71.
26. Barse LM, Jansen PW, Edelson-Fries LR, Jaddoe VWV, Franco OH, Tiemeier,
et al. Infant feeding and child fussy eating: The Generation R Study. Appetite. 2017 Jul; 114: 374-81.
27. Specht IO, Rohde JF, Olsen NJ, Heitmann BL. Duration of exclusive breastfeeding may be related to eating behaviour and dietary intake in obesity prone normal weight young children. PLoS One. 2018 Jul; 13 (7): e0200388.
28. Pang WW, McCrickerd K, Quah PL, Fogel A, Aris IM, Yuan WL,
et al. Is breastfeeding associated with later child eating behaviours? Appetite. 2020 Jul; 150: 104653.
29. Shim JE, Kim J, Mathai RA; STRONG Kids Research Team. Associations of infant feeding practices and picky eating behaviors of preschool children. J Am Diet Assoc. 2011 Sep; 111 (9): 1363-8.
30. Maranhão HS, Aguiar RC, Lira DTJ, Sales MUF, Nóbrega NADN. Feeding difficulties in preschool children, previous feeding practices, and nutritional status. Rev Paul Pediatr. 2017 Oct; 36 (1): 7.
31. Grammer AC, Balantekin KN, Barch DM, Markson L, Wilfley DE. Parent-Child influences on child eating self-regulation and weight in early childhood: A systematic review. Appetite. 2022 Jan: 1; 168: 105733.
Received on March 14, 2022
Final version presented on September 5, 2022
Approved on September 21, 2022
Associated Editor: Ana Ortigoza
Authors' contribution: Ergang BC, Caprara GL, Machado MB: writing, data analysis and review of the manuscript. Moreira PR: writing and review of the manuscript. Hagen MEK: review of the manuscript. Bernardi JR: review of the manuscript and research guidance.
The authors approved the final version of the article and declare no conflict of interest.


 ; Gabriele Luiza Caprara2
; Gabriele Luiza Caprara2







 Ler em português
Ler em português