ABSTRACT
OBJECTIVES: to evaluate the use of iron supplementation and associated factors in children aged six to 59 months attended at the Family Health Strategy units in a city in Minas Gerais (MG).
METHODS: a cross-sectional, analytical-exploratory study, carried out with 252 children aged six to 59 months, attended at ten units, between 2014 and 2016. A structured questionnaire was used to collect data on socioeconomic conditions, maternal health, child's health and the knowledge of those responsible regarding anemia and iron supplementation, in addition to analysis of the child's medical records /booklet to collect test results. Descriptive statistics, bivariate association analysis and logistic regression for multivariate analysis were performed.
RESULTS: only 22.6% of the children aged between six and 24 months were receiving iron supplement at the time of the interview. Considering children aged six to 59 months, 13.1% were supplemented and breastfeeding time (p=0.006) and the participation in childcare (p=0.042), were positively associated with the use of supplementation.
CONCLUSION: most children aged six to 24 months were not receiving supplementation as recommended by the Ministry of Health, demonstrating the need to implement prevention programs, such as the National Iron Supplementation Program and training of professionals on the importance of health education in preventing childhood anemia.
Keywords:
Anemia, Iron deficiency, Nutritional supplement, Breastfeeding, Child care
RESUMO
OBJETIVOS: avaliar o uso do suplemento de ferro e fatores associados em crianças de seis a 59 meses atendidas em unidades Estratégia Saúde da Família em município de Minas Gerais (MG).
MÉTODOS: estudo transversal, analítico-exploratório, realizado com 252 crianças na faixa etária seis a 59 meses, atendidas em dez unidades, entre 2014 e 2016. Utilizou-se questionário estruturado para coleta de dados sobre condições socioeconômicas, saúde materna, saúde da criança e conhecimentos dos responsáveis acerca da anemia e suplementação com ferro, além de análise do prontuário / caderneta da criança para coleta de resultados de exames. Realizou-se análise estatística descritiva, análise de associação bivariada e regressão logística para análise multivariada.
RESULTADOS: apenas 22,6% das crianças com idade entre seis e 24 meses estavam recebendo o suplemento de ferro no momento da entrevista. Considerando as crianças de seis a 59 meses, 13,1% eram suplementadas e o tempo de amamentação (p=0,006) e a participação na puericultura (p=0,042) apresentaram associação com o uso de suplemento.
CONCLUSÃO: a maioria das crianças de seis a 24 meses não recebia a suplementação, demonstrando a necessidade de implementação dos programas de prevenção, como o Programa Nacional de Suplementação de Ferro e capacitação dos profissionais sobre a importância da educação em saúde para prevenção da anemia infantil.
Palavras-chave:
Anemia, Deficiência de ferro, Suplemento nutricional, Aleitamento materno, Cuidado da criança
IntroductionAccording to the World Health Organization (WHO), anemia is a multifactorial pathological process in which the hemoglobin (Hb) concentration in the blood is below reference values. These values depend on the physiological need, which is individual and varies according to age, sex, gestational period, altitude (below, above, or at sea level), and lifestyle adopted by the patient, such as smoking.
1 For children aged six to 59 months, a Hb concentration <11g/dL characterizes an anemia framework.
1According to the WHO, the global prevalence of anemia among children aged six to 59 months averaged 39.8% in the year 2019.
2 In Brazil, there is a lack of studies with population-based samples to estimate the prevalence of childhood anemia. Systematic reviews such as that of Jordão
et al.
3 and Vieira
et al.,
4 indicate prevalence higher than 40%. In 2022, the report of the
Estudo Nacional de Alimentação e Nutrição Infantil (ENANI-2019) (National Study of Infant Food and Nutrition) showed a prevalence value of 18.9% in infants.
5 Thus, anemia is configured as a national and worldwide public health problem.
Iron deficiency anemia (IDA), identified as the leading cause of anemia in children worldwide, is a late manifestation of the body facing iron deficiency, which results in the depletion of iron reserves and, consequently, low Hb concentration.
1During pregnancy, the fetus accumulates iron coming from the mother's diet. Labor and postpartum periods are extremely delicate and therefore susceptible to complications if the care provided by the professionals involved is not adequate. Clamping the umbilical cord within one to three minutes after birth is a strategy recommended by the WHO for allowing the continuous passage of blood from the placenta to the newborn and improving iron storage, reducing iron deficiency after delivery.
6 Exclusive breastfeeding (EBF) for the first six months of life, as recommended by the WHO, the Brazilian Ministry of Health (MH), and the Brazilian Society of Pediatrics (BSP), is also a preventive strategy, since breast milk provides iron and other nutrients with high bioavailability.
1,7 Starting at six months of age, children should receive complementary feeding,
8 which should contain iron-source food such as red meat, dark green leafy vegetables, and beans, while avoiding high consumption of milk and dairy products near mealtime, as a way to help prevent iron deficiency.
8-10In the context of the COVID-19 pandemic, concerns about malnutrition are even more relevant. The United Nations estimates that in 2020, 9.9% of the population in the world suffered from malnutrition and 149 million children under the age of five presented a growth delay with negative perspectives in the years to come if actions are not taken.
11Early diagnosis of iron depletion is extremely important to prevent the evolution of the condition and to ensure success in the treatment. Observational studies show that anemia, when untreated, has significant consequences and can compromise the child's development. Cognitive and neuropsychomotor development are affected, since iron deficiency can lead to alterations in brain structure and function and can impair the metabolism of important hormones and the immune system.
1,12,13 In this scenario, childcare, which consists of continuous monitoring of children from birth to pre-adolescence (10 years of age), is extremely important.
14 Childcare practices include evaluation of the child's health condition (physical and laboratorial tests), and guidance to guardians on the importance of immunization and prevention programs.
15The
Programa Nacional de Suplementação de Ferro (PNSF), (National Program of Iron Supplementation), created in 2005, instituted the prophylactic supplementation with iron salts in children aged 6 to 24 months, pregnant women, premature infants, and women after delivery or abortion.
16 The use of oral iron supplements is recognized by the WHO,
1 and their effectiveness in increasing Hb levels has been demonstrated by several studies.
17,18 However, treatment to reverse the more severe consequences of anemia has not been effective,
17,18 and it is very important to prevent, diagnose, and treat IDA early. The BSP also recommends prophylactic iron supplementation from six months to 24 months; however, for children who present risk factors, supplementation should start at three months of life.
19This study aimed to evaluate the use of iron supplementation and associated factors in children aged six to 59 months attended at the Family Health Strategy (FHS) units in a city in Minas Gerais (MG).
MethodsThis was a cross-sectional analytical-exploratory study conducted between 2014 and 2016. Data were collected in ten FHS units located in Governador Valadares, in the State of Minas Gerais (MG), Brazil. It counted on a sample size of 252 children in the age group of six to 59 months, attended at FHS units that were selected by convenience according to their location in the city, in the urban territory. The sample size calculation was performed considering the number of children in the age group of interest registered at the FHS (1,064 children), the estimated frequency of anemia of 30%, 5% accuracy and 95% confidence interval, with 3% added in preventing losses. The research participants were contacted by means of an invitation carried by the community health agents to their homes and when they were attended at the health unit. The inclusion criterion was the child in the age group of interest and the exclusion criterion was previously diagnosed of diseases that prevented treatment with iron salt (hemoglobinopathies and hemochromatosis).
Data collection was performed using a structured questionnaire applied to the guardians, at the health unit, in a reserved room, where the child's anthropometry was also performed. The child's card and/or family records were also consulted when necessary.
The variables were collected in relation to the child's living and health status (categorical variables: sex; low birth weight; prematurity; complete blood count; breastfeeding; childcare; weight/age ratio; height/age and weight/age; continuous variables: age; birth weight; current weight; current height); the guidance given by the health professionals to the caregivers regarding anemia and preventive treatment (categorical variables: receipt of information about anemia; whether the child presents symptoms of anemia; dosage of the supplement; side effects); the family's socioeconomic conditions (continuous variables: mother's age; categorical variables: family income; maternal schooling) and about maternal health conditions during pregnancy (continuous variables: gestational age and categorical variable: number of prenatal visits).
A chart analysis was performed to collect hemogram results, and Hb levels below 11g/dL established the diagnostic criteria for anemia.
Descriptive statistics were performed, with absolute and relative frequency for categorical variables and calculation of means and standard deviation for continuous variables. The odds ratio (OR) was used as a measure of association between the occurrence of iron supplementation (response variable) and children's living and health conditions (explanatory variables), with the respective 95% confidence intervals (CI95%) estimated by the Mantel-Haenszel method. In the initial logistic model, variables with
p values ≤0.20 in the bivariate analyses were selected for multivariate analysis. In the final logistic model, the association level remained below 0.05. Data analysis was performed using Stata® version 14.0.
This study was approved by the Ethics Committee at the
Universidade Federal de Juiz de Fora (CAAE 29174814.3.0000.5147. Opinion number 715.272).
ResultsMost of the children were female (53.2%, n=134) and the median age was 28 months (two years and four months). Also, 45.6% (n=115) were in the six to 24 months age group while 54.4% were in the 25 to 59 month age group.
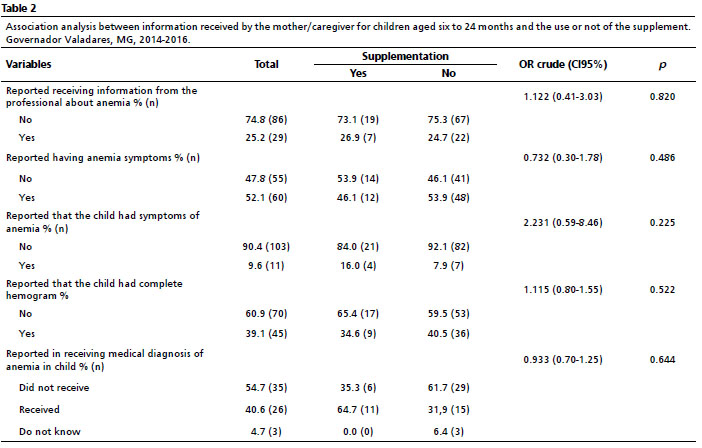
Tables 1 and 2 show the results obtained in the bivariate analysis for children aged six to 24 months, the target age group of the NPIS. In the final logistic regression model, no association obtained a significant
p value (
p≤0.05).
Of the 115 children in this age group, only 22.6% (n=26) were receiving supplementation at the time of the interview, and of those with anemia (n=18), only 22.2% (n=4) were supplemented at the time of the interview.
In relation to the group that was supplemented in the six to 24 month age group, 100.0% of the guardians (n=26) said they had received professional orientation regarding dosage and when they mentioned the dosage they used, 88.5% were correct; 15.4% of the guardians (n=4) said they had been oriented regarding possible side effects; 37.5% (n=9) observed improvement in the child and 30.8% (n=8) identified adverse effects, among them, diarrhea, cramps, stained teeth, nausea.
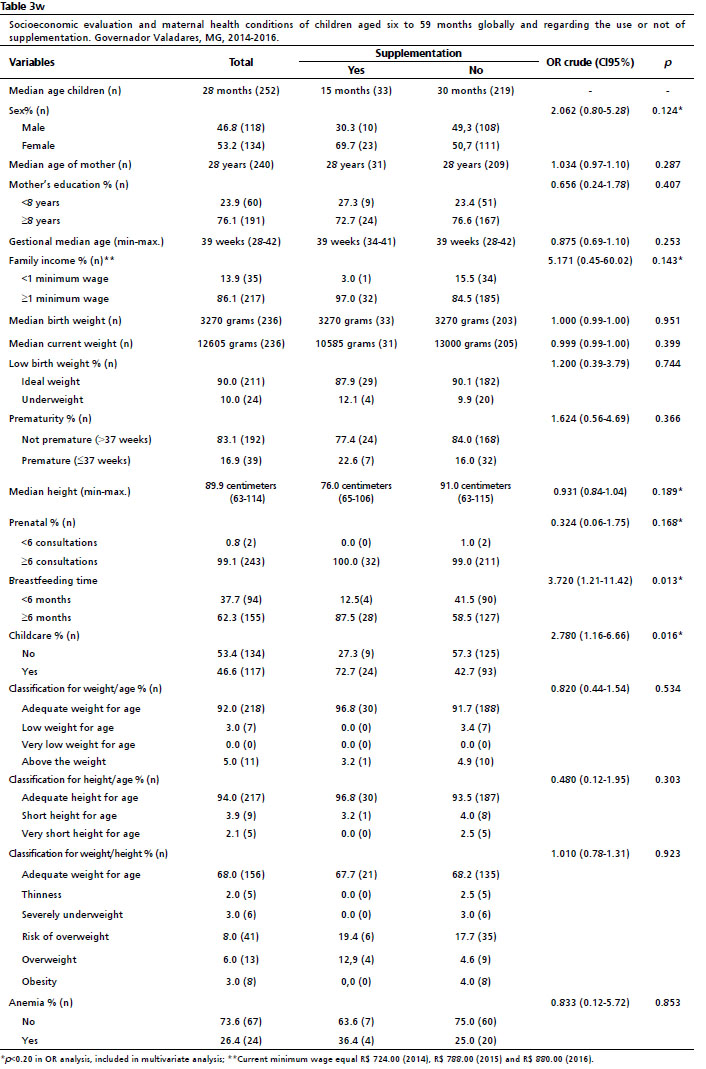
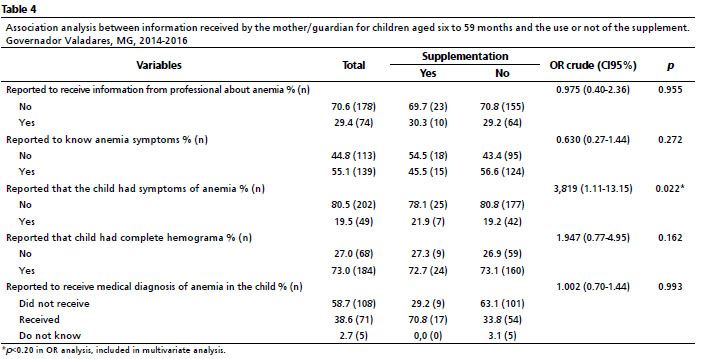
The same analyses were performed for the six to 59 month age group (n=252). Tables 3 and 4show the results obtained in the bivariate analysis for this population. Of the 252 children, 13.1% (n=33) were receiving the supplement at the time of the interview.
In the multivariate analysis only the variables breastfeeding time and childcare remained in the final logistic model, as shown in Table 5.
Regarding to the group that was supplemented in the age group of six to 59 months, 93.9% of the guardians said they had been oriented about the dosage and 81.2% reported a correct dosage; 18.2% of the guardians were oriented about the possible side effects; 45.2% observed improvement in the child and 30.3% perceived adverse effects, among them: diarrhea, cramps, stained teeth, nausea, and among others.
DiscussionFrom the data collected in this study, it was observed that 77.4% of children aged six to 24 months were not receiving iron supplementation, portraying a worrisome scenario, since the NPIS recommends that all children aged six to 24 months should receive it.
These lower-than-expected results corroborate national data on adherence to the NPIS. In 2018, the MH made a document available with results of coverage analysis on Ferrous Sulphate supplementation in 2017.
20 It was possible to observe that in the State of MG, Southeast region of the country, of the 407,146 children who should receive the supplement, only 2,564 received it, which corresponds to only 0.63% coverage of the program.
20 The Brazilian State that registered the highest coverage was Amapá, which reached 23.33% of the children aged six to 24 months, even so, it was still below the recommended coverage. Overall, Brazil had a goal of 4,441,081 children to be supplemented, but in 2017, according to registrations, only 2.69% (n = 119,378) received the proper supplementation, a significantly low number.
20 It is worth noting that these results were made available by each Brazilian State and some cities did not enter the data into the micronutrient system and consequently were not computed.
In the ENANI report, regarding the use of supplements containing iron, the survey results for a sample of 12,598 children under 5 years of age from all the regions of Brazil showed a prevalence of 21.7%. Regarding the use of supplements containing only iron, they found a prevalence of 14.6%. Interestingly, no significant difference was found between household situation, sex, color, and the child's race and the use of iron supplements.
5Other national studies have also evaluated the difficulties in implementing prevention programs. Marques
et al. 21 conducted a qualitative study with health professionals involved in the practice and observed a certain lack of information about IDA and the importance of prevention programs, as well as a lack of training and education of these professionals regarding health strategies.
21In the present study, the analysis of possible factors associated with the use or non-use of iron supplementation by children aged 6 to 59 months indicated a positive association between the use of the supplement with childcare follow-up and the duration of breastfeeding. Most supplemented children in this age group were active in childcare (72.7%) and were breastfed for six months or longer (87.5%).
As previously mentioned, the monitoring of children during childcare is extremely important to avoid complications in their development.
16 The result of the positive association between supplementation and participation in childcare, in other words, the performance of child health monitoring, corroborates the importance of this practice and of primary health care, indicating that strengthening the culture of childcare can collaborate with the implementation of prevention programs, ensuring greater chances of healthy development for children.
The importance of guidance, monitoring, and support from the health professionals was evidenced in Rodrigues
et al. study,
22 whose results showed an association between adherence to supplementation and the frequency of childcare. Furthermore, another study pointed out the necessity to seek new partners, such as daycare centers, since children meet 70.0% of their nutritional needs in these institutions.
23Still regarding to childcare and IDA prevention, it is necessary to pay attention to actions for the diagnosis of iron deficiency and IDA. Most of those responsible for the children included in this study reported that they had not had a complete hemogram (HG). According to the MH, screening for anemia through complete hemogram is recommended in situations where the child has not received adequate iron supplementation and for premature infants and those with short gestational age.
24 The BSP suggests that diagnostic tests for iron deficiency (complete hemogram, serum ferritin, and C-reactive protein) should be performed from 12 months of age onward, regardless of the child's condition.
8,19 However, most health professionals involved in childcare have difficulty identifying which tests should be performed and the ideal time to request them for asymptomatic children.
8,19The main national policies to prevent iron deficiency also encourage the use of iron supplements and EBF up to six months of age. The orientation and awareness of parents about the importance of breastfeeding is also an attribution of health professionals involved in child care.
25 As previously mentioned, breastfeeding is extremely important for the supply of micronutrients and macronutrients that are indispensable in the process of children's development and growth.
7 In this study, the positive association between the use of supplements and the length of breastfeeding may be due to guidance and awareness, actions of those responsible for taking the children for childcare monitoring, reinforcing the importance of these actions.
It is worth pointing out that the present study had limitations related to the type of research and data collection. Regarding the type of research, because it is a cross-sectional study (timeless), it is only possible to identify associations between exposure and outcome and not causality. In relation to data collection, it was about the difficulty of access to the children's guardians and the low number of hemogram results, even when schedules were made for the exam.
Thus, it was concluded that the supplementation was not occurring as recommended by prevention policies and that the factors of breastfeeding time and participation in childcare were associated with the use of the supplement, emphasizing the need to implement prevention programs, such as the
Programa Nacional de Suplementação de Ferro (National Program for Iron Supplementation) and training of professionals on the importance of health education for preventing infant anemia.
AcknowledgementsWe would like to thank all the students who participated in the projects related to the "
Programa de Prevenção da Anemia Infantil no município de Governador Valadares, MG" (PROANE) (Program for Prevention of Childhood Anemia) in the city of Governador Valadares, MG, between 2014 and 2017 and performed at some point the data collection: Carolina Filgueiras Torres, Iara A. Santos, Renan N. Gonçalves, Jéssica Aline Soares, Lais Xible Leite, Gustavo Estevam da Silva Gomes, and Daniel Vilas Novas Dornellas Caldeiras.
We also would like to thank the
Pró-Reitoria de Pesquisa e Pós-Graduação (PROPP) and
Pró-Reitoria de Extensão (PROEX-UFJF) of the
Universidade Federal de Juiz de Fora, MG, Brazil, the
Prefeitura Municipal de Governador Valadares, the
Secretaria Municipal de Saúde and the
Departamento de Atenção à Saúde for authorizing the execution of the projects that gave rise to the data presented in this work.
References1. World Health Organization (WHO). Nutritional anaemias: tools for effective prevention and control. Geneva: WHO; 2017. [access in 2022 ago 9]. Available from:
https://www.who.int/publications/i/item/97892415130672. World Health Organization (WHO). WHO Global Anaemia estimates, 2021 Edition. [access in 2022 ago 9]. Available from:
https://www.who.int/data/gho/data/themes/topics/anaemia_in_women_and_children3. Jordão RE, Bernardi JLD, Barros Filho ADA. Prevalência de anemia ferropriva no Brasil: uma revisão sistemática. Rev Paul Pediatr. 2009; 27 (1): 90-8.
4. Vieira RCDS, Ferreira HDS. Prevalência de anemia em crianças brasileiras, segundo diferentes cenários epidemiológicos. Rev Nutr. 2010; 23 (3): 433-44.
5. Universidade Federal do Rio De Janeiro (UERJ). Uso de suplementos de micronutrientes: caracterização do uso de suplementos de micronutrientes entre crianças brasileiras menores de 5 anos: ENANI 2019. Rio de Janeiro (RJ): UFRJ; 2022. [access in 2022 maio 25]. Available from:
https://enani.nutricao.ufrj.br/wp-content/uploads/2022/05/Relato%CC%81rio-6_ENANI-2019_Suplementac%CC%A7a%CC%83o-de-Micronutrientes-1.pdf6. Sociedade Brasileira de Pediatria e Federação Brasileira de Associações de Ginecologia e Obstetrícia. Diretriz: Recomendações sobre o clampeamento do cordão umbilical. Rio de Janeiro: SBP/FEBRASGO; 2022. [access in 2022 maio 25]. Available from:
https://www.sbp.com.br/fileadmin/user_upload/23396c-Diretrizes-Recom_Clamp_CordUmb.pdf7. Ministério de Saúde (BR). Secretaria de Atenção Primária à Saúde. Departamento de Promoção da Saúde. Guia alimentar para crianças brasileiras menores de 2 anos. Brasília (DF); 2019; [access in 2022 ago 9]. Available from:
http://189.28.128.100/dab/docs/portaldab/publicacoes/guia_da_crianca_2019.pdf8. Sociedade Brasileira de Pediatria (SBP). Departamento de Nutrologia e Hematologia. Consenso sobre anemia ferropriva: mais que uma doença, uma urgência médica! Rio de Janeiro: SBP; 2018. [access in 2021 dez 2]. Available from:
https://www.sbp.com.br/fileadmin/user_upload/21019f-Diretrizes_Consenso_sobre_anemia_ferropriva-ok.pdf9. Faria ACF, Pereira L, Silva P, Heitor R, Oiveira Jr WV, Domingueti CP. Avaliação da presença de anemia e de deficiência de ferritina em crianças. RBAC. 2017; 49 (4): 365-70.
10. Ferreira MCP, Pires PCC, Ribeiro RT, Silva CLAD. Frequência de consumo de alimentos fonte de ferro entre crianças de 6 a 59 meses atendidas pela Estratégia de Saúde da Família. HU Rev. 2019; 45 (4): 389-95.
11. FAO, IFAD, UNICEF, WFP and WHO. 2021. The State of Food Security and Nutrition in the World 2021. Transforming food systems for food security, improved nutrition and affordable healthy diets for all. Rome: FAO; 2021. [access in 2022 mai 25]. Available from:
https://www.fao.org/documents/card/en/c/cb4474en/12. Beard JL. Why iron deficiency is important in infant development. J Nutr. 2008; 138 (12): 2534-6.
13. Wachs TD, Georgieff M, Cusick S, Mcewen BS. Issues in the timing of integrated early interventions: contributions from nutrition, neuroscience, and psychological research. National Institutes of Health (NIH), Ann N Y Acad Sci. 2014; 1308: 89-106.
14. Brígido AF, Santos EOD, Prado EVD. Qualificação do cuidado a puericultura: uma intervenção em serviço na Estratégia de Saúde da Família. Rev Fund Care Online. 2019; 11: 448-58.
15. Del Ciampo LA, Ricco RG, Daneluzzi JC, Del Ciampo IRL, Ferraz IS, Almeida CAN. O Programa de Saúde da Família e a Puericultura. Ciên Saúde Colet. 2006; 11 (3): 739-43.
16. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Programa Nacional de Suplementação de Ferro: manual de condutas gerais. Brasília (DF): Ministério da Saúde; 2013. [access in 2021 dez 2]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/manual_suplementacao_ferro_condutas_gerais.pdf17. Larson LM, Phiri KS, Pasricha SR. Iron and cognitive development: what is the evidence? Ann of Nutr Metab. 2017; 71 (3): 25-38.
18. Sachdev H, Gera T, Nestel P. Effect of iron supplementation on mental and motor development in children: systematic review of randomised controlled trials. Public Health Nutr. 2005; 8 (2): 117-32.
19. Sociedade Brasileira de Pediatria (SBP). Departamento de Nutrologia e Hematologia. Consenso sobre anemia ferropriva: atualização: destaques 2021. Rio de Janeiro (RJ): SBP; 2021. [access in 2022 set 3]. Available from:
https://www.sbp.com.br/fileadmin/user_upload/23172c-Diretrizes-Consenso_sobre_Anemia_Ferropriva.pdf20. Ministério da Saúde (BR). Coordenação Geral de Alimentação e Nutrição. Ofício-Circular nº 14/2018/CGAN/DAB/SAS/MS. Divulgação dos resultados do Programa Nacional de Suplementação de Ferro em 2017. Brasília (DF); 2018. [access in 2021 dez 2]. Available from:
http://189.28.128.100/dab/docs/portaldab/documentos/NT_PNSF_2017.pdf21. Marques RM, Andrade Marques A, Serafim ALC, Cândido DB, Braga D, Almeida PT. Avaliação do Programa Nacional de Suplementação de Ferro. Rev Bras Promoç Saúde. 2019; 32: 1-8.
22. Rodrigues VB, Dallazen C, Vítolo MR. Impacto da atualização de profissionais de saúde em alimentação infantil na prevalência de anemia em crianças: Ensaio de Campo Randomizado. Rev Inova Saúde. 2017; 6 (1): 1-19.
23. Ferraz, ST. Anemia ferropriva na infância: estratégias para prevenção e tratamento. Pediatr Mod. 2012; 48 (3): 85-8.
24. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Saúde da criança: crescimento e desenvolvimento. Brasília (DF); 2012. [access in 2021 dez 2]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/saude_crianca_crescimento_desenvolvimento.pdf25. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Estratégia Nacional para Promoção do Aleitamento Materno e Alimentação Complementar Saudável no Sistema Único de Saúde. Manual de Implementação. Brasília (DF); 2015; [access in 2021 dez 2]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/estrategia_nacional_promocao_aleitamento_materno.pdfReceived on February 1, 2022
Final version presented on October 18, 2022
Approved on October 27, 2022
Associated Editor: Gabriela Sette
Authors' contribution: Ferreira ACRM: data analysis, discussion of results, and writing of the manuscript.
Ferreira MCP and Caetano GC: data collection and critical review of the manuscript.
Silva CLA and Ribeiro TR: project conception, study design, data collection and analysis, and writing the manuscript.
All authors approved the final version of the article and declare no conflict of interest.


 ; Mariany Cristine Peres Ferreira2
; Mariany Cristine Peres Ferreira2







 Ler em português
Ler em português