ABSTRACT
OBJECTIVE: to present the epidemiological profile of infant mortality and neonatal and post neonatal components, in addition to the temporal dynamics of these events in Pernambuco State between 2009 and 2018.
METHODS: descriptive, ecological, temporal space study of infant mortality in Pernambuco between 2009 and 2018. Epidemiological and temporal space characteristics were described using the Sistema de Informação sobre Mortalidade (Mortality Information System) and the Sistema de Informação sobre Nascidos vivos. (Information System on Live Births) as data sources.
RESULTS: there were 19,436 infant deaths in the period; 13,546 (69.7%) in the neonatal period and 5,890 (30.3%) in the post neonatal period. Male (55.4%), non-white children (74.7%) with low birth weight (63.5%) predominated; mothers were aged between 20 and 29 years (46.6%), with 8-11 years of schooling (43.9%) and preterm pregnancy (65.2%). Although the infant mortality rate decreased during the analyzed decade, high rates persisted in cities in the Sertão (backwoods) and Vale do São Francisco and Araripe macroregions of health services.
CONCLUSIONS: even though infant mortality declined over the years studied, it is necessary to achieve better rates and confront inequalities and other obstacles that perpetuate the event in Pernambuco State.
Keywords:
Infant mortality, Epidemiological surveillance, Vital statistics, Spatial analysis, Linear regression
RESUMO
OBJETIVOS: apresentar o perfil epidemiológico da mortalidade infantil e dos componentes neonatal e pós-neonatal, além da dinâmica espaço temporal desses eventos em Pernambuco, entre os anos de 2009 e 2018.
MÉTODOS: estudo descritivo e ecológico, de abordagem espaço temporal, da mortalidade infantil de Pernambuco entre 2009 e 2018. Foram descritas características epidemiológicas e espaço temporais, tendo como fonte de dados o Sistema de Informação sobre Mortalidade e o Sistema de Informação sobre Nascidos vivos.
RESULTADOS: ocorreram 19.436 óbitos infantis no período, sendo 13.546 (69,7%) no período neonatal e 5.890 (30,3%) no período pós neonatal. Predominaram crianças do sexo masculino (55,4%), não brancas (74,7%), com baixo peso ao nascer (63,5%), sendo as mães com idade entre 20 e 29 anos (46,6%), com escolaridade entre oito e 11 anos (43,9%) e com gestação pré-termo (65,2%). Houve decréscimo da taxa de mortalidade infantil durante a década analisada, entretanto elevadas taxas persistiram em municípios das Macrorregiões de saúde Sertão e Vale do São Francisco e Araripe.
CONCLUSÕES: a mortalidade infantil apresentou cenário de queda ao longo dos anos estudados, todavia é necessário o alcance de melhores taxas, o enfrentamento às desigualdades e a outros entraves que perpetuam o evento no estado de Pernambuco.
Palavras-chave:
Mortalidade infantil, Vigilância epidemiológica, Estatísticas vitais, Análise espacial, Regressão linear
IntroductionInfant mortality (IM) is considered a serious public health problem and is directly related to living conditions, access and quality of maternal and child healthcare, and is mostly preventable. In this sense, it is a strong indicator of access and quality of care provided to the maternal and child population.
1The children'sdeaths under one year of age are a consequence of biological, sociocultural, economic aspects, failures in the health system, and other social determinants of health. Therefore, actions to reduce this problem involve various society sectors as structural changes are required from the social sphere to the strengthening and qualification of maternal and child care actions, through the creation and implementation of public health policies.
2IM integrates two components, neonatal mortality and post-neonatal mortality, referring to deaths occurring in children under one year of age, between 0 and 27 days of life and between 28 and 364 days of life, respectively. In neonatal mortality, the causes of death are associated with the quality of healthcare, while in post-neonatal mortality there is a relationship with the environment in which the child grows and interacts. Even in environments with precarious contexts, there is evidence that better healthcare decreased infant mortality, further highlighting the importance of the mother's access to pregnancy planning, quality inprenatal care, assisted childbirth, and care until the first year of life to ensure survival, growth, and development.
3In Brazil, from 1990 to 2015, a decline in the infant mortality rate (IMR) was identified, going from 47.1 to 13.5 deaths/1,000 live births (LB), respectively.
4 When observed by regions, the highest rates were identified in the North (21 deaths/1,000 LB), followed by the Northeast (19 deaths/1,000 LB).
5 In 2016, PernambucoState showed an IMR of 13 deaths/1,000 LB.
6Although Brazil has achieved the reduction in infant mortality proposed by the 2015 agenda of the
Objetivos de Desenvolvimento do Milênio (ODM) (Millennium Development Goals), there are still challenges facing this public health problem, which demonstrates the need for commitment to achieve the
Objetivos de Desenvolvimento Sustentável (ODS) (Sustainable Development Goals), which presents a global agenda to be achieved by 2030, aiming to reduce neonatal mortality to at least 12/1,000 LB and mortality of children under five years of age to at least 25/1,000 LB.
7The association between infant mortality and territorial inequalities reinforces the need to analyze how this phenomenon is geographically distributed. In this sense, spatial analysis has been incorporated into epidemiological studies to reveal regions with higher risks for the occurrence of infant deaths.
8 The methods of this analysis in public health have been used mainly in ecological studies, through the detection of spatial or spatio-temporal clusters, evaluation and monitoring of this environment.
9The aim of this study is to present the epidemiological profile of infant mortality and the neonatal and post-neonatal components, as well as the spatial and temporal dynamics of these events in Pernambuco, between the years 2009 and 2018.
MethodsThis is a descriptive and ecological temporal space series study on infant mortality and its components. The study location, Pernambuco State, had in 2019 a population of 9,557,071 inhabitants
10 and of these, 133,359 were under one year of age.
11 The State is composed of 185 cities administratively distributed in twelve Health Managements Regionaggregated in the Metropolitan,
Agreste,
Sertão (Backwoods), and
Vale do São Francisco (Valley) and
Araripe Health Macroregions, according to Figure 1.
12 The study population corresponded to live births residing in Pernambuco in the period between January 1, 2009 to December 31, 2018. We used the databases of the
Sistema de Informação sobre Mortalidade (SIM) (Mortality Information System) and the
Sistema de Informações sobre Nascidos Vivos (Sinasc) (Live Births Information System) through the website of the
Departamento de Informática do Sistema Único de Saúde (DATASUS)(Department of Informatics of the Public Health System).
For the epidemiological profile and spatial analysis of two five-year periods were considered, the first consisting of the years 2009 to 2013 and the second consisting of the years 2014 to 2018.
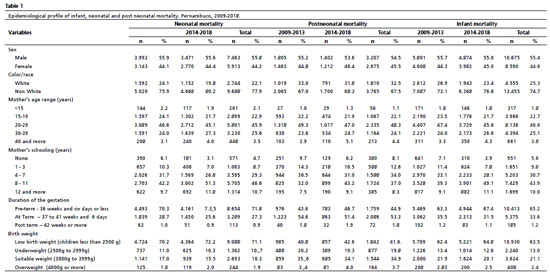
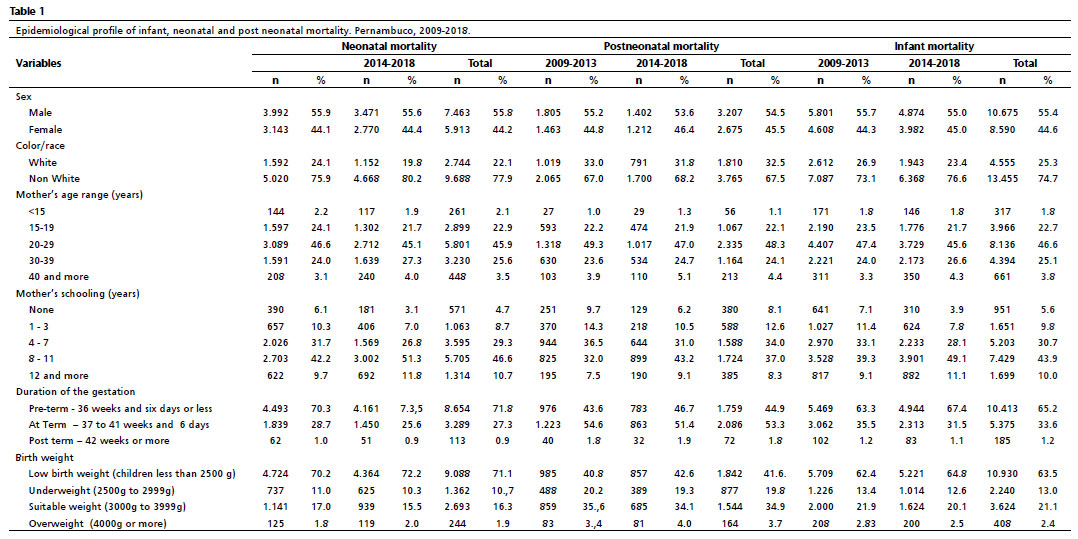
The epidemiological profile of infant, neonatal and post neonatal deaths was described by means of absolute and relative frequencies of the variables related to the child: sex (male/female), color/race (white/non-white), birth weight (low weight - less than 2500g; underweight - 2500g to 2999g; adequate weight - 3000g to 3999g or overweight 4000g or more) and, the variables concerning the mother of the child were age group (<15 years; 15-19 years; 20-29 years; 30-39 years; 40 and more), schooling (none; 1 to 3 years; 4 to 7 years; 8 to 11 years; 12 and more years of study) and gestation duration (preterm - 36 weeks and six days or less; full-term - 37 to 41 weeks and six days or post-term - 42 weeks or more).
For the time trend analysis, the neonatal, post-neonatal, and infant mortality rates were calculated for each year. Subsequently, linear regression was performed, with mortality rates as the dependent variable (Y) and the year of death as the independent variable (X).
For the spatial analysis, the crude infant, neonatal and post neonatal mortality rates were calculated for each city per five-year period.For this purpose, it was considered, for each five-year period, the total number of deaths (infant or neonatal or postneonatal) in the five-year period divided by the total number of live births in the five-year period multiplied by 1,000. Recognizing that crude mortality rates can be influenced by small population numbers or underreporting, smoothing of the rates by means of the local empirical Bayesian estimator was adopted in order to control for possible random fluctuations not associated with risk.
13Subsequently, the risk ratio (RR) was calculated, being the smoothed rate of the second five-year period divided by the smoothed rate of the first five-year period. If RR > 1.0 indicates an excess risk of infant mortality; if RR < 1.0 points to a reduction in infant mortality, while a RR=1.0 reports no change in the infant mortality scenario.
Spreadsheets and Epiinfo 7software, Terraview 4.2.2 and QGIS 2.18 were used. The cartographic base of Pernambuco State by cities of residence was made available on the website of the
Instituto Brasileiro de Geografia e Estatística (IBGE) (Brazilian Institute of Geography and Statistics). Due to the public nature of the data, it was not necessary to submit a research project to the Research Ethics Committee.
ResultsIn Pernambuco, 19,436 infant deaths occurred between 2009 and 2018, with 10,476 (53.9%) in the 1
st five-year period and 8,690 (46.1%) in the 2
nd five-year period, corresponding to an IMT of 14.9 and 12.9 deaths/1000 LB, respectively.
Of the total number of deaths, 13,546 (69.7%) were neonatal; of these, 7,203 (10.3 deaths/1000 LB) occurred in the first five-year period and 6,343 (9.1 deaths/1000 LB) in the second five-year period. The postnatal period accounted for 30.3% of all deaths (n=5,890), with 3,281 (4.7 deaths/1000LB) recorded in the first five-year period and 2,609 deaths (3.8 deaths/1000 LB) in the second five-year period.
The epidemiological profile of infant deaths had a similar pattern, whether in the neonatal or post-neonatal period, for the characteristics related to the child (predominance of male gender, non-white color/race and low birth weight) and the mother (age range of the mother between 20 and 29 years, schooling between eight and 11 years of study). Among the deaths in the neonatal period, preterm births were more common (Table 1).
The temporal trends of infant, neonatal, and postneonatal mortality rates presented themselves in a decreasing form in the analyzed period (Figure 2). The IMT was highest in the first year of the series (2009) with 17.1 and lowest in 2017 with 12.1. The neonatal IMT was the highest in 2009 (11.6) and reached 8.7 deaths/1000 LB in 2018. In a smaller magnitude, the post neonatal IMT started the series with 5.5 deaths/1000 LB in 2009 and reached the lowest level in 2017, with 3.5 deaths/1000 LB (Figure 2). Regarding the variability of the data, the linear model explains 76.5% of the variance of the infant mortality rate in relation to time, as well as the neonatal (68.7%) and post neonatal (75.6%) mortality rate (Figure 2).

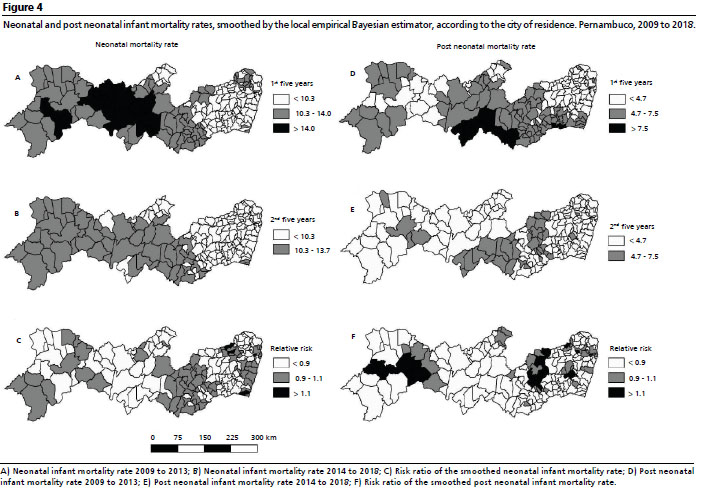
Although the temporal analysis revealed a decline in the IMT and its components, the spatial distribution reveals that the reduction of indicators takes place in a heterogeneous way in the Pernambuco territory (Figure 3 and 4). In the first five-year period, high IMT were observed, higher than the state average (14.9 deaths/1000 live births), especially in cities located in the Macroregions
Sertão (Backwoods) and
Vale do São Francisco and
Araripe (Figure 3A). In the second five-year period, we notice a reduction in the IMT, especially in the cities located in the
Sertão (Backwoods) of the State (Figure 3B), and this behavior is confirmed by the risk ratio (Figure 3C), which reveals the reduction or maintenance of the rates observed in the study period.
Similarly, the spatial pattern of neonatal IMT shows rates higher than the average observed in Pernambuco in the 1
st five-year period (10.3 deaths/ 1000 LB), tending to decrease when the period between 2014 and 2018 is observed (Figures 4A and 4B). However, the analysis of the risk ratio reveals a persistence of mortality, especially in cities concentrated in part of the
Agreste Macroregion, South of the Metropolitan Macroregion, and West of the
Vale do São Francisco and
Araripe Macroregion (Figure 4C).
Between 2009 and 2013, postneonatal infant mortality rates was higher than the average State (4.7 deaths/1000 LB) were concentrated in cities in the central region of the State (part of the Macroregions
Agreste and
Sertão (Backwoods) and in part of the Western Pernambuco (Macroregion of
Vale do São Francisco and
Araripe) (Figure 4D). Although a reduction in the number of cities with high rates was observed in the 2
nd five-year period (Figure 4E), the analysis of the risk ratio reveals the existence of cities in which rates increased - located in the Macro-region
Agreste and to the West of the State, in the Macroregions of
Vale do São Francisco and
Araripe (Figure 4F).
DiscussionThe present study identified that 19,436 infant deaths occurred in the period, 13,546 (69.7%) in the neonatal period and 5,890 (30.3%) in the post neonatal period. There was a predominance of male children (55.4%), non-white (74.7%), with low birth weight (63.5%), mothers aged between 20 and 29 years (46.6%), with schooling between 8 and 11 years (43.9%), and preterm pregnancy (65.2%). There was a decrease in IMT during the decade analyzed, however, high rates persisted in cities of the Macroregions of
Sertão and
Vale do São Francisco and
Araripe.
This behavior is aligned with the findings of the research of Souza
et al. ,
14 who investigated infant mortality in all Brazilian States between the years 1990 and 2015
14; throughout the 26 years analyzed, the reduction of IMT was perceived throughout the country, being more impactful in the States of the Northeast Region.
The literature recognizes as positive for improving this indicator. The improvement of living conditions, such as access to basic sanitation, food and nutritional security, and vaccination,
15 in addition to income transfer programs, such as the
Bolsa Família Program.
16 The strengthening of health policies, such as the expansion of the Family Health Strategy, the implementation of the
Política Nacional de Atenção Integral à Saúde da Criança (National Policy for Comprehensive Care of Child Health), and the creation of the
Rede Cegonha (Stork Network) a possible influence on coverage and care quality in the prenatal care, birth, and childbirth, and the form of care and management in women and children's health care.
16-18However, literature points out that after a long period of reduction of the IMT, an increase of 2.4% was identified in Brazil, corresponding to 12.7 deaths per 1000 LB in 2016. This behavior can be partially explained by the decrease in the number of LB in the period and the increase in postneonatal deaths. This period is related to the worsening of living conditions and access to health services,
19 the occurrence of the Zika virus epidemic in the years 2015 and 2016 with concomitant cases of Congenital Zika Virus Syndrome,
20 corroborating the results verified in the present study, which identified an increase in IMT and its neonatal and postneonatal components in 2016.
The predominance of infant deaths in male children, with low birth weight, premature, and children of young adult mothers as identified in the present study are characteristics found in other studies.
21-23 Low birth weight is related to the risk of malnutrition, infections, and respiratory problems in the first year of life.
22 As for the males, it may be related to the pulmonary maturation of the babies of this sex that occurs later, favoring the emergence of respiratory problems, which represents one of the main causes of death in this age group.
23In Pernambuco, the highest proportion of neonatal and postneonatal deaths occurred in children with young adult mothers (20 to 29 years) and with eight to 11 years of schooling. Since over the years a strong relationship has been identified between the occurrence of infant mortality and low maternal schooling
2,24 and extreme maternal age groups,
21,24 the findings of the present study need to be better investigated, with a more robust analytical approach, relating it to other factors such as access to health services, number of prenatal visits, occupation, and family income, among others.
As for the higher proportion of deaths in non-white children, similar results were found in most Brazilian State capitals.
2 Picoli
et al.
25 state that color or race alone would not be risk factors for the occurrence of infant death, but when they interact with other indicators of social position (schooling, income and sex), race or color can expose the group to situations of vulnerability, given their adverse social insertion.
The spatial analysis allowed us to identify the heterogeneous pattern of infant mortality in Pernambuco territory. High rates were concentrated in cities located in the Health Mesoregions of
Vale do São Francisco and
Araripe and in
Sertão (Backwoods), in regions more distant from the capital city of Recife. In Espírito Santo State, an investigation adopting spatial analysis on preventable infant mortality between 2006 and 2013 revealed spatial clusters in locations more distant from urban centers and with a greater lack of services. Such services - especially those of high complexity - in general located in greater concentration in the Metropolitan Regions of the States, indicate possible shortages in immediate specialized care for newborns, an essential component in the survival of children under one year of age.
26,27In the present study, the aggregates of high mortality rates may be related to population size, income, socioeconomic development, operation and locality of services. However, it is worth noting the reduction in infant mortality rates during the decade analyzed, identified by means of the risk ratio. The expansion of primary health care in the cities may have provided the reduction of access barriers, while its qualification may have increased its resolutivity and the articulation between interventions of surveillance and assistance.
28During the period, the strengthening of infant death surveillance committees in States and cities was also expanded and encouraged.
29 This instance has in its practice actions aimed at identifying the causes and factors that contribute to death, in addition to recognizing what has worked and what can be improved in relation to the care provided.
30 In this sense, the strengthening of infant death surveillance is essential to plan actions aimed at reducing infant mortality.
8Among the limitations of this study are the use of secondary data from
SIM and
SINASC, which may present inaccuracies, especially related to data quality. It is also noteworthy that smaller units of analysis, such as neighborhoods, would allow greater accuracy in the detection of priority regions for infant mortality. However, the use of cities is relevant due to the availability of these data in the information systems, in addition to the easy understanding and interpretation of this spatial level. To correct possible random fluctuations arising from the adopted analysis unit, the data were aggregated in five years concomitant with the application of rate smoothing estimator as a way to stabilize and minimize this effect.
The results show a scenario of decreasing infant mortality and its components, reflected in the temporal trend that may be a reflection of the strategies carried out over the years, indicating improvement in the quality of maternal and child care.
Studies with robust methodologies for temporal and spatial analysis are recommended at academic level and in health services, given the ability of
Sistemas de Informações Geográficas (Geographic Information Systems) to assist in understanding the context. Finally, identifying the profile of deaths and the spatial pattern of IM may contribute to the prioritization of interventions in healthcare and surveillance, especially in the most vulnerable territories.
References1. Rodrigues Martins PC, Jardim Cury Pontes ER, Higa LT. Convergência entre as Taxas de Mortalidade Infantil e os Índices de Desenvolvimento Humano no Brasil no período de 2000 a 2010. Interações (Campo Grande). 2018; 19 (2): 291-303.
2. Maia LTS, Souza WV, Mendes ACG. Determinantes individuais e contextuais associados à mortalidade infantil nas capitais brasileiras: uma abordagem multinível. Cad Saúde Pública. 2020; 36 (2): e00057519.
3. Santos EP, Ferrari RAP, Bertolozzi MR, Cardelli AAM, Godoy CB, Genovesi FF. Mortality among children under the age ofone: analysis of cases after discharge from maternity. Rev Esc Enferm USP. 2016; 50 (3): 390-8.
4. Leal MC, Szwarcwald CL, Almeida PVB, Aquino EML, Barreto ML, Barros F,
et al. Saúde reprodutiva, materna, neonatal e infantil nos 30 anos do Sistema Único de Saúde (SUS). Ciênc Saúde Colet. 2018; 23 (6): 1915-28.
5. Carvalho RAS, Santos VS, Melo CM, Gurgel RQ, Oliveira CCC. Inequalities in health: living conditions and infant mortality in Northeastern Brazil. Rev Saúde Pública. 2015; 49: 5.
6. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Análise em Saúde e Vigilância de Doenças não Transmissíveis. Saúde Brasil 2019: uma análise da situação de saúde com enfoque nas doenças imunopreveníveis e na imunização. Brasília (DF): Ministério da Saúde; 2019. [access in 2022 Aug 18] p. 369-404. Available from:
https://antigo.saude.gov.br/images/pdf/2019/dezembro/10/Apresenta----o-Expoepi-Sa--de-Brasil-Rodrigo-Said.pdf7. Marinho CSR, Flor TBM, Pinheiro JMF, Ferreira MÂF. Objetivos de Desenvolvimento do Milênio: impacto de ações assistenciais e mudanças socioeconômicas e sanitárias na mortalidade de crianças. Cad Saúde Pública. 2020; 36 (10): e00191219.
8. Bonfim CVD, Silva APSC, Oliveira CM, Vilela MBR, Freire NCF. Spatial analysis of inequalities in fetal and infant mortality due to avoidable causes. Rev Bras Enferm. 2020; 73 (Suppl. 4): e20190088.
9. Elliott P, Wartenberg D. Spatial Epidemiology: Current Approaches and Future Challenges. Environ Health Perspect. 2004; 112 (9): 998-1006.
10. Brasil. DATASUS TabNet Win32 3.0: População Residente - Estimativas para o TCU [Internet]. Pernambuco; 2021 [access in 2022 Aug 18]. Available from:
http://tabnet.datasus.gov.br/cgi/tabcgi.exe?ibge/cnv/poptpe.def11. Brasil. DATASUS TabNet Win32 3.0: Nascidos vivos [Internet]. Pernambuco; 2021 [access in 2022 Aug 18]. Available from:
http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sinasc/cnv/nvpe.def12. Pernambuco. Secretaria Estadual de Saúde. Plano Diretor de Regionalização [Internet]. [access in 2020 Jun 28]. Available from:
http://portal.saude.pe.gov.br/sites/portal.saude.pe.gov.br/files/pdrconass-versao_final1.doc_ao_conass_em_jan_2012.pdf.13. Martins Assunção R, Barreto SM, Guerra HL, Sakurai E. Mapas de taxas epidemiológicas: uma abordagem Bayesiana. Cad Saúde Pública. 1998; 14 (4): 713-23.
14. Souza MFM, Malta DC, França EB, Barreto ML. Transição da saúde e da doença no Brasil e nas Unidades Federadas durante os 30 anos do Sistema Único de Saúde. Ciênc Saúde Colet. 2018; 23 (6): 1737-50.
15. Barros de Medeiros VA, Dos Santos Bezerra IN, Monteiro FS, Mota LM. Perfil da mortalidade neonatal em Alagoas no período de 2008 a 2017. Rev Ciênc Plural. 2019; 5 (2): 16-31.
16. Silva ESA, Paes NA. Programa Bolsa Família e a redução da mortalidade infantil nos municípios do Semiárido brasileiro. Ciênc Saúde Colet. 2019; 24 (2): 623-30.
17. Ministério da Saúde (BR). Portaria nº. 1.130, de 5 de agosto de 2015. Institui a Política Nacional de Atenção Integral à Saúde da Criança (PNAISC) no âmbito do Sistema Único de Saúde (SUS). Brasília (DF): DOU de 5 ago 2015. [access in 2021 abr 3]. Available from:
http://bvsms.saude.gov.br/bvs/saudelegis/gm/2015/prt1130_05_08_2015.html»http://bvsms.saude.gov.br/bvs/saudelegis/gm/2015/prt1130_05_08_2015.html18. Gama SGN, Thomaz EBAF, Bittencourt SDA. Avanços e desafios da assistência ao parto e nascimento no SUS: o papel da Rede Cegonha. [Editorial] Ciênc Saúde Colet. 2021; 26 (3): 772.
19. Associação Brasileira de Saúde Coletiva (ABRASCO). Especial Abrasco sobre o aumento da mortalidade infantil e materna no Brasil. [
Internet]. 2018 [access in 2018 Ago 31]. Available from:
https://www.abrasco.org.br/site/outras-noticias/institucional/especial-abrasco-sobre-o-aumento-da-mortalidade-infantil-e-materna-no-brasil/36777/»https://www.abrasco.org.br/site/outras-noticias/institucional/especial-abrasco-sobre-o-aumento-da-mortalidade-infantil-e-materna-no-brasil/36777/.20. Nunes ML, Carlini CR, Marinowic D, Neto FK, Fiori HH, Scotta MC,
et al. Microcephaly and Zika virus: a clinical and epidemiological analysis of recurrent outbreak in Brazil. J Pediatr (Rio J. ). 2016; 92 (3): 230-40.
21. Oliveira MND, Camargo BA, Pinto Junior EP, Luz LA. Características dos óbitos infantis em um munícipio de médio porte da região Nordeste do Brasil. J Health Biol Sci. 2017; 5 (2):160-4.
22. Cutland CL, Lackritz EM, Mallett-Moore T, Bardají A, Chandrasekaran R, Lahariya C,
et al. Low Birthweight: Case definition & guidelines for data collection, analysis, and presentation of maternal immunization safety data. Vaccine. 2017; 35 (48): 6492-500.
23. Lourenço EC, Brunken GS, Luppi CG. Mortalidade infantil neonatal: estudo das causas evitáveis em Cuiabá, Mato Grosso, 2007. Epidemiol Serv Saúde. 2013; 22 (4): 697-706.
24. Fonseca SC, Flores PVG, Camargo Junior KR, Pinheiro RS, Coeli CM. Maternal educationand age: inequalities in neonatal death. Rev Saúde Pública. 2017; 51: 94.
25. Pícoli RP, Cazola LHDO, Nascimento DDG. Mortalidade infantil e classificação de sua evitabilidade por cor ou raça em Mato Grosso do Sul. Ciênc Saúde Colet. 2019; 24 (9): 3315-24.
26. Dias BAS, Santos-Neto ET, Andrade MAC, Zandonade E. Análise espacial dos óbitos infantis evitáveis no Espírito Santo, Brasil, 2006-2013*. Epidemiol Serv Saúde. 2019; 28 (3): e2018111.
27. Instituto de Geografia e Estatistica (IBGE). IBGE-Panorama-cidades-Recife. [access in 2021 nov 15]. Available from:
https://cidades.ibge.gov.br/brasil/pe/recife/panorama.28. Almeida PF, Fausto MCR, Giovanella L. Fortalecimento da atenção primária à saúde: estratégia para potencializar a coordenação dos cuidados. Rev Panamericana Salud Pública. 2011; 29 (2): 84-95.
29. Ministério da Saúde (BR). Portaria nº. 72, de 11 de janeiro de 2010. Estabelece que a vigilância do óbito infantil e fetal é obrigatória nos serviços de saúde (públicos e privados) que integram o Sistema Único de Saúde (SUS). Brasília (DF): DOU Janeiro; 2010. [access in 2022 set 7]. Available from:
https://bvsms.saude.gov.br/bvs/saudelegis/gm/2010/prt0072_11_01_2010.html30. Aminu M, Bar-Zeev S, van den Broek N. Cause of and factors associated with stillbirth: a systematic review of classification systems. Acta Obstet Gynecol Scand. 2017; 96 (5): 519-28.
Received on February 5, 2022
Final version presented on January 31, 2023
Approved on February 23, 2023
Associated Editor: Ana Albuquerque
Authors' contribution: Silva AV: conceptualization, data curation, analysis, research, methodology, project management, software use, final analyses and reviews.
Oliveira ECA: conceptualization, data curation, analysis, investigation, methodology, project management, software use, final analyses, reviews, supervision, validation, and co-guidance.
Silva AP: data curation, analysis, investigation, support, software use, final analysis support and reviews.
Silva APSC: conceptualization, data curation, analysis, investigation, methodology, project management, software use, final analyses, reviews, supervision, validation, and co-teaching.
The authors have approved the final version of the article and declare no conflict of interest.


 ; Emília Carolle Azevedo de Oliveira2
; Emília Carolle Azevedo de Oliveira2








 Ler em português
Ler em português