ABSTRACT
OBJECTIVES: to analyze differences between violence against children and adolescents according to characteristics of cases, probable perpetrators, occurrences and typologies and compare their temporal and spatial distributions.
METHODS: data were collected from the Notifiable Diseases Information System (SINAN), Maranhão, from 2009-2019.
RESULTS: 4,457 notifications of violence against children and 5,826 against adolescents were analyzed. In the 11 years investigated, violence against children was more frequent in 2015 and 2016 and in five of the 19 Maranhão Health Regions. Violence against males was more frequent in childhood and against females prevailed mostly in adolescence (p<0.001). While mothers (p<0.001), fathers (p=0.029) and caregivers (p<0.001) were most frequently accused of violence against children, friends/acquaintances (p<0.001), spouses/boyfriends/girlfriends (p<0.001) and strangers (p<0.001) mainly assaulted adolescents. Violence motivated by sexism (p=0.006), generational conflict (p<0.001), street situation (p=0.002) and disability (p=0.035) were more frequent in adolescence. Physical (p<0.001), sexual (p<0.001) and psychological/moral (p<0.001) violence, torture (p<0.001) and self-aggression (p<0.001) were most commonly reported in adolescence and neglect/abandonment predominated was mostly reported against children (p<0.001).
CONCLUSIONS: violence against children and adolescents residing in the state of Maranhão and notified in SINAN were distinct phenomena in relation to the characteristics of cases, probable authors, occurrences, and typologies.
Keywords:
Adolescent, External causes, Child, Notification, Violence
RESUMO
OBJETIVOS: analisar diferenças entre violências praticadas contra crianças e adolescentes segundo características de casos, prováveis autores, ocorrências e tipologias e comparar suas distribuições temporais e espaciais.
MÉTODOS: os dados foram coletados do Sistema de Informação de Agravos de Notificação (SINAN), Maranhão, de 2009-2019.
RESULTADOS: foram analisadas 4.457 notificações de violências contra crianças e 5.826 contra adolescentes. Nos 11 anos investigados, violências contra crianças predominaram em 2015 e 2016 e em cinco de 19 Regiões de Saúde maranhenses. Violências contra casos do sexo masculino foram mais frequentes na infância e contra pessoas do sexo feminino prevaleceram na adolescência (p<0,001). Enquanto mães (p<0,001), pais (p=0,029) e cuidadores (p<0,001) foram mais acusados de violência contra crianças, amigos/conhecidos (p<0,001), cônjuges/namorados(as) (p<0,001) e desconhecidos (p<0,001) teriam agredido principalmente adolescentes. Violências motivadas por sexismo (p=0,006), conflito geracional (p<0,001), situação de rua (p=0,002) e deficiência (p=0,035) foram mais frequentes na adolescência. Violências física (p<0,001), sexual (p<0,001) e psicológica/moral (p<0,001), tortura (p<0,001) e autoagressões (p<0,001) foram mais notificadas na adolescência e negligência/abandono predominou contra crianças (p<0,001).
CONCLUSÕES: violências contra crianças e adolescentes estudadas se mostraram como fenômenos distintos em relação a características de casos, prováveis autores, ocorrências e tipologias sugerindo a necessidade de considerar suas especificidades nos planejamentos e avaliações de programas e projetos de enfrentamentos.
Palavras-chave:
Adolescente, Causas externas, Criança, Notificação, Violência
IntroductionAll violence committed against children and adolescents should be considered a violation of human rights, a public health problem and a preventable event. Children and adolescents from every nations should have their rights granted and be protected from any type of physical, emotional and sexual violence, as well as neglect and exploitation or any relation of power that could generate harm in their development, dignity and health.
1With the Convention on the Rights of the Child, signed in 1989, a broad articulation of the States party of the United Nations occurred in order to make children and adolescents subjects to rights and to combat violence performed against them.
1-4 In Brazil, this international mark substantiated the foundation of the Statute of the Child and Adolescent (ECA - Portuguese acronym) in the integral protection of people aged until 17 years.
3-5 In the Article 13, the ECA determinates that suspected or confirmed cases of physical punishment, cruel or degrading treatment and mistreatment against children and adolescents should be mandatorily informed to the Tutelary Council.
4In 2001, the National Policy of Reduction of Morbimortality by Accidents and Violence brought attention to the need for structuring systems of violence surveillance in Brazil, attempting to bring more visibility and to improve the confrontation against this health risk.
5 As a consequence of this Public Policy, the Ministry of Health created the System of Surveillance of Violence and Accidents (VIVA - Portuguese acronym), in 2006; included violence in the list of compulsory notification of the Notification Aggravation Information System (SINAN - Portuguese acronym), in 2009; and determined, in 2011, that suspect or confirmed cases of domestic and sexual violence, as well as other types of violence, assisted in health and educational systems should be compulsorily notified.
6These and other legal rules and the growing increase of VIVA/SINAN coverage in Brazilian Federative Units improved substantially violence notification in Brazil, from 2011.
6,7 Despite of these improvements, recent epidemiological surveys with data from this System evidenced that interpersonal
8-15 and self-inflicted
16,17 violence against children and adolescents were underreported.
Studies with data from SINAN frequently do not compare temporal trends of interpersonal and/or self-inflicted violence in these two life stages,
9-11,13,15-17,20-23, do not investigate the motivation of interpersonal violence
9-11,13-15,18-23 and do not measure statistical difference between types of violence perpetrated against children and adolescents
9,10,12,14,16,18-23, which justifies this study. Moreover, in the State of Maranhão, the epidemiological knowledge on this subject is restricted to a few descriptive studies that do not allow the recognition of specifities of interpersonal and self-inflicted violence reported in childhood and adolescence.
21-23Based on these considerations, the following hypothesis was developed: there are characteristics that distinguish types of violence perpetrated against children and adolescents, and it is not recommended to analyze these phenomena as a totality. In this perspective, this study compared temporal and spatial distributions of violence perpetrated against children and adolescents residing in the state of Maranhão and reported at SINAN, and analyzed differences between characteristics of cases, probable authors, occurrences and typologies in these two stages of life.
MethodsA temporal and spatial study of suspect and confirmed cases of violence perpetrated against children and adolescents residing in the state of Maranhão (Brazil) and reported in the SINAN in the period from January 1, 2009 to December 31, 2019.
2009 was defined as the temporal onset of the survey because in this year, the individual Sheet of notification/surveillance - domestic, sexual and other types of interpersonal violence were integrated to SINAN.
6 Since the databases of interpersonal/self-inflicted violence in 2020 and 2021 were not available in Information System Department of Unified Health System (DATASUS) in October, 2021, when the analyses of this study were concluded, the temporal limit was set in 2019.
24In agreement with SINAN definitions, it was considered as child a person in the age range of 0-9 years and as adolescent the individual aged 10-19 years old.
6The state of Maranhão, located in the Northeast Region of Brazil, had a population estimated in 6,367,111 inhabitants in 2009 (21.9% with 0-9 years and 20.7% with 10-19 years) and a projected population of 7,083,578 inhabitants in 2019 (18.3% with 0-9 years and 19.8% with 10-19 years).
25With the Tab for Win software (TABWIN), data from Maranhão were exported to the TABNET application and scheduled in a Microsoft Office Excel (version 2019) spreadsheet.
Data from the SINAN's violence Sheet classified as key field (that identifies system registry) selected for this study were date and municipality of notification. Among the fields of mandatory fulfillment (the absence of data precludes the inclusion of the notification in SINAN), were analyzed: date of occurrence of violence case, date of birth, age and gender of the person assisted, municipality of occurrence, gender and life cycle of the possible author of violence, link/degree of kinship of the probable author with the person assisted, place of occurrence, motivation and type of violence. The essential fulfillment fields (necessary to the surveillance of the case or for calculating epidemiological or operational indicators) studied were race/color of the person assisted, whether the individual possessed any type of deficiency/disorder, if the injury occurred in another occasions and whether the violence was self-inflicted.
6The analysis of consistency of fulfillment of the age field of the person assisted was executed. When the answer to this field was ignored, it was fulfilled with the difference between the dates of occurrence of violence and birth, if they were compatible.
6Interpersonal violence was defined by SINAN as any intentional behavior of force, power or omission that could generate or result in harm to another individual. Self-inflicted violence occurs when there is self-aggressions, suicide ideation, suicide attempts and suicides.
6Temporal analyses were performed separating interpersonal and self-inflicted violence. In spatial distribution, the 19 Health Regions of the state of Maranhão were used as analysis unit, categorized as follows: Açailândia, Bacabal, Balsas, Barra do Corda, Caxias, Chapadinha, Codó, Imperatriz, Itapecuru-Mirim, Pedreiras, Pinheiro, Presidente Dutra, Rosário, Santa Inês, São João dos Patos, São Luís, Timon, Viana, Zé Doca.
25In the analyses of interpersonal violence, all cases of self-inflicted violence were excluded. The variables that assessed characteristics of the people assisted (or cases) were age (0-9 years and 10-19 years), gender (male and female), race/color (white, brown, yellow, black and indigenous) and deficiency/ mental disorder (yes and no). Race/color was collected in a self-declared manner or with the professional responsible for the case, when the person assisted was a child.
6In regard to the probable author of interpersonal violence, the studied variables were sex (male, female, both and ignored), life cycle (0-9 years, 10-19 years, 20=59 years or young/adult and 60 years or more or elderly) and link/kinship degree with the case (father, mother, mother and father-in-law, current or former spouse/boyfriend/girlfriend, brother/sister, friends/acquaintances, unknown people, caregiver and others).
Characteristics of the occurrence of interpersonal violence were assessed with the variables place of occurrence (residence, collective inhabitation, school/crèche and public locations) and motivation for violence (sexism or violence against women, homophobia/lesbophobia/biphobia/transphobia, racism/xenophobia/religious intolerance, generational conflict, street situations, deficiency and others). The field motivation for violence was included in SINAN sheet only in the year 2015.
6In SINAN, the category "residence" includes the place where the assisted person resides and the residences of friends, relatives, neighbors, spouses, girlfriends/boyfriends and probable author of the aggression. Collective inhabitation is a term that encompasses places such as military camp, workers camp, nursing home for elderly, student's dormitories, barracks, psychiatric hospital (when used as residence by the assisted person), shelters, penitentiary, colony hospitals, boarding house, socio-educational unit, host unit and hostel.
6The types of studied interpersonal violence were physical violence, psychological/moral/sexual violence, neglect/abandon, torture, human trafficking, child labor, financial/economic violence and violence in legal intervention, all dichotomized in yes and no. Recurrent interpersonal violence and self-inflicted violence also were categorized as yes and no.
In SINAN, physical violence is defined as the intentional use of physical force with the attempt to inflict damage to others. Moral/psychological violence is every action that might harm identity, self-esteem or the development of another person. Sexual violence means to force someone to participate or witness sexual interactions. Neglect/abandon is not providing the assisted person with basic needs and care for their physical, emotional and social development. Torture means to embarrass someone by physical force or threats in order to obtain information or confessions or by means of discrimination, such as the racial one. Human trafficking is defined as the movement of people by coercion or by means of mislead in an attempt to exploit. Child labor is any kind of activity performed by children and adolescents in an enforceable, regular, uneventful manner, paid or not, that endangers their well-being and limits their growth and development. Financial/economical violence is defined as loss, damage or destruction of something that belongs to the assisted person. Violence by legal intervention is that committed by a public agent in the exercise of his/her function.
6The descriptive (frequency and percentage) and statistical analyses were performed with Stata
® 15.0 software. The temporal analyses were made by year surveyed, and the spatial analyses gathered eleven years because there were regions without notification of cases in the first years of SINAN implementation. It was considered that there were differences of violence performed against children and adolescents when the Pearson's chi-square test or Fisher's exact test had
p-value <0.05. When the variables were polychotomous, the p value with Fisher's exact test was calculated for each category.
Since this is a survey with secondary public data, the approval of the research project by the Research and Ethics Committee was not necessary, according to the ethical guidelines of resolution number 510/2016 of National Health Council.
ResultsAfter verification and correction of errors in answers to the field "age of assisted person" (21 children and two adolescents), 10,283 cases of violence were accounted for against people aged 0-19 years, being 4,457 (43.3%) against children and 5,826 (56.7%) against adolescents. Most notifications were of interpersonal violence cases (n=9,162). 1,121 cases of self-inflicted violence (11.9%) were registered.
Notifications of interpersonal violence against children were more frequent in 2015 and 2016 and interpersonal violence against adolescents predominated from 2009 to 2014 and 2017 to 2019 (Figure 1).
In all of the surveyed years, there were more notifications of self-inflicted violence in adolescence. From 2010 to 2014, no cases of self-aggressions in children were registered, as they appeared in 2015 and increased in 2016, decreasing in 2018 and 2019. The number of self-lesions in adolescents increased from 2009 to 2012, remaining stable until 2015, decreasing in 2016, increasing in 2017 and increasing expressively in 2018 and 2019 (Figure1).
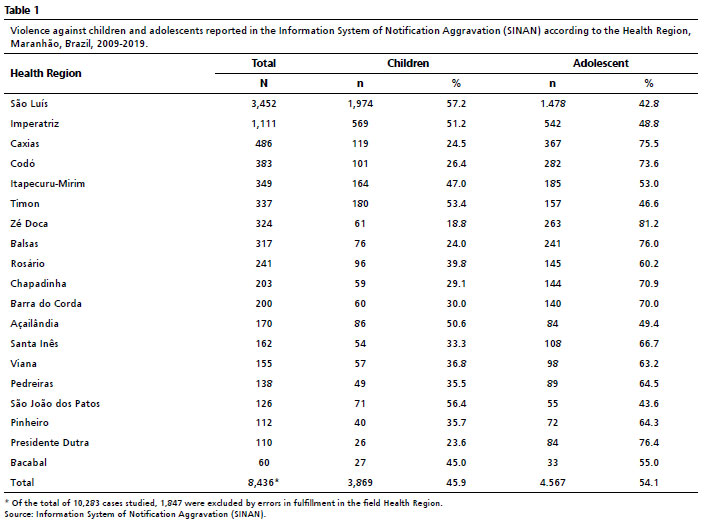
Violence against children were more frequent in five of the 19 Health Regions of Maranhão: São Luiz, Imperatriz, Timon, Açailândia and São João dos Patos. In the other 14 Regions, violence against adolescent predominated, with higher percentages in Zé Doca, Presidente Dutra, Balsas, Caxias and Codó (Table 1).
Interpersonal violence against people of male gender (
p<0.001), brown (
p<0.001) and indigenous (
p=0.005) predominated in childhood. Aggressions against people of female gender (
p<0.001), white (
p<0.001), black (
p<0.001), yellow (
p<0.004) and with deficiencies (
p<0.002) were more notified in adolescence. Self-inflicted violence was performed mostly by adolescents of female gender (
p<0.001) (Table 2).
Probable authors of female gender would have practiced more interpersonal violence against children (
p<0.001). When there were two or more probable authors of different genders, the aggressions also predominated against children (
p<0.001). In adolescence, probable authors were mostly people from male gender (
p<0.001) (Table 2).
Concerning the link between the probable author and the assisted person, mothers (
p<0.001), fathers (
p<0.0029) and caregivers (
p<0.001) would have performed more frequently violence against children. Friends/acquaintances (
p<0.001) former/current spouse/boyfriend (girlfriend) (
p<0.001) and unknown people (
p<0.001) were more accused of violence against adolescents. Children (
p<0.001) and elderly (
p<0.001) would have attacked mainly children and adolescents (
p<0.001) and adult people (
p=0.002) were the main probable authors of violence against adolescents (Table 2).
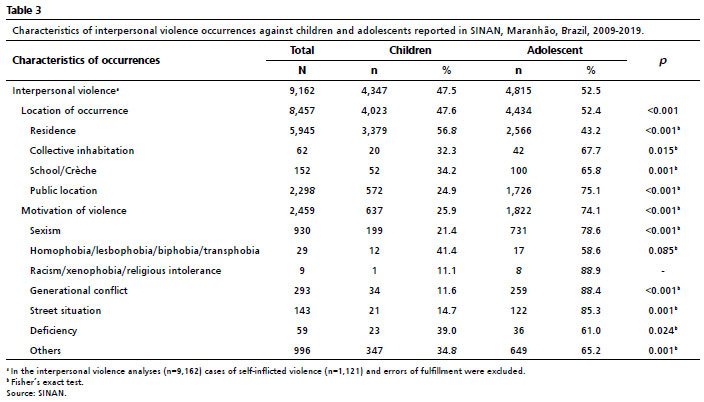
Whilst interpersonal violence against children occurred more frequently in residences (
p<0.001), public locations (
p<0.001), schools/crèches (
p=0.001) and collective inhabitations (
p=0.015) were the places in which violence against adolescents predominated (Table 3).
Violence motivated by sexism (
p<0.001), generational conflict (
p<0.001), street situation (
p<0.001), deficiencies (
p=0.024) were more reported in adolescence (Table 3).
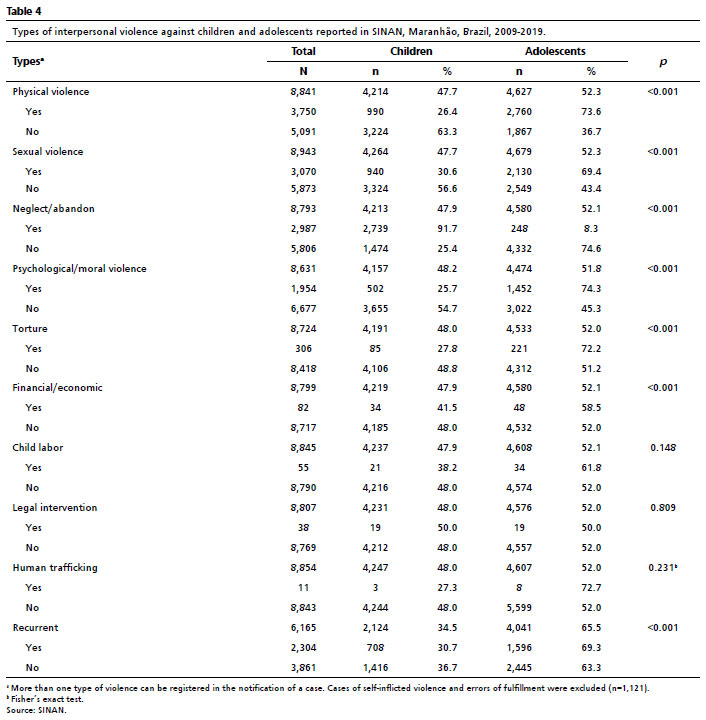
Interpersonal violence of physical, sexual, psychological/moral and torture types were more frequent against adolescents (
p<0.001). Neglect/abandon was the only type of violence more frequent in childhood (
p<0.001) (Table 4), having occurred mainly in 2015 and 2016 and in the five regions in which violence against children predominated. A mother was referred to as probable author of this kind of violence in approximately 90% of cases (result not presented in table).
Recurring violence also occurred more between adolescents (
p<0.001) (Table 4). Recurrence of episodes was more frequent in female gender (n=1,807) than in male gender (n=497), with higher percentages in sexual violence (45%) and physical violence (44.6%) (results not presented in tables).
DiscussionThe findings of this study demonstrated that interpersonal violence against children predominated in the years 2015 and 2016 and interpersonal violence against adolescents occurred more frequently from 2009 to 2014 and 2017 to 2019; there were annual expressive increases in notifications of self-inflicted violence from 2017, mainly within the female gender; violence against children prevailed in five of nineteen Regions of Health from Maranhão; and a group of characteristics of the attended cases, probable authors, occurrences and types distinguished violence perpetrated against children and adolescents.
Increases in the number of notifications of violence against children and adolescents in the state of Maranhão occurred simultaneously to the expansion of VIVA/SINAN coverage in the state, similarly to what was observed in Brazil, in the period from 2009 to 2017.
10 In 2011, only 19.8% of municipalities of Maranhão reported cases of violence assisted by SUS, against 85.7% in the year 2018.
7The predominance of notifications of interpersonal violence against adolescents may be explained due to the fact of the main authors were, more frequently, friends/acquaintances, former/current spouse/boyfriend (girlfriend), unknown people and other non-relative aggressors, which may have facilitated the unveiling of violence.
1 Another possible justification for this finding is that the two types of violence that were more practiced against them, physical and sexual, are easier to identify by health professionals.
26 Furthermore, adolescents commonly challenge established rules and involve themselves in conflicts that may result in violence.
3 Nevertheless, it is worth not ignoring that the notified episodes in adolescence may have started in childhood and stood hidden for years.
1,3Higher percentages of violence against children in 2015 and 2016 may be the reflection of national and state conjunctures. The reported cases in these two years were mainly of neglect/abandonment of children of male gender, being the mother the probable author. In Brazil, the years 2015 and 2016 were highlighted by a great economic recession, with drops in GDP and number of jobs (mainly formal jobs), increase in family debt and decrease in family consumption. In 2016, Maranhão had 52.4% of people residing in particular permanent residences with family per capita income under 5.5 dollars per day, a poverty indicator according to the World Bank. In this biennium, Maranhão was the second worst Brazilian state in regard to percentage of workers in formal jobs.
27 In this perspective, it is possible that the predominance of notifications of neglect/abandon of children residing in the state of Maranhão, in 2015 and 2016, was the consequence of the increase of families in situation of poverty in the state.
28In regard to self-inflicted violence, it prevailed in adolescents, mainly of the female gender, and had an exacerbated increase in 2018 and 2019. Characteristics of the adolescence, for example the search for identity, a trend of organization in groups and getting apart from the family, conflicting relationships, impulsiveness, constant humor variations, use of illicit and licit drugs and higher autonomy for the use of damaging social media lead the adolescent to soothe their suffering with self-injuries.
16,17It is possible that the increase of notifications of self-inflicted violence, observed from 2015, is consequence of the expansion of notification units in the state, which reached approximately 86% of Maranhão municipalities, in 2018
6 and the awareness of health professionals to identify and report self-aggressions.
16In Brazil as a whole and in the state of Rio Grande do Sul, self-inflicted violence were mostly performed by adolescents of female gender.
16,17 In Rio Grande do Sul, self-aggressions increased at the same time of the increase of sexual violence, notably from 2016.
16The five Regions of Health were predominated violence against children encompasses the six most populous municipalities of Maranhão. In these regions, neglect/abandon was the most registered type of violence, which may explain this finding. Another two studies conducted in municipalities of the states of Rio de Janeiro and Paraná also found spatial differences between violence against children and adolescents.
18,19Violence against children occurred more frequently in residences and would have been practiced mainly by mothers, fathers and caregivers, which characterizes the episodes, mostly, as manifestations of familiar/domestic violence.
10,12,14,15,20 In brazil, from 2009 to 2017, the residence was the place where violence against children were more practiced, with higher percentages in the age range of five to nine years (66.7%). Mothers and fathers were pointed as the main probable authors of this aggression.
10Neglect/abandon was the only type of violence that was more frequent against children residing in Maranhão. Between indigenous children, this kind of violence reached a percentage of 51.4%, being the most reported type. For any motivation of neglect/abandon, it is important that children in social vulnerability situation are identified and conducted to the Tutelary Council for the proper protection.
4 In the state of Rio de Janeiro, neglect/abandon predominated within children, in the year 2018.
20Interpersonal violence against brown children and adolescents prevailed in relation to other races/skin colors. Justifying this finding, the National Survey for Continuous Residence Sample 2019 demonstrated that 68.5%, 17.9% and 12.8% of the population residing in Maranhão are self-declared brown, white and black, respectively.
29 It is possible that the predominance of violence in brown children found in this study may be related to the type of aggression: neglect/abandon, for example, occurred in eighteen brown children and only one brown adolescent. Differences in races/skin colors have been found in several studies, depending on the type of violence, gender and age ranges of cases and region of occurrence.
10,12,13,14In agreement with other studies,
14,19 interpersonal violence against people with deficiencies/disorders occurred more frequently in adolescence than in childhood. Adolescents with deficiency/disorder were mainly of the female gender and were victims of sexual violence, mostly, unlike what is observed in Brazil, in the year 2018.
19 In regard to the condition that provoked aggression, violence motivated by deficiency was the most observed among adolescents. Children with deficiencies/disorders were victims mainly of neglect/abandon, similar to what was found in Brazil, in the year 2018.
19Whilst probable authors of female gender would have committed violence mainly against children (mostly neglect/abandon cases), probable authors of male gender were more mentioned as perpetrators of violence against adolescents, mainly sexual, physical, psychological/moral violence and torture. These findings may be explained by unequal relations of power between genders and generations.
3 In the city of Manaus, people from male gender practiced approximately 57% and 80% of aggressions against children and adolescents, respectively.
14Sexism or violence against women was almost four times more frequent in adolescence. Violence against women is based on unequal power relations between genders, with supremacy of the male over the female.
1,3 Predominated also in adolescence the motivations "generational conflict" and "street situation", which can be consequences of unequal power relations between generations and social classes.
3Recurrent violence was more reported in adolescence than in childhood, with more victims of the female gender, a result that can be explained due to the fact that most recurrent types were the physical and sexual ones, which prevailed more in adolescents of this gender. Nevertheless, it is known that these episodes are frequently initiated in childhood and remain hidden for years. This happens because small children cannot report what have occurred, are threaten by their aggressors and hide the experienced violence, are not protected by their families and the episodes are not perceived by health professionals that are responsible for compulsory notification.
1 In the state of Espírito Santo, recurrent violence against children occurred mainly in the age range of six to nine years in female gender.
30The limitations of this study are related to underreport of interpersonal and self-inflicted violence and errors of fulfillment of fields in the Violence Sheet of SINAN. Underreports occurred mainly in 2009 and 2010, when there wasn't the obligation of health professionals to notify compulsorily domestic and other types of violence.
6 It is possible that other cases of violence against children and adolescent had not been reported because health professionals has difficulties in recognizing signs of violence that are not evident and due to the false concern of breaking professional secrecy.
7,26 Nevertheless, notification (and not denounce) are part of a dimension of care for Integrative Healthcare for children, adolescents and their families in situation of violence.
6The results of this study indicated differences in temporal and spatial distributions of violence performed against children and adolescents. Interpersonal violence against children and adolescents came to be distinct phenomena according to characteristics of cases, probable authors, occurrences and types, suggesting the need for considering their specifities in the planning and evaluation of programs and projects of combat.
References1. Pinheiro PSMS. World report on violence against children. Geneva: United Nations; 2006. [acesso em 2021 set 24]. Disponível em:
https://digitallibrary.un.org/record/5873342. United Nations. Convention on the Rights of the Child. New York; 1989. [Internet]. [access in 2021 set 24]. Available from:
https://www.unicef.org/child-rights-convention3. Ministério dos Direitos Humanos (BR). Secretaria Nacional de Proteção dos Direitos da Criança e do Adolescente. Violência contra crianças e adolescentes: análises de cenários e propostas de Políticas Públicas. Brasília (DF): Ministério dos Direitos Humanos; 2018. [access in 2021 set 24]. Available from:
https://www.gov.br/mdh/pt-br/centrais-de-conteudo/consultorias/conada/violencia-contra-criancas-e-adolescentes-analise-de-cenarios-e-propostas-de-politicas-publicas.pdf4. Brasil. Presidência da República. Lei nº 8.069, 13 de julho de 1990. Dispõe sobre o Estatuto da Criança e do Adolescente e dá outras providências. [access in 24 set 2021]. Available from:
http://www.planalto.gov.br/ccivil_03/leis/l8069.htm5. Ministério da Saúde (BR). Portaria n. º 737, de 16 maio de 2001. Política Nacional de Redução da Morbimortalidade por Acidentes e Violências. Brasília (DF): DOU de 18 maio de 2001; Seção 1, v.96, p.1-62. [access in 24 set 2021]. Available from:
https://bvsms.saude.gov.br/bvs/saudelegis/gm/2001/prt0737_16_05_2001.html6. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância de Doenças e Agravos Não Transmissíveis e Promoção da Saúde. Viva: instrutivo notificação de violência interpessoal e autoprovocada. 2
nd ed. Brasília (DF): Ministério da Saúde; 2016. [access in 24 set 2021]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/viva_instrutivo_violencia_interpessoal_autoprovocada_2ed.pdf7. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Vigilância de violências e acidentes no Brasil: análise da cobertura da notificação compulsória de violência interpessoal/autoprovocada nos municípios brasileiros. Bol Epidemiol. [periódico
on line]. 2020; 51 (4): 11-7. [access in 24 set 2021]. Available from:
https://saude.es.gov.br/Media/sesa/DANTS/viol%C3%AAncia-cultura%20de%20paz/CGDANT%202020%20(2).pdf8. Macedo DM, Foschiera LN, Bordini TC, Habigzang LF, Koller SH. Revisão sistemática de estudos sobre registros de violência contra crianças e adolescentes no Brasil. Ciên Saúde Colet. 2019; 24 (2): 487-96.
9. Sociedade Brasileira de Pediatria (SBP). 233 casos de violência física ou psicológica contra crianças e adolescentes são notificados todos os dias. Rio de Janeiro: SBP; 2019. [Internet]. [access in 2021 set 24]. Available from:
https://www.sbp.com.br/imprensa/detalhe/nid/233-casos-de-violencia-fisica-ou-psicologica-contra-criancas-e-adolescentes-sao-notificados-todos-os-dias/10. Paungartner LM, Moura JQ, Fernandes MTC, Paiva TS. Análise epidemiológica das notificações de violência contra crianças e adolescentes no Brasil de 2009 a 2017. Rev Eletr Acervo Saúde [periódico
on line]. 2020; 12 (9): e4241. [access in 2021 set 24]. Available from:
https://acervomais.com.br/index.php/saude/article/view/424111. Pereira VOM, Mascarenhas MDM, Ramalho WM, Shimizu HE, Ramalho WM, Fagg CW. Violências contra adolescentes: análise das notificações realizadas no setor saúde, Brasil, 2011-2017. Rev Bras Epidemiol. 2020; 23: e200004.
12. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Análise epidemiológica da violência sexual contra crianças e adolescentes no Brasil, 2011 a 2017. Bol Epidemiol [periódico
on line]. 2018; 49 (27): 1-17. [access in 2021 set 24]. Available from:
https://portaldeboaspraticas.iff.fiocruz.br/wp-content/uploads/2019/07/2018-024.pdf13. Levandowski ML, Stahnke DN, Munhoz TN, Hohendorff JV, Salvador-Silva R. Impacto do distanciamento social nas notificações de violência contra crianças e adolescentes no Rio Grande do Sul, Brasil. Cad Saúde Pública. 2021; 37 (1): e00140020.
14. Oliveira NF, Moraes CL, Junger WL, Reichenheim ME. Violência contra crianças e adolescentes em Manaus, Amazonas: estudo descritivo dos casos e análise da completude das fichas de notificação, 2009-2016. Epidemiol Serv Saúde. 2020; 29 (1): e2018438.
15. Lima ÁT, Sousa RPR, Clemente SMPS, Viana MAO, Porto E, Sousa JP,
et al. Epidemiological profile of violence against children and adolescents: an analysis of compulsory notifications in the State of Paraiba. Res Soc Dev. 2020; 9 (10): e1359108421.
16. Fattah N, Lima MS. Perfil epidemiológico das notificações de violência autoprovocada de 2010 a 2019 em um estado do sul do Brasil. Rev Eletr Saúde Mental Álcool Drog [periódico
on line]. 2020; 16 (4): 65-74. [acess in 2021 set 24]. Available from:
https://www.revistas.usp.br/smad/article/view/166310/17083917. Bahia CA, Avanci JQ, Pinto LW, Minayo MCS. Notificações e internações por lesão autoprovocada em adolescentes no Brasil, 2007-2016. Epidemiol Serv Saúde. 2020 ; 29: e2019060.
18. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Violência interpessoal contra pessoas com deficiência/transtorno no Brasil. Bol Epidemiol [periódico
on line]. 2020; 51 (46): 1-7. [access in 2021 set 24]. Available from:
https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/boletins-epidemiologicos/edicoes/2020/boletim_epidemiologico_svs_46.pdf19. Instituto de Estudos Socioeconômicos e Cartográficos. Secretaria de Estado de Programas Estratégicos. Boletim Social do Maranhão: os diversos tipos de violência no Maranhão. IMESC [periódico
on line]. 2020; 2 (4): 1-45. [access in 2021 set 24]. Available from:
http://imesc.ma.gov.br/src/upload/publicacoes/f48dc0929a2506771788426339d7185b.pdf 20. Silva SBJ, Conceição HN, Câmara JT, Machado RS, Chaves TS, Moura DES, Borges LVA, Moura RP. Perfil das notificações de violência contra criança e adolescentes. Rev Enferm UFPE. 2020; 14: e244171.
21. Sousa AYA, Pinho EFS, Silva JTN, Meireles ACV, Lago RJM, Silva WN, Moraes FC. Caracterização dos casos de violência sexual contra a mulher notificados no Estado do Maranhão no período de 2009 a 2017. Braz J Dev. 2021; 7 (1): 9925-41.
22. Lolli LF, Mesacasa D, Campos FNL, Silva NS, Oliveira VA, Fabiano GR. Violência praticada contra crianças e adolescentes no estado do Paraná: estudo retrospectivo do quinquênio 2010-2014. Braz J Health Rev. 2020; 3 (4): 11198-214.
23. Secretaria de Estado de Saúde do Rio de Janeiro. Subsecretaria de Vigilância em Saúde. Superintendência de Vigilância Epidemiológica e Ambiental. Panorama da violência interpessoal/autoprovocada a partir da análise sobre o preenchimento da ficha de notificação. Boletim Epidemiológico 001/2019. Rio de Janeiro: Secretaria de Estado de Saúde; 2020. [access in 24 set 2021]. Available from:
http://www.riocomsaude.rj.gov.br/Publico/MostrarArquivo.aspx?C=wdMTu5zzZ%2BE%3D 24. Ministério da Saúde (BR). DATASUS. 9. Violência interpessoal/autoprovocada - Maranhão [online]. Brasília (DF): Ministério da Saúde; 2019. [access in 2021 set 24]. Available from:
http://tabnet.datasus.gov.br/cgi/deftohtm.exe?sinannet/cnv/violema.def25. Ministério da Saúde (BR). DATASUS. População residente [online]. Maranhão. Brasília (DF): Ministério da Saúde; 2009 e 2019. [access in 2021 set 24]. Available from:
https://datasus.saude.gov.br/populacao-residente26. Reis ERL, Souza SJP, M MT, Weigert SP. Dificuldades dos profissionais de saúde em identificar e notificar a violência infantil. Rev Gestão Saúde. 2017 Nov; 17 (Supl.1 ): 63-70.
27. Instituto Brasileiro de Geografia e Estatísticas (IBGE). Síntese de indicadores sociais: uma análise das condições de vida da população brasileira. Rio de Janeiro: IBGE; 2018. [access in 2021 set 10]. Available from:
https://biblioteca.ibge.gov.br/visualizacao/livros/liv101629.pdf28. Mata NT, Silveira LMB, Deslandes SF. Família e negligência: uma análise do conceito de negligência na infância. Ciên Saúde Colet. 2019; 22 (9): 2281-8.
29. Instituto Brasileiro de Geografia e Estatísticas (IBGE). PNADC - Pesquisa Nacional por Amostra de Domicílios Contínua [Internet]. Brasília (DF): IBGE; 2019. [access in 2021 jun 15]. Available from:
https://cidades.ibge.gov.br/brasil/ma/panorama30. Pedroso MRO, Leite FMC. Recurrent violence against children: analysis of cases notified between 2011 and 2018 in Espírito Santo state, Brazil. Epidemiol Serv Saúde. 2021; 30 (3): e2020809.
Received on July 20, 2020
Final version presented on May 31, 2022
Approved on July 7, 2022
Associated Editor: Samir Kassar
Author's contribution: Silva VEO, Ribeiro MRC, Branco MRFC, Almeida JS, Gomes JA and Silva AAM: conceptualizations, methodology, analyses and writing of the manuscript. Marques MTS and Silva DPA: methodology, analyses, and writing of the manuscript. All authors approved the final version of the article and declare no conflict of interest.


 ; Marizélia Rodrigues Costa Ribeiro2
; Marizélia Rodrigues Costa Ribeiro2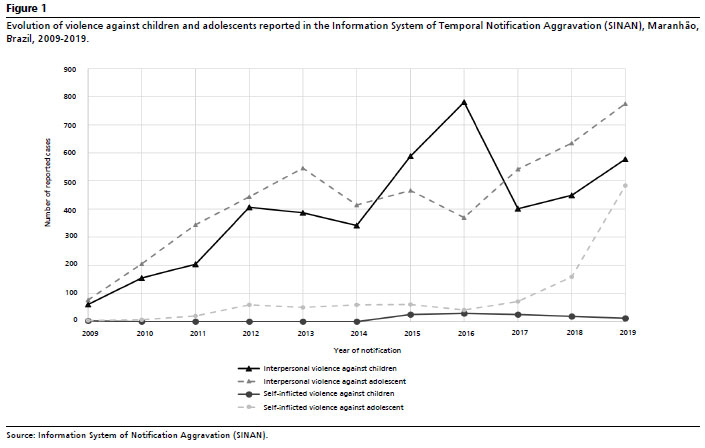







 Ler em português
Ler em português