ABSTRACT
OBJECTIVES: to investigate the association between the Índice de Qualidade da Dieta Adaptado para Gestantes (IQDAG) (Quality of Diet Index Adapted for Pregnant Women) with food consumption, lifestyle and health information.
METHODS: cross-sectional study with 110 pregnant women assisted at a public health service. Sociodemographic, nutritional and health data were collected from medical records. Food consumption was investigated through the usual intake, for a nutritional analysis, DietPro® program version 6.1 was used. Quality ofdiet was assessed using the IQDAG. Multinomial logistic regression was used to investigate an association between food consumption and IQDAG.
RESULTS: the average total score of the IQDAG was 61.3 (±26.1), this is the best quality of the diet. After adjusting for age, schooling and physical activity, the highest consumption of vitamin A (OR=1.04; CI95% = 1.02-1.07) and B2 (OR=2.63; CI95% = 1.19-5.70) was associated with a greater chance of having a better quality of diet (3rdtertile of the IQDAG).
CONCLUSIONS: pregnant women with better quality of diet had higher intakes of vitamins A and B2. However, other population-based studies are suggested to more broadly in verify its association with food consumption and its ability to identify adherence to nutritional recommendations.
Keywords:
Pregnancy, Food consumption, Quality of diet
RESUMO
OBJETIVOS: investigar a associação entre o Índice de Qualidade da Dieta Adaptado para Gestantes (IQDAG) com o consumo alimentar e hábitos de vida e informações de saúde.
MÉTODOS: estudo transversal com 110 gestantes atendidas em um serviço público de saúde. Os dados sociodemográficos, nutricionais e de saúde foram coletados a partir dos prontuários de atendimento. O consumo alimentar foi investigado por meio do recordatório de ingestão habitual, para a análise nutricional foi utilizado o Programa DietPro® versão 6.1. A qualidade da dieta foi avaliada utilizando o IQDAG. A regressão logística multinomial foi usada para investigar a associação entre o consumo alimentar e IQDAG.
RESULTADOS: a média da pontuação total do IQDAG foi 61,3 (±26,1), isto é uma melhor qualidade da dieta. Após ajuste por idade, escolaridade e atividade física, o maior consumo de vitamina A (OR=1,04; IC95%= 1,02-1,07) e B2 (OR= 2,63; IC95%= 1,19-5,70) esteve associado a maior chance da gestante apresentar uma melhor qualidade da dieta (3º tercil do IQDAG).
CONCLUSÕES: gestantes com melhor qualidade da dieta tiveram maior ingestão das vitaminas A e B2. Entretanto, sugere-se outros estudos de base populacional para verificar de forma mais ampla sua associação com o consumo alimentar e sua capacidade de identificar a adesão as recomendações nutricionais.
Palavras-chave:
Gestação, Consumo alimentar, Qualidade da dieta
IntroductionPregnancy constitute of an opportune time to promote and adopt healthier eating practices, since inadequate habits during this period can bring harmful health outcomes for both mother and child.
1The beneficial effects of improved quality diet include adequate gestational weight gain, lower maternal blood glucose concentration, and lower risk of preeclampsia.
2 For the child, the benefits include prevention of low birth weight, birth defects associated with micronutrient deficiency, and optimization of obstetric/fetal outcomes.
3Studies suggest that nutritional interventions during this period can produce positive effects,
1,4 by promoting the overall quality of the diet, with emphasis on the nutrients of interest in pregnancy.
5 The use of useful methods to evaluate the quality of the diet in this period of life is of great importance in health care.
Dietary indices are tools that allow to assess the complexity of the diet and monitoring its adequacy in relation to nutritional recommendations, based on predetermined dietary components.
6 In 2018, Crivellenti et al.
7 proposed the
Índice de Qualidade da Dieta Adaptado para Gestantes (IQDAG)( Quality of Diet Index Adapted for Pregnant Women), which presents nine components: three food groups, servings/1000 kcal (vegetables, fresh fruit, and legumes), five nutrients (omega 3, fiber, folate, calcium, and iron), and the percentage of the total energy value coming from ultra-processed foods.
It is noteworthy that this was the first national index to include in the guidelines of the new Food Guide for the Brazilian Population and the percentage of total calories from ultra-processed food as a moderator component, something that is relevant from the public health point of view,
7since they are currently widely consumed in Brazil, and for their impact on the nutritional quality of the diet and the risk of chronic diseases,
8 which may have a negative influence both for the pregnant woman and the baby.
Currently, dietary quality indexes have been considered important tools to evaluate the of individuals or groups' dietary intake, since they contribute to the development of better professional conduct, in addition to their low cost and practical application.
9To our knowledge, there are still no studies in the literature that evaluated the relationship between food intake and the quality of diet using the index adapted for Brazilian pregnant women. In order to contribute to the evaluation of this index as a tool to be used in the nutritional monitoring pregnant women, the objective of this study was to investigate the association between the IQDAG with food intake and characteristics of pregnant women assisted in a public health service.
MethodsThis is a cross-sectional study, which sample comprised of pregnant women to accompanied in the maternal and child nutritional care project (PROAMI) at the
Universidade Federal de Viçosa, (Federal University of Viçosa, Minas Gerais). The data are from care provided between December 2015 and March 2020. Data collection was performed in the medical records by a trained nutritionist and a nutritional student. Medical records that did not present information related to the pregnant women's diet, such as quantities, preparation methods, and measurements used were excluded, and adolescent pregnant women with chronic diseases (except obesity) and those who reported an energy intake below 500 kcal/day or above 3500 kcal/day were also excluded.
10Dietary intake was assessed by means of a usual intake recall collected at the first nutrition visit, regardless of the weeks of gestation. To calculate the nutritional value of food intake for pregnant women, the DietPro
® version 6.1 program was used. The Brazilian Table of Chemical Composition of Food (TACO) and the United States Department of Agriculture Research Service (USDA) were used to estimate the nutrients investigated (energy, carbohydrates, proteins, lipids, saturated fat, polyunsaturated fat, trans fat, fibers, vitamins A, C, B1, B2, B3, B6, B12, zinc, iron, folate, omega 3 and calcium).
11,12 To control the effect of energy intake on the nutrients evaluated, adjustment by the residual method was used.
13The quality of the pregnant women's diet was assessed using the IQDAG7 based on the recommendations of the Ministry of Health.
14To determine the IQDAG, two equations were used, the first to determine all the adequacy components (vegetables, legumes, fresh fruit, fiber, omega-3, calcium, folate, and iron). For intakes greater than or equal to the established cut-off points for these food and nutrient groups, a maximum score of ten points was assigned, and zero for no intake. The second equation was used to define the moderation component, which represents the percentage of total calories from ultra-processed foods, with zero as the minimum score and 20 points as the maximum value
7 (Table 1).
The intermediate values of the components were calculated proportionally and the final score of the index was obtained by the sum of all components, presenting a maximum value of 100 points. The IQDAG score was categorized in tertiles, adopting the first tercile as reference.
5,7 Below are the equations to calculate the IQDAG:
Equation 1 = 10* (QCIx-Min) / (Max-Min)
Equation 2 = 20* (Max-QCIx) / (Max-Min)
QCIx =value that corresponds to the amount of each component swallowed by the pregnant woman; Min= value for minimum score; Max= value for maximum score.
Sociodemographic data were obtained through a structured questionnaire containing the variables age, gestational age ranging from four (minimum GA) to 35 (maximum GA), number of children, parity, marital status, schooling and occupation.
The health profile was assessed by the report of current disease and information regarding supplement use, physical exercise, alcohol consumption, and smoking.
Pregestational weight was self-reported by the pregnant women, and those who did not remember, but were in the first trimester were considered their current weight. To measure current weight a Marte® digital platform scale was used, with an accuracy of 0.2g to 100g, and height was measured using a Stanley® stadiometer with an accuracy of 0.1 cm. Pregestational BMI was classified according to the World Health Organization (WHO) cut-off points and gestational nutritional status was calculated according to gestational age, based on the date of last menstrual period (LMP) when accurate or the expected date of delivery on ultrasound examination. We used the cutoff points proposed by Atalah, which evaluates the body mass index by gestational week, classifying into underweight, eutrophy, overweight, and obesity.
14-16 Pregnant women with overweight and obesity were grouped into "overweight" and those with underweight and eutrophy into the "not overweight" group.
Statistical analyses were performed in STATA for Windows, version 13.0. The data were submitted to descriptive analysis by means of estimates, standard deviation, median, interquartile range, as well as absolute and relative frequencies. The Shapiro-Wilk test was used to verify the normality of the variables. To compare food intake and pregnant women's characteristics between IQDAG tertiles, ANOVA and Kruskal-Wallis tests were used for continuous variables with and without normal distribution, respectively. The Kruskal-Wallis test with Dunn's post hoc was performed to compare the differences between the groups, and in the table groups that presented differences were represented by different letters. While for the categorical variables, Pearson's chi-square test, Fisher's Exact test or linear trend chi-square test was applied.
To investigate the association of IQDAG with nutrient intake, multinomial logistic regression was used, based on the Backward strategy, and variables with
p<0.20 in the bivariate analysis were included in the final model. The final model was adjusted for age, schooling, and physical activity, and the selection of variables was based on a literature review. The quality of model fit was assessed by the Hosmer-Lemeshow test, and was considered adequate when the test showed a
p value greater than 0.05 Sensitivity analysis was performed to re-estimate the associations by excluding eight pregnant women with current diseases (anemia, preeclampsia, and gestational diabetes mellitus). The level of statistical significance adopted in all analyses was
p<0.05.
The study was approved by the Ethics Committee on Research with Human Beings of the
Universidade Federal de Viçosa (Nº. 4.098.560), CAAE number 31465819.2.0000.5153, approved on June 19, 2020.
ResultsFrom a total of 116 medical records, five were excluded for not presenting quantities of food or home measures used, one of them was because the pregnant woman presented daily energy intake above 3500kcal, resulting in a final sample of 110 pregnant women.
The mean age was 34.3 (±5.5) years, mean gestational age at the first visit was 26.2 (±7.6) weeks, 67.6% had a partner and 74.8% were primiparous. As for changes in nutritional status, 20.7% were underweight and 32.4% were overweight at the current gestation. Of all pregnant women, 95.5% consumed some nutritional supplement, 60.4% did not practice physical activity, 2.7% consumed alcoholic beverages, 1.7% were smokers, 72.2% had no nausea in the past 30 days, and 1.8% had pyramalacia during pregnancy.
The sociodemographic characteristics, lifestyle, and health profile of pregnant women according to the IQDAG tertiles are presented in Table 2. No difference was found between the groups, except for the presence of current disease, which was more frequent in the 1
st tercile of IQDAG.
The mean (standard deviation) IQDAG total score value was 61.3 (±26.1) points, this is the bestquality of diet. Good quality of diet was verified regarding the intake of legumes (servings/1000 kcal) and omega 3, since most pregnant women reached the maximum score for these components. On the other hand, it was observed that most pregnant women did not reach the maximum score for the consumption of vegetables, fresh fruit, ultra-processed foods (% TEV), fiber, calcium, folate, and iron, demonstrating a poor quality of diet for these components (Table 3).
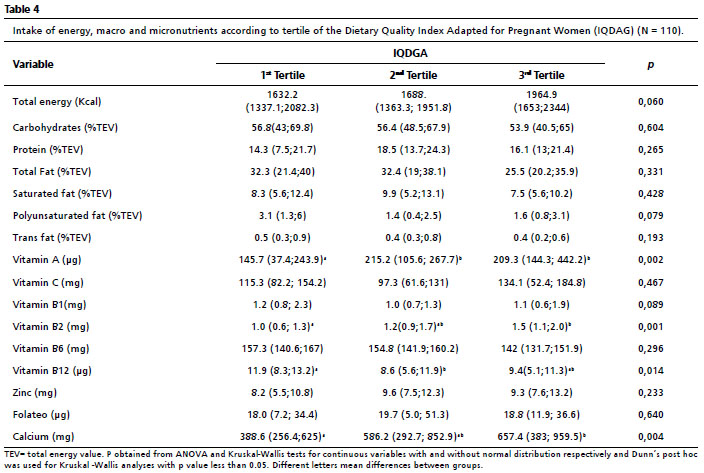
Table 4 presents the intake of macro and micronutrients according to IQDAG tertiles. Pregnant women in the 3
rd tertile had higher intakes of vitamins A, B2 and calcium than those in the 1
st tertile. On the other hand, the pregnant women in the 1
st tercil had a higher intake of vitamins B12 in relation to the 2
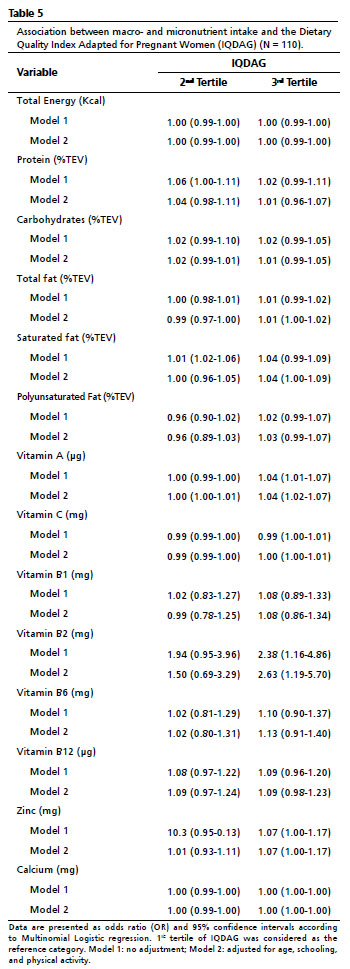
nd tercil. After adjusting for age, schooling and physical activity, the higher intake of vitamin A (OR=1.04; CI95%=1.02-1.07) and B2 (OR=2.63; CI95%=1.19-5.70) was associated with a higher chance of the pregnant woman presenting a better quality of diet (3
rd tertile of IQDAG) (Table 5). After exclusion of pregnant women with current diseases, only vitamin B2 remained associated with a higher chance of a better quality of diet (OR=2.65; CI95%=1.20-5.84).
DiscussionIn the present study, higher intake of vitamins A, B2 and calcium was observed in the group with higher quality of diet. After adjusting for other variables, a positive association between vitamin A and B2 intake and higher quality of diet was observed among pregnant women. Crivellenti
et al.
5 observed higher IQDAG scores among pregnant women with higher intake of carbohydrates, proteins, vitamins C, E, A, folate, minerals calcium and iron. Another study in Singapore also found higher calcium intake in pregnant women who were in the highest tertile of the Healthy Eating Index (HI).
17The need for vitamin A during pregnancy is critical not only for fetal growth and development, but also for maternal outcomes.
18 Likewise, maternal intake of vitamin B2 during pregnancy has also been independently and inversely related to emotional problems in infancy, in addition to affecting uterine growth, birth weight, fetal and placental epigenome.
19Unexpectedly, higher vitamin B6 and B12 intakes were identified in the group with the worst quality of diet. This may be explained by the fact that the index did not include food of animal origin, and that the two vitamins have their greatest sources in food of animal origin.
In this study, a higher frequency of current disease was observed in the first tertile of quality of diet. Another study evaluating quality of diet by the alternative healthy eating index suggested that a healthy eating pattern may decrease the excess risk of type 2 diabetes related to a higher genetic susceptibility.
20 In another study conducted in Finland, it was observed that pregnant women in the highest quartile of the IQD had a higher diversity of the intestinal microbiota compared to those in the lowest quartile.
21A good quality diet was observed regarding legume consumption (portions/1000 kcal), corroborating the results found in pregnant women in the cities of Ribeirão Preto, São Paulo and Rio de Janeiro.
7,22 One of the reasons for the high consumption of legumes may be that the mixture of beans and rice is the food culture of most Brazilians, and in addition to this, other legumes that are also most consumed are peas, lentils, and chickpeas.
23Good quality of diet was also observed in relation to the consumption of omega 3, similar to the result found by another study conducted in Ribeirão Preto, São Paulo.
7 This high consumption of omega 3 may be due to the high education level observed in the sample, with a higher prevalence of college-pregnant women. Another study observed that the higher the levels of schooling and maternal age, the higher the consumption of omega-3.
24However, this study observed that most pregnant women did not reach the maximum score for the intake of vegetables, fresh fruit, calcium, folate, fiber and iron. This result corroborates what has been found by other authors, in which a low proportion of women reached the maximum score for the intake of fresh fruit, fiber, calcium, folate, and iron, indicating poor quality of the diet in this aspect.
22 Another study identified that the nutrients with the highest inadequate intake were iron and calcium during pregnancy and lactation, because women did not change their eating habits during this phase, thus suggesting that guidelines should encourage the intake of healthy food for women throughout life.
25The low intake of iron was worrisome, since the needs for this nutrient during pregnancy are very high. Therefore, the Ministry of Health recommends prophylactic iron supplementation as a strategy to prevent and control anemia that has been very frequent in this phase,
23 and also as a way to prevent hypertensive syndrome of pregnancy, spontaneous abortions, placental abruption, premature delivery, low birth weight, fetal growth restriction, some chronic cardiovascular and cerebrovascular diseases, dementia, and depression.
26The use of dietary indices has numerous advantages, among which are the following: ease of obtaining a global view of the quality of the diet and not only of isolated components; they take into consideration the principles of variation, moderation, and proportionality,
27 mostly composed of nutrients and food groups, and the greater the number of dietary components, the more accurately it can reflect the dietary pattern of individuals or populations.
28The present study has some limitations: the use of secondary data allowed us to obtain only the information existing in the medical records, the use of self-reported pre-pregnancy weight, and the sample size may have been a limiting factor to identify some differences between the groups. On the other hand, its strength is the fact of having analyzed a new and specific index for pregnant women that adheres to the nutritional guidelines of the new Brazilian food guide, which contributes to the improvement of nutritional care to this group.
It was concluded that pregnant women with higher scores on the Quality of Diet Index had higher intakes of vitamins A and B2. However, further population-based studies are suggested to verify more broadly the association of the IQDAG with food intake and its ability to identify adherence to nutritional recommendations. Additionally, it is emphasized the promotion of consumption of healthy foods in this phase, aiming to improve the quality of the diet and consequently ensure favorable gestational outcomes.
References1. Muktabhant B, Lawrie TA, Lumbiganon P, Laopaiboon M. Diet or exercise, or both, for preventing excessive weight gain in pregnancy. Cochrane Database Syst Rev. 2015 Jun; 2015 (6): CD007145.
2. Rifas-Shiman SL, Rich-Edwards JW, Kleinman KP, Oken E, Gillman MW. Dietary Quality during Pregnancy Varies by Maternal Characteristics in Project Viva: A US Cohort. J Am Diet Assoc. 2009 Jun; 109 (6): 1004-11.
3. Pick ME, Edwards M, Moreau D, Ryan EA. Assessment of diet quality in pregnant women using the Healthy Eating Index. J Am Diet Assoc. 2005 Feb; 105 (2): 240-6.
4. Gomes CB, Malta MB, Louzada MLC, Benício MHD, Barros AJD, Carvalhaes MABL. Ultra-processed Food Consumption by Pregnant Women: The Effect of an Educational Intervention with Health Professionals. Matern Child Health J. 2019 May; 23 (5): 692-703.
5. Crivellentti LC, Zuccolotto DCC, Sarotelli DS. Associação entre o Índice de Qualidade da Dieta Adaptado para Gestantes (IQDAG) e o excesso de peso materno. Rev Bras Saúde Matern Infant. 2019; 19 (2): 285-94.
6. Kourlaba G, Panagiotakos DB. Dietary quality indices and human health: a review. Maturitas. 2009 Jan; 62 (1): 1-8.
7. Crivellenti LC, Cristina D, Zuccolotto C, Sartorelli DS. Desenvolvimento de um Índice de Qualidade da Dieta Adaptado para Gestantes. Rev Saúde Pública. 2018; 52: 59.
8. Monteiro CA, Cannon G, Levy R, Moubarac JC, Jaime P, Martins AP,
et al. NOVA. The star shines bright. World Nutr. 2016; 7 (1-3): 28-38.
9. Bressiani J, Martins LC, Honicky M, Mazur CE. Índices de qualidade da dieta oral: uma revisão bibliográfica. Ries. 2017; 6 (2): 94-102.
10. Loy SL, Chan JKY, Wee PH, Colega MT, Cheung YB, Godfrey KM,
et al. Maternal circadian eating time and frequency are associated with blood glucose concentrations during pregnancy. J Nutr. 2017 Jan; 147 (1): 70-7.
11. U.S. Department of Health and Human Services and U.S. Department of Agriculture. Dietary Guidelines for Americans. Washington (DC): US/DHHS/DA; 2005. 6
th Ed. [access in 2007 Jun 7]. Available from:
https://health.gov/sites/default/files/2020-01/DGA2005.pdf12. Lobstein A. La « Pharmacie de Charité» de Waldersbach, à l'initiative d'un pasteur-herboriste du XVIIIe siècle. Phytotherapie. 2005; 3 (3): 125-9.
13. Willett W, Stampfer M. Implications of total energy intake for epidemiologic analyses. Nutr Epidemiol. 2009; 124 (1): 17-27.
14. Ministério da Saúde (BR). Atenção ao pré-natal de baixo risco. Brasília (DF) : Ministério da Saúde; 2013. 1
st ed rev. [access in 2007 Jun 7]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/atencao_pre_natal_baixo_risco.pdf15. Atalah E, Castillo C, Castro R, Aldea A. [Proposal of a new standard for the nutritional assessment of pregnant women]. Rev Med Chil. 1997; 125 (12): 1429-36.
16. Hurria A, Cohen HJ, Extermann M. Geriatric oncology research in the Cooperative groups: a report of a SIOG special meeting. J Geriatr Oncol. 2010 Jun; 1 (1): 40-4.
17. Han CY, Colega M, Quah EPL, Chan YH, Godfrey KM, Kwek K,
et al. A healthy eating index to measure diet quality in pregnant women in Singapore: a cross-sectional study. BMC Nutr. 2015 Nov; 1 (1): 1-11.
18. Gannon BM, Jones C, Mehta S. Vitamin A requirements in pregnancy and lactation. Curr Dev Nutr. 2020 Oct; 4 (10): 1-18.
19. Miyake Y, Tanaka K, Okubo H, Sasaki S, Arakawa M. Maternal B vitamin intake during pregnancy and childhood behavioral problems in Japan: The Kyushu Okinawa Maternal and Child Health Study. Nutr Neurosci. 2020 Sep; 23 (9): 706-13.
20. Li M, Rahman ML, Wu J, DIng M, Chavarro JE, Lin Y,
et al. Genetic factors and risk of type 2 diabetes among women with a history of gestational diabetes: Findings from two independent populations. BMJ Open Diabetes Res Care. 2020 Jan; 8 (1): e000850.
21. Laitinen K, Mokkala K. Overall dietary quality relates to gut microbiota diversity and abundance. Int J Mol Sci. 2019 Apr; 20 (8): 1835.
22. Vieira MA, Sally EOF, Barbosa RMS, Ferreira DM. Qualidade da dieta de gestantes adolescentes assistidas na Rede Básica de Saúde. Saúde Pesq. 2020; 13 (3): 515-22.
23. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Programa Nacional de Suplementação de Ferro. Manual de Condutas Gerais. Brasília (DF): Ministério da Saúde. 2013; [access in 2007 Jun 7]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/manual_suplementacao_ferro_condutas_gerais.pdf24. Wilson NA, Mantzioris E, Middleton PF, Muhlhausler BS. Influence of sociodemographic, lifestyle and genetic characteristics on maternal DHA and other polyunsaturated fatty acid status in pregnancy: A systematic review. Prostaglandins Leukot Essent Fatty Acids. 2020 Jan; 152: 102037.
25. Santos Q, Sichieri R, Marchioni DML, Verly Junior E. Brazilian pregnant and lactating women do not change their food intake to meet nutritional goals. BMC Pregnancy Childbirth. 2014 Jun; 14 (1): 186.
26. Federação Brasileira das Associações de Ginecologia e Obstetrícia (FEBRASGO). Recomendação sobre a Suplementação Periconcepcional de Ácido Fólico na Prevenção de Defeitos de Fechamento do Tubo Neural (Anencefalia e outros defeitos abertos do tubo neural). Guia Prático Condutas. Rio de Janeiro (RJ): FEBRASGO; 2012. [access in 2007 Jun 7]. Available from:
http://189.28.128.100/dab/docs/portaldab/documentos/recomendacao_prevencao_dtn.pdf27. Volp ACP, Alfenas RCG, Costa NMB, Minim VPR, Stringueta PC, Bressan J. Índices dietéticos para avaliação da qualidade de dietas. Rev Nutr. 2010; 23 (2): 281-95.
28. Pinheiro AC, Nascimento R. Avaliação da qualidade da dieta pelo Índice de Alimentação Saudável e suas variações : uma revisão bibliográfica. Nutr Clín Diet Hosp. 2014; 34 (2): 88-96.
Received on September 2, 2021
Final version presented on August 24, 2022
Approved on December 12, 2022
Associated Editor: Leila Katz
Acknowledgments: We would like to thank the
Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) for the financial support.
Authors' contribution: All the authors contributed to the design, structuring, data analysis and interpretation, and critical review of the manuscript. The authors approved the final version of the article and declare no conflict of interest.


 ; Mariana De Santis Filgueiras2
; Mariana De Santis Filgueiras2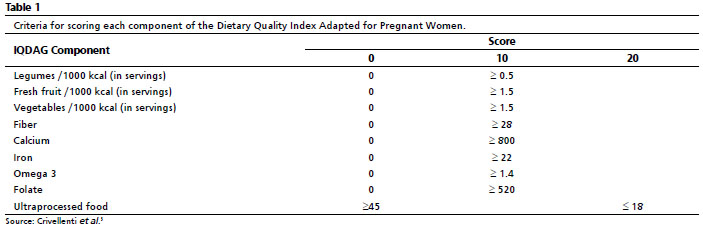








 Ler em português
Ler em português