ABSTRACT
OBJECTIVES: to evaluate the relationship between the ductus venosus (DV) and the variables of fetal growth in the first trimester in a Colombian pregnant population.
METHODS: a descriptive cross-sectional study was carried out with secondary data obtained from a multicenter study.526 patients were included between weeks 11 and 14 for gestational ultrasound follow-up attended in three health care institutions in Bogotá, Colombia, between May 2014 and October 2018. A bivariate descriptive analysis was carried out where the relationship between the characteristics of the DV in the first trimester and ultrasound findings.
RESULTS: the flow wave of the DV in the first trimester was normal in the entire sample, with a pulsatility index of the ductus venosus (DVPI) of 0.96±0.18. In addition, a negative correlation was found between the crown-rump length (CRL) and the DVPI (p<0.05).
CONCLUSION: there is a relationship between the DVPI regarding the CRL, indicating an interest in this early marker in relation to fetal growth alterations; however, more studies are required to determine the usefulness of this variable with respect to fetal growth.
Keywords:
First trimester, Doppler ultrasonography, Fetal growth, Crown-rump length
RESUMO
OBJETIVOS: evaluar la relación entre el ductus venoso (DV) y las variables del crecimiento fetal en primer trimestre en una población de gestantes colombianas.
MÉTODOS: se realizó un estudio transversal descriptivo con datos secundarios obtenidos de un estudio multicéntrico. Se incluyeron 526 pacientes entre las semanas 11 a 14 para seguimiento ecográfico gestacional atendidas en tres instituciones prestadoras de salud en Bogotá, Colombia, entre mayo del 2014 y octubre del 2018. Se realizó un análisis descriptivo bivariado donde se evaluó la relación entre las características del DV en primer trimestre y los hallazgos ecográficos.
RESULTADOS: la onda de flujo del DV en primer trimestre fue normal en la totalidad de la muestra, con un índice medio de pulsatilidad del ductus venoso (IPDV) de 0,96±0.18. Se encontró una correlación negativa entre la longitud cefalocaudal (LCC) y el IPDV (p<0.05).
CONCLUSIÓN: existe una relación entre el IPDV respecto a la LCC, señalando un interés de este marcador temprano en relación con las alteraciones del crecimiento fetal, sin embargo, se requieren más estudios para determinar la utilidad entre esta variable respecto al crecimiento fetal
Palavras-chave:
Primer trimestre del embarazo, Ultrasonografía doppler, Desarrollo fetal, Largo Cráneo-Cadera
IntroductionScreening for fetal growth disorders is of great importance as these pathologies favor deterioration and compromise fetal health.
1 Low birth weight has been associated with the development of coronary disease, non-insulin-dependent diabetes, and other chronic pathologies.
2 There is noknown biomarker at present that allows for the early prediction of the development of these diseases, therefore, screening is based on the routine measurement of fundal height, supplemented by the ultrasound measurement of fetal size in women who have pregnancy complications or relevant history.
3,4One of the ultrasonographic variables used infetal biometry to evaluategrowth is cephalocaudal length (CRL), which can be used to determine the date of pregnancy.
5 Additionally, there is evidence of its usefulness in the early detection of fetal growth alterations
6and the relationship that exists between the alteration of this marker and high-risk pregnancies.
7,8Ductus venosus (DV) is a hemodynamic marker for the screening, diagnosis, and prognosis of structural and functional changesin the fetus that may lead to pathological states, and thus, plays a key role in determining the fetal hemodynamic state.
9-12 It is a structure that facilitates the supply of oxygen from the umbilical vein directly to the brain and myocardium. Its assessment by Doppler ultrasonography allows for the indirect evaluation of fetal hemodynamic status, where changes are seen in its flow wave or pulsatility index in the event of deterioration due to physiological stress conditions, such as hypoxia and acidemia.
13-17Given the relationship between this vessel and the impact of placental insufficiency on fetal growth, this study is aimed at evaluating the relationship between DV and fetal growth variables during the first trimester in a population of pregnant Colombian women.
MethodsA descriptive cross-sectional study was carried outusing secondary data obtained from a multicenter study. Data were collected from a total of 566 patients who underwent ultrasound monitoring during their pregnancy at the Ecodiagnóstico El Bosque Prenatal Diagnosis Unit, the El Bosque Clinic, and the Suroccidente Health Services Unit - Hospital Occidente de Kennedy in Bogotá, Colombia, between May 2014 and October 2018. A total of 526 patients who met the following inclusion criteria were selected: pregnant women between 11 weeks and 13 weeks and 6 days of gestation who had undergone ultrasound follow-up. A total of 40 women were excluded, including pregnant women under 14 years of age, women who had losses during pregnancy, and women who did not have maternal and perinatal results.
Patients attended ultrasound evaluation during the first trimester between week 11 and week 13 and 6 days, where the sociodemographic, clinical, ultrasound (nuchal translucency [NT] and CRL), and gynecologic-obstetric variables (parity, history of full-term and preterm delivery, preeclampsia, and intrauterine growth restriction [IUGR]) were recorded.Fetal DV characteristics (pulsatility index and flow waveform) were assessed during fetal quiescence via ultrasound in a midsagittal plane with the fetuslying on its back. The image was enlarged until the fetal thorax and abdomen could be seenclearly. Subsequently, the DV that connects the umbilical vein with the inferior vena cava was visualized usinga color Doppler and medium insonation through the fetal abdomen at the hepatic level, where greater turbulence was observed, with an insonation angle of less than 30 degrees. Finally, the DV waveform was acquired using pulsed Doppler with a sample volume between 0.5 and 1.0 mm (Figure 1A),
18,19 and the DV normality references reported by Borrell
et al.
20 were used for the study. The CRL was measured on a sagittal plane by enlarging the image and with the fetus in a neutral position and measuring the maximum length of the fetus from the outer side of the crown of the head and to the rump. Gestational age was calculated and confirmed based on this measurement (in cm) taken using ultrasound from 11 to 13.6 weeks of gestation (Figure 1B).
21 Finally, postnatal outcomes were recorded, including maternal-perinatal diagnoses (preeclampsia and IUGR) and neonatal outcomes (gestational age, weight, height, APGAR, and Ballard scores, etc. ).

A descriptive analysis of the sociodemographic, ultrasound, gynecologic-obstetric, and postnatal characteristics was conducted to characterize the study participants by calculating simple and relative frequencies expressed as percentages for the qualitative variables, and measurements of central tendency and dispersion (mean and standard deviation) for quantitative variables. Furthermore, a bivariate analysis was carried out where the relationship between the characteristics of the DV and the ultrasound findings was determined. For the quantitative variables, normality was first evaluated with the Kolmogorov-Smirnov test and the homogeneity of variances was evaluated with the Levene test. As the assumptions were not met in eithercase, the non-parametric Mann-Whitney U test was used to compare groups and the Spearman correlation coefficient (ρ) was used to evaluate the relationship between the quantitative variables. A
p-value <0.05 was considered significant. The data were entered into an Excel database and the analyses were processed using the SPSS version 22 software package.
This project was approved by the Universidad El Bosque Ethics Committee, Minutes Nº. 026-2017.
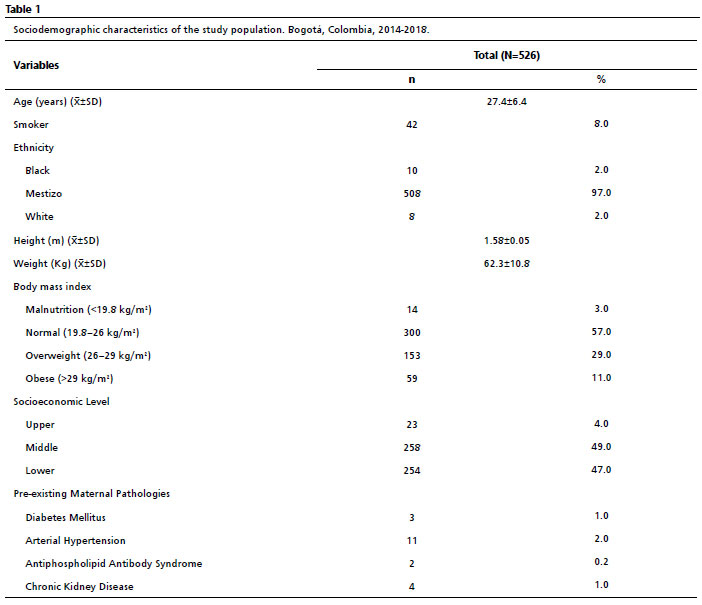
ResultsThe sample consisted of 526 pregnant women, with an average age of 27±6 years. It was also observed that 4.2% had pre-existing pathologies, with gestational diabetes and arterial hypertension being the most common. Table 1 shows the maternal sociodemographic and clinical characteristics.
The DV flow wave was normal in the entire sample (100%). Similarly, the mean pulsatility index during the first trimester was 0.96±0.1.
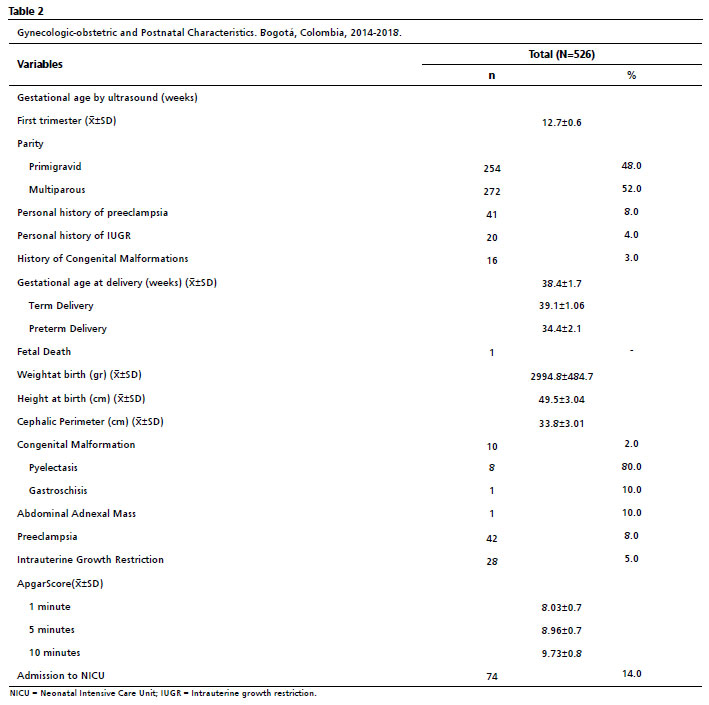
Regarding the gynecologic-obstetric variables (Table 2), for gestational age on ultrasound corresponding to the number of weeks at the time of assessment, the mean was 12.7±0.6 weeks in the first trimester. It was also found that 48% (254) of the pregnant women were primigravid and 52% (272) were multiparous.
In terms of the ultrasound variables in the first trimester, the mean NT was 1.58±0.4 mm, and the mean CRLwas 66.3±9.3 cm.
The postnatal results showed that the mean gestational age at delivery was 38.4±1.7 weeks. It should be noted that, out of the 526 patients, only one participant experienced fetal death in the 29th week of gestation. At the time of delivery, it was found that 5% of the pregnant women were diagnosed with IUGR and 8% had a diagnosis of preeclampsia. Regarding the neonates, theirmean weight at birth was 2994.8±484.7 g and mean height at birth was 49.5±3.04 cm. (Table 2).
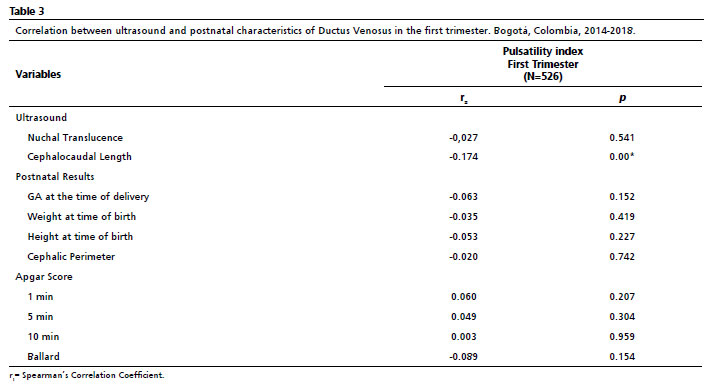
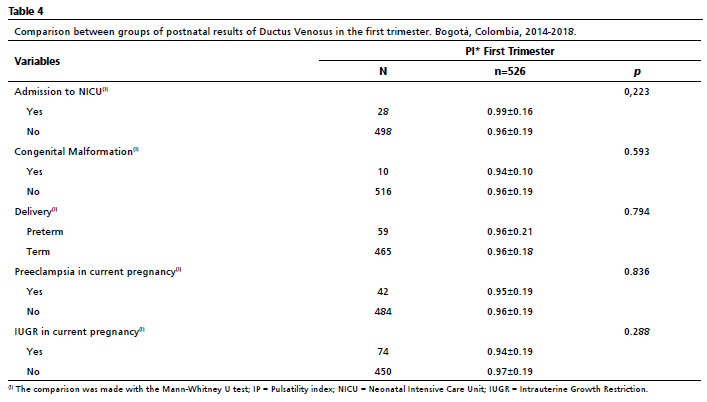
In the bivariate analysis of the DV variables in the first trimester using the ultrasound variables and the postnatal results, it was determined that the correlation between the CL and the DVPI in the first trimester was statistically significant (
p<0.05) (Tables 3 and 4). However, the correlation between DVPI and the rest of the ultrasound variables and postnatal results was not statistically significant.
DiscussionNormal fetal growth is a result of the interaction between potential growth (genetically predetermined) and the relationship between maternal and fetoplacental health
5. Ultrasound studies-together with the different ultrasound markers-are key tools for fetal evaluation throughout pregnancy since they help evaluate fetal development and facilitate the early detection of different pathological states, thus making an early management approach possible. DV is a characteristic used to study the fetal hemodynamic state whose alterations can provide valuable information about fetal-placental circulation.
13,14,22The behavior of DVregarding fetal biometry (CRL, TN) was characterized in the first trimester in this investigation, along with the sociodemographic, ultrasound, clinical, and postnatal characteristics of the pregnant women.This made it possible to highlight several findings, such as normal behavior of the DVduring the first trimester of pregnancy, and a negative correlation between DVPI and CRL.
We aimed to determine the relationship between intrauterine fetal growth and the DV marker in the first trimester. Changes in growth have an impact on fetal prognosis and adult life (the relationship between the presence of IUGR and cardiovascular disease in adulthood),
2 and follow-ups are critical in determining the prognosis of alterations in fetal growth. Thus, DVplays an important role in the detection of placental insufficiency, which when associated with hypoxia can alter fetal growth.
23-25 Therefore, we also aimed to analyze the relationship between the biometric parameter-CRL-in the first fetal trimester and DV, and found a negative correlation between DVPI and CRL in the first trimester (
p<0.05).
This relationship can be explained by the fact that this vessel grows along with the rest of the fetal structures as pregnancy progresses,
11 thus increasing the caliber of the DV and promoting a decrease in its resistance and, consequently, its pulsatility index. Therefore,as the size of the fetus increases, the resistance in the vessel is significantly reduced under normal conditions. Based on this correlation, the DVPI could be an early marker in determining growth alterations in the first trimester. To the best of our knowledge, there is no previous scientific literature that describes this relationship, therefore, DV should be studied as an early marker of abnormal fetal growth.
Among the strengths of this study are the sample size and the fact that it is one of the first studies in Colombia and Latin America to evaluate DV as a primary marker of fetal growth. One of the limitations of the study is the low frequency of fetuses with abnormal DV flow waveforms, although the most important limitation is the cross-sectional study design, which does not allow for causal inference. However, this design has not prevented us from determining the relationship between DVPI and CRL.
In conclusion, this study has demonstrated that there is a relationship between DVPI and CRL, which promotes the further study of this marker in relation to changes in fetal growth. However, more studies are required to determine the usefulness of this variable forfetal growth evaluation.
References1. Turan OM, Turan S, Gungor S, Berg C, Moyano D, Gembruch U,
et al. Progression of Doppler abnormalities in intrauterine growth restriction. Ultrasound Obstet Gynecol. 2008 Aug; 32 (2): 160-7.
2. Visentin S, Grumolato F, Nardelli GB, Di Camillo B, Grisan E, Cosmi E. Early origins of adult disease: Low birth weight and vascular remodeling. Atherosclerosis. 2014 Dec; 37 (2): 391-9.
3. Papageorghiou AT, Ohuma EO, Altman DG, Todros T, Ismail LC, Lambert A,
et al. International standards for fetal growth based on serial ultrasound measurements: The Fetal Growth Longitudinal Study of the INTERGROWTH-21st Project. Lancet. 2014 Sep; 384 (9946): 869-79.
4. Audette MC, Kingdom JC. Screening for fetal growth restriction and placental insufficiency. Semin Fetal Neonatal Med. 2018Apr; 23 (2): 119-25.
5. Committee Opinion Nº 611. Method for Estimating Due Date. Obstetr Gynecol. 2014 Oct; 124 (4): 863-6.
6. Salomon L, Hourrier S, Fanchin R, Ville Y, Rozenberg P. Is first-trimester crown-rump length associated with birthweight? BJOG. 2011 Sep; 118 (10): 1223-8.
7. Cho K, Dunne C, Albert AYK, Havelock JC. Adverse perinatal outcomes associated with crown-rump length discrepancy in in vitro fertilization pregnancies. Fertil Steril. 2018 Jan; 109 (1): 123-9.
8. Reljič M. The significance of crown-rump length measurement for predicting adverse pregnancy outcome of threatened abortion. Ultrasound Obstetr Gynecol. 2001 Jun; 17 (6): 510-2.
9. Nicolaides KH. A model for a new pyramid of prenatal care based on the 11 to 13 weeks' assessment. Prenat Diagn. 2011 Jan; 31 (1): 3-6.
10. Kiserud T. Hemodynamics of the ductus venosus. Eur J Obstet Gynecol Reprod Biol. 1999 Jun; 84 (2): 139-47.
11. Kiserud T. The ductus venosus. Semin Perinatol. 2001 Feb; 25 (1): 11-20.
12. Hernandez-Andrade E, Patwardhan M, Cruz-Lemini M, Luewan S. Early Evaluation of the Fetal Heart. Fetal Diagn Ther. 2017; 42 (3): 161-73.
13. Seravalli V, Miller JL, Block-Abraham D, Baschat AA. Ductus venosus Doppler in the assessment of fetal cardiovascular health: an updated practical approach. Acta Obstet Gynecol Scand. 2016 Jun; 95 (6): 635-44.
14. Braga M, Moleiro ML, Guedes-Martins L. Clinical Significance of Ductus Venosus Waveform as Generated by Pressure- volume Changes in the Fetal Heart. Curr Cardiol Rev. 2019 May 6; 15 (3): 167-76.
15. Baschat AA. Fetal responses to placental insufficiency: an update. BJOG. 2004 Oct; 111 (10): 1031-41.
16. Nardozza LMM, Caetano ACR, Zamarian ACP, Mazzola JB, Silva CP, Marçal VMG,
et al. Fetal growth restriction: current knowledge. Arch Gynecol Obstet. 2017 May 11; 295 (5): 1061-77.
17. Kanagawa T, Ishii K, Yamamoto R, Sasahara J, Mitsuda N. Fetal Outcomes Associated with the Sequence of Doppler Deterioration in Severely Growth-Restricted Fetuses. J Ultrasound Med. 2021 Nov 13; 40 (11): 2307-15.
18. The Fetal Medicine Foundation. Ductus venosus flow [
Internet]. [access in 2022 Mar 3]. Available from: https://fetalmedicine.org/fmf-certification-2/ductus-venosus-flow
19. Maiz N, Kagan KO, Milovanovic Z, Celik E, Nicolaides KH. Learning curve for Doppler assessment of ductus venosus flow at 11 + 0 to 13 + 6 weeks' gestation. Ultrasound Obstet Gynecol. 2008 May; 31 (5): 503-6.
20. Borrell A, Quintó L, Fortuny A, Boroblo V, Mercadé I, Goncé A,
et al. Translucencia nucal y ductus venoso: Valores de referencia en el primer trimestre de la gestación. Progresos Obstetr Ginecol. 2006 Aug; 49 (8): 434-40.
21. Bottomley C, Bourne T. Dating and growth in the first trimester. Best Pract Res Clin Obstet Gynaecol. 2009 Aug; 23 (4): 439-52.
22. Sandoval I, Véliz R, Sepúlveda Á, Candia AA, Herrera EA. Utilidad de la ecografía Doppler en el diagnóstico, el pronóstico y el manejo de la restricción del crecimiento fetal: situación en Chile. Rev Chil Obstet Ginecol. 2022 Jul 12; 87 (3): 218-28.
23. Turan Ş, Turan ÖM. Harmony Behind the Trumped-Shaped Vessel: the Essential Role of the Ductus Venosus in Fetal Medicine. Balkan Med J. 2018 Mar 15; 35 (2): 124-30
24. Pimiento Infante LM, Beltrán Avendaño MA. Restricción del crecimiento intrauterino: una aproximación al diagnóstico, seguimiento y manejo. Rev Chil Obstet Ginecol. 2015 Dec; 80 (6): 493-502.
25. Maršál K. Preeclampsia and intrauterine growth restriction: placental disorders still not fully understood. J Perinat Med. 2017 Oct 26; 45 (7): 775-7.
Received on November 18, 2021
Final version presented on September 22, 2022
Approved on October 27, 2022
Associated Editor: Alex Sandro Rolland
Acknowledgments: We thank the following health care centers: El Bosque Ecodiagnostic Prenatal Diagnosis Unit, El Bosque Clinic, and the Suroccidente Health Services Unit - Hospital Occidente de Kennedy, who provided their assistance, and all the pregnant women who participated in this study.
Authors' contribution: Ramírez MAM and Gamboa VMV: conception and design of the work, analysis and interpretation of the results, and writing and critical review of the manuscript.
Infante XCR: Conception and design of the work, collection/obtaining of data, analysis and interpretation of the results, and writing and critical review of the manuscript, patient contributions, or study material.
Calvo MU: conception and design of the work, collection/obtaining of data, analysis and interpretation of the results, and writing and critical review of the manuscript, patient contributions, or study material.
Hernández AMBP: Processing, analysis and interpretation of the results, methodological and statistical advice, and critical review of the manuscript.
The authors approved the final version of the article and declare that there are no conflicts of interest.


 ; Valentina María Vargas Gamboa2
; Valentina María Vargas Gamboa2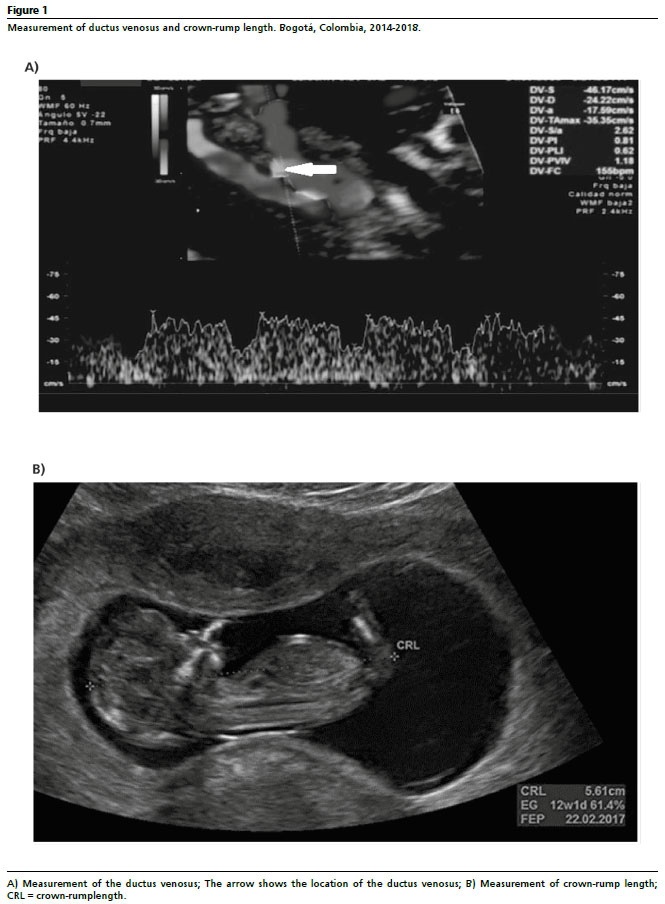






 Ler em português
Ler em português