ABSTRACT
OBJECTIVES: to analyze the trend and correlation of obesity and the increase in continued breastfeeding in children aged six to 23 months in Brazil, from 2015-2019.
METHODS: ecological time series study with data from the Sistema de Vigilância Alimentar e Nutricional (Food and Nutritional Surveillance System). The dependent variable was the prevalence of obesity. Prais-Winsten linear regression was used to verify the trend. Spearman's correlation was used to verify the relationship between the prevalence of obesity and the increase in continued breastfeeding.
RESULTS: there was a trend towards a reduction in the prevalence of obesity in all regions in Brazil (Annual Percentage Variation [APV]: -4.14; CI95%=-4.50; -3.79). The prevalence of continued breastfeeding showed an upward trend in the North (APV=4.89; CI95%=2.92; 6.90), Southeast (APV=3.36; CI95%=2.32; 4 .41) and South (APV=2.67; CI95%=0.98; 4.38). There was a negative and significant correlation between obesity and continued breastfeeding in the North, Northeast, Southeast and South regions.
CONCLUSION: the reduction in the prevalence of obesity and the increase in continued breastfeeding occurred only in some regions, requiring the implementation of effective strategies to be present throughout the country. Actions to promote, protect and support continued breastfeeding and healthy eating should be more prioritized to promote the child's healthy growth.
Keywords:
Obesity, Breastfeeding, Infant nutrition, Time series studies
RESUMO
OBJETIVOS: analisar a tendência e a correlação de obesidade e o aumento do aleitamento materno continuado em crianças de seis a 23 meses no Brasil, de 2015-2019.
MÉTODOS: estudo ecológico de série temporal com dados do Sistema de Vigilância Alimentar e Nutricional. A variável dependente foi a prevalência de obesidade. A regressão linear de Prais-Winsten foi usada para verificar a tendência. Adotou-se a correlação de Spearman para verificar a relação entre as prevalências de obesidade e o aumento do aleitamento materno continuado.
RESULTADOS: verificou-se tendência de redução da prevalência de obesidade em todas as suas regiões do Brasil (Variação Percentual Anual [VPA]: -4,14; IC95%=-4,50; -3,79). A prevalência do aleitamento materno continuado apresentou tendência de aumento nas regiões Norte (VPA=4,89; IC95%=2,92; 6,90), Sudeste (VPA=3,36; IC95%=2,32; 4,41) e Sul (VPA= 2,67; IC95%=0,98; 4,38). Houve correlação negativa e significativa entre obesidade e aleitamento materno continuado nas regiões Norte, Nordeste, Sudeste e Sul.
CONCLUSÃO: a redução da prevalência da obesidade e o aumento do aleitamento materno continuado ocorreram somente em algumas regiões, requerendo implementação de estratégias eficazes para esteja presente em todo o país. Ações de promoção, proteção e apoio ao aleitamento materno continuado e a alimentação saudável devem ser mais priorizadas para promover o crescimento saudável da criança.
Palavras-chave:
Obesidade, Aleitamento materno, Nutrição infantil, Estudos de séries temporais
IntroductionChildhood obesity has shown an increasing concern among Brazilian children in recent decades, from 1990 to 2010, becoming a public health challenge.
1 Overweight is a difficult condition to treat. Recognizing the protective or modifiable risk factors is a key aspect to prevent obesity and the development of diseases such as cancer and type 2 diabetes in childhood, conditions that may persist into adulthood, besides causing morbidity and mortality from heart disease.
2Children are the most affected by the ingestion of unhealthy food, because during childhood nutritional necessities are increased and both the scarcity and inadequate quality of food can trigger major health problems, such as low immunity, learning disabilities, increased infections, obesity, and in many situations, death.
3 Thus, childhood is a decisive period in relation to human health, especially when it comes to nutrition.
3,4Upto six months of age, breast milk is the ideal food for every child because of its nutritional composition, being rich in proteins, fat, and vitamins.
5 From six months to two years of age or beyond, continued breastfeeding (CBF) is recommended,
6 a factor that seems to have a significant effect on nutritional control throughout life.
7 Continued breastfeeding provides several benefits to the child, such as protection against infectious diseases, especially gastrointestinal and respiratory diseases, and reduces the chances of dyslipidemia, obesity, and diabetes.
8 Estimates from other studies show that continued breastfeeding could prevent, on average of 820,000 deaths in low- and middle-income countries.
8The
Sistema de Vigilância Alimentar e Nutricional (SISVAN) (Food and Nutrition Surveillance System) can be used to support early prognosis,
9 because it is a relevant source to promote greater assertiveness in planning actions and assist in the development of nutrition and food activities for the population assisted in local, state, and federal levels.
10In this context, it is important to analyze aspects related to children's health for a better elaboration of strategies and early health policies,
11 especially regarding eating habits and nutritional status. The recognition of the importance of breastfeeding for nutritional status in childhood and the relevance of adequate coverage of SISVAN to support the diagnosis of food and nutritional status at childhood
12 justify this investigation.
The article aimed to analyze the trend and correlation of obesity and BMI in children aged six to 23 months followed up in primary health care services in Brazil from 2015 to 2019.
MethodsThis is an ecological observational time series study conducted in Brazil, from 2015 to 2019, whose units of analysis were the
Unidades Federativas (UF) (Federative Units). SISVAN data about the nutritional status and food consumption of children aged six to 23 months assisted in the primary health care services linked to the
Sistema Único de Saúde (SUS) (Brazilian Public Health System) were used. SISVAN is publicly accessible and data are obtained through electronic reports via the web.
13The following filters were used to obtain the following indicators:
(a) nutritional status (obesity prevalence): reference year (2015-2019), reference month (all), grouped (State), UF (all), region (all), life stage (children from six to 23 months), anthropometric index (body mass index-BMI by age). BMI is calculated by dividing body mass in kilograms (Kg) and the height in square meters (m²), using the cutoff points as reference established by the World Health Organization (WHO) and used by the Ministry of Health.14
b) Food consumption (prevalence of continued breastfeeding): reference year (2015-2019), reference month (all), grouped (State), UF (all), region (all), life stage (children aged six to 23 months).
To determine the prevalence of obesity, the number of children aged six to 23 months with obesity (>99.9 percentile of BMI for age) was divided by the total number of registration of children of the same age in SISVAN, multiplying the result by 100. The prevalence of CBF was calculated by dividing the number of children aged six to 23 months with CBF by the total number of records of children of the same age in SISVAN, multiplying the result by 100.
The data were organized in Microsoft Excel 2013 and analyzed in Stata program version 14 (Stata Corp LP, College Station, USA). For the time trend analysis, the Prais-Winsten linear regression model was applied to estimate the annual percent change (APC) in the prevalence of obesity and CBF and their 95% confidence intervals (CI95%). The trends were considered increasing when p<0.05 and positive regression coefficient, decreasing when p<0.05 and negative regression coefficient, and stable when p>0.05.15 Spearman correlation was used to check for a monotonic relationship between obesity (dependent variable) and CBF (independent variable), considering a 5% significance level.
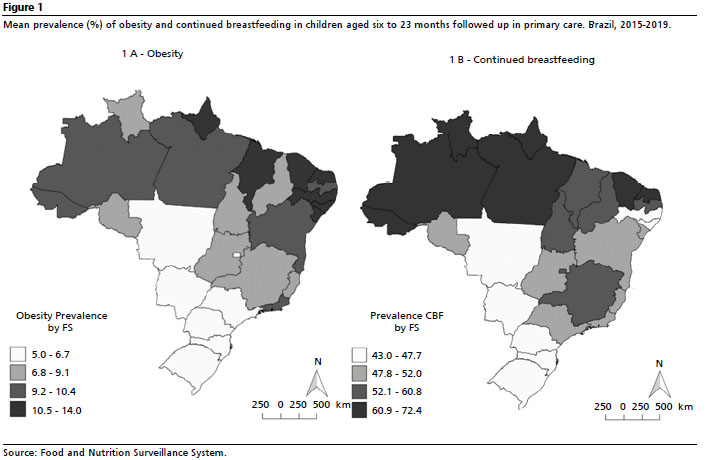
The distribution of the averages of obesity and CBF prevalence by UF was presented on maps built in the QGIS 2.18.23 Las Palmas program.
There was no submission to the Research Ethics Committee (CEP), because it is a study using a secondary database, available on public access websites, without any identification of the participants.
Results
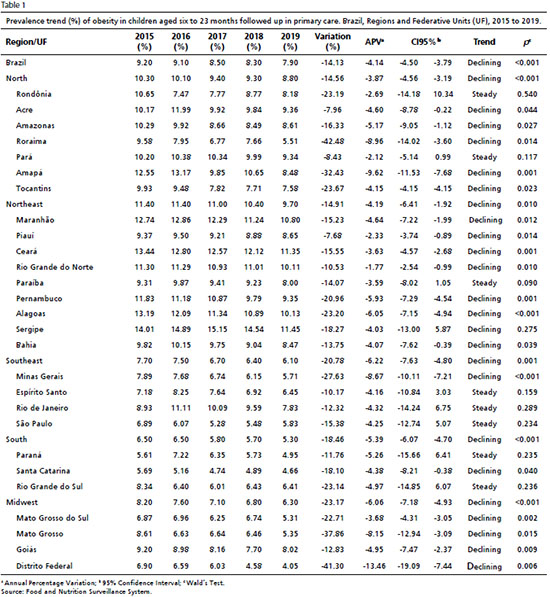
In the period from 2015 to 2019, an average of 1,350,000 children aged six to 23 months were followed up in the primary care services in Brazil each year. The prevalence of obesity among followed up children ranged from 9.20% in 2015 to 7.90% in 2019, with a decreasing trend in this period (APC=-4.14; CI95%=-4.50; -3.79). The decreasing trend in obesity prevalence was observed for all geographic regions, with the greatest reduction in the Southeast (APC=-6.22; CI95%=-7.63; -4.80), Midwest (APC=-6.06; CI95%=-7.18; -4.93) and South (APC=-5.39; CI95%=-6.07; -4.70) regions. The UFs with the highest annual percentage change in obesity prevalence were Distrito Federal (APC=-13.46; CI95%=-19.09; -7.44) and Minas Gerais (APC=-8.67; CI95%=-10.11; -7.21) (Table 1).
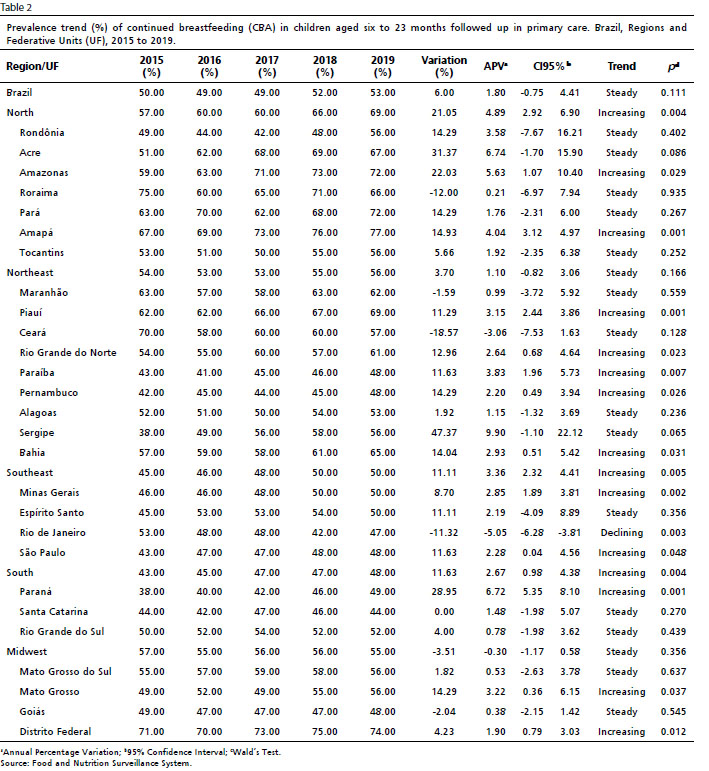
In the same period, the prevalence of CBF increased from 50.00% to 53.00%, with a mean annual increase of 1.80%, verifying a trend towards stability (APC=1.80; CI95%=-0.75; 4.41). There was a significant increase in the trend in the prevalence of CBF in the North (APC=4.89; CI95%=2.92; 6.90), Southeast (APC=3.36; CI95%=2.32; 4.41) and South (APC=2.67; CI95%=0.98; 4.38) regions.
The UFs showed an increasing trend in the prevalence of CBF were Paraná (APC=6.72; CI95%=5.35; 8.10), Amazonas (APC=5.63; CI95%=1.07; 10.40), Paraíba (APC=3.83; CI95%=1.96; 5.73), Mato Grosso (APC=3.22; CI95%=0.36; 6.15) and Minas Gerais (APC=2.85; CI95%=1.89; 3.81). Only the State of Rio de Janeiro showed a reduction trend in CBF prevalence (APC=-5.05; CI95%=-6.28; -3.81) (Table 2).
The highest mean prevalences of obesity were concentrated in the States of the Northeast region, being highest in Sergipe (14.01%), Ceará (12.46%), and Maranhão (11.09%). The lowest mean prevalence of obesity was found in Santa Catarina (5.03%), Distrito Federal (5.63%), and São Paulo (5.91%) (Figure 1-A). Most States in the North region had mean prevalence of CBF above 63%, being highest in Amapá (72.40%), Amazonas (67.60%), and Roraima (67.40%), while the lowest prevalences were found in Mato Grosso do Sul (43.00%), Mato Grosso (44.60%), and Pernambuco (44.60%) (Figure 1-B).
In Table 3 it is possible to verify negative and significant correlation between obesity and CBF. There was a reduction in the prevalence of obesity inversely proportional to the increase in the prevalence of CBF in the North, Northeast, Southeast, and South regions.
Discussion The results of this research showed that children on CBF had better results of nutritional status assessed according to BMI, compared to children who did not continue breastfeeding after six months of life.
At childhood, obesity can occur due to endogenous factors, such as hereditary problems, or exogenous, of behavioral, dietary, and/or environmental origin. The habits of family members or other individuals in the social environment in which the child lives and mirrors itself can influence children's eating habits.
16Combating childhood obesity can prevent chronic non-communicable diseases in adulthood such as cardiovascular accidents and diabetes, as well as orthopedic problems, dyslipidemia, hypertension, sleep apnea, gout, cancer, and psychological problems.
17 For this reason, the detection of overweight early in life is important, because it allows early interventions and prevention of future complications. The longer the obesity persists, the more difficult it will be for the treatment and the incorporation of new habits.
18Thus, monitoring the development and growth of children from birth and especially in the first year of life becomee essential.
19 It is during this phase that early weaning and/or the inappropriate introduction of complementary foods, both in quality and quantity, occurs. Moreover, early introduction of food is also associated with increased risk of malnutrition, more episodes of diarrhea, and poor absorption of relevant nutrients from breast milk,
19 in addition to obesity.
18Worldwide, between 1980 and 2014, the proportion of obese individuals more than doubled.
20 According to WHO, by 2020, about 40 million children under five years of age were identified as obese, and 340 million adolescents and children between five and 19 years of age were obese or overweight.
21A survey of children up to one year of age living in New York City (U.S.A)
22 found that 11.2% of the group investigated were considered obese. In a study conducted at Duke University with children and adolescents aged 2 to 19 years old on the prevalence of obesity and severe obesity, it was observed that the most prominent rates were found in adolescents, although an increase in severe obesity was observed among children aged 2 to 5 years old.
23It is projected that Brazil, in 2030, will occupy the fifth position in the ranking of countries with the highest percentage of adolescents and children with obesity, with little chance of reversing the picture. In a study conducted in 2019, nationwide, the prevalence of obesity in children under five years old was 10.1%. The region with the lowest prevalence was the Midwest (7.1%), which showed a statistically significant difference compared to the South, the region with the highest prevalence (12.0%).
21 Regarding children under two years of age, the states located in the Northeast region showed the highest percentages of obesity, especially Sergipe (14.4%), Ceará (11.8%), and Maranhão (11.2%).
24Despite the reduction in the prevalence of obesity found in this study, the Northeast region, especially the Sates of Sergipe, Ceará, and Maranhão, had the highest rates on obesity. This finding can be explained by the socioeconomic status of families, which is a determining factor for childhood obesity, influencing people's attitudes, especially in the choice and purchasing food.
11 Families with low socioeconomic conditions tend to offer food with high glycemic index through ultra-processed and processed food, rich in calories, fat and sugar. This socioeconomic context sedentifies and harms the child, making it evident that the social reality can characterize a blockage to meet the nutritional necessities of children with low financial status.
2The stability in the prevalence of CBF in children aged six to 23 months old when comparing regions in the period of 2015 to 2019 suggests an important factor to be analyzed. It is likely that there is an association between dose-response and duration of CBF, that is, the longer the breastfeeding period of the individual, the lower the possibility of developing obesity and/or overweight.
19 Despite the close relationship between CBF and obesity found in this study, there was no significant relationship in most UF in Brazil. This condition may be explained by the fact that the study considered age groups starting at 6 months of age, as, children who were already able to receive complementary feeding, and other Variables, could favor weight gain and reduce the influence of breastfeeding.
25The study was carried out with 566 children living in a city of São Paulo in the period 2004-2005 recognized that both CBF for six months or more and as CBF for 24 months or more constitute a protective factor against obesity and overweight.
24 A research done by WHO on the evidence of the protective effect of breastfeeding in the long term showed that children with continuous breastfeeding were 22 times less likely to be obese and/or overweight.
26The probable mechanisms that reduce the risk of obesity and/or overweight in breastfed children are due to the action of bioactive compounds present in human milk that, when associated with protein intake, promote satiety regulation. In addition, breast milk contains leptin, a hormone that acts directly on energy balance and appetite regulation, which contributes to protection against overweight and obesity in breastfed children.
25This study showed a negative correlation between CBF and obesity in almost all regions of Brazil, suggesting that breastfeeding works as an early protection factor in the prevention of obesity. Infants who are breastfed seem to have a greater ability to self-regulate food intake, which may be important for the establishment of healthy patterns of appetite regulation, favoring self-control of food intake according to needs. On the other hand, bottle-feeding and complementary feeding, administered by a caregiver, insensitive to the hunger and satiety signals emitted by the child, may favor overfeeding, consequently increasing the risk of childhood overweight and obesity.
27This study presented limitations because it is a survey with secondary data, susceptible to errors due to registration or typing errors and possible underreporting. Moreover, the results should be cautiously evaluated due to the ecological fallacy, in other words, one cannot make causal inferences regarding individuals based on group observations,
28 given the heterogeneous distribution of exposure and outcome variables within the groups themselves. However, despite the potential limitations, the study design allows us to obtain inferences at the population group level and contribute to strengthen actions to protect and monitor child health in Brazil.
Despite the downward trend in childhood obesity found in all the regions in Brazil, it is necessary to maintain and implement other effective actions for its reduction because of the serious consequences of this problem. CBF was shown to be increasing in most Brazilian regions; however, its consumption should be increasingly encouraged in order to promote healthy child growth.
References1. Camargos ACR, Azevedo BNS, Silva D, Mendonça VA, Lacerda ACR. Prevalência de sobrepeso e de obesidade no primeiro ano de vida nas Estratégias Saúde da Família. Cad Saúde Colet. 2019; 27 (1): 32-8
2. Sociedade Brasileira de Pediatria (SBP). Departamento de Nutrologia. Manual de orientação para a alimentação do lactente, do pré-escolar, do escolar, do adolescente e na escola. 3rd ed. Rio de Janeiro (RJ): SBP; 2012. [access in 2022 mai 2]. Available from:
https://www. sbp.com.br/fileadmin/user_upload/pdfs/14617a- PDManualNutrologia-Alimentacao.pdf3. Matos SMA, Barreto ML, Rodrigues LC, Oliveira VA, Oliveira LPM, D'Innocenzo S,
et al. Padrões alimentares de crianças menores de cinco anos de idade residentes na capital e em municípios da Bahia, Brasil, 1996 e 1999/2000. Cad Saúde Pública. 2014; 30 (1): 44-54.
4. Rayane DB, Sousa DHAV. Privação afetiva e suas consequências na primeira infância: um estudo de caso. Rev Inter Scientia. 2018; 6 (2): 51-62.
5. Ministério da Saúde (BR). Secretaria de Ciência, Tecnologia e Insumos Estratégicos. Departamento de Ciência e Tecnologia. Síntese de evidências para políticas de saúde: promovendo o desenvolvimento na primeira infância Brasília (DF): Ministério da Saúde; 2016. [access in 2022 mai 2]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/sintese_evidencias_politicas_primeira_infancia.pdf6. World Health Organization (WHO). Infant and young child feeding. Geneva: WHO; 2009. [access in 2022 mai 2]. Available from:
https://apps.who.int/iris/handle/10665/441177. Contarato AAPF, Rocha EDM, Czarnobay SA, Mastroeni SSBS, Veugelers PJ, Mastroeni MF. Efeito independente do tipo de aleitamento no risco de excesso de peso e obesidade em crianças entre 12-24 meses de idade. Cad Saúde Pública. 2016; 32 (12): e00119015.
8. Victoria CG, Barros AJD, Bahl R, Rollins NC, Horton S, Krasevec J,
et al. Amamentação no século 21: epidemiologia, mecanismos, e efeitos ao longo da vida. Epidemiol Serv Saúde. 2016; 2 (1): 1-24.
9. Rolim MD, Lima SML, Barros DC, Andrade CLT. Avaliação do SISVAN na gestão de ações de alimentação e nutrição em Minas Gerais, Brasil. Ciênc Saúde Colet. 2015; 20 (8): 2359-69.
10. Lima JF, Schmidt DB. Sistema de Vigilância Alimentar e Nutricional: utilização e cobertura na atenção primária. Rev Saúde Desenv. 2018; 12 (11): 316-33.
11. Matsudo VKR, Ferrari GLM, Araujo TL, Oliveira LC, Mire E, Barreira TV,
et al. Indicadores de nível socioeconômico, atividade física e sobrepeso/obesidade. Rev Paul Pediatr. 2016; 34 (2): 162-70.
12. Coelho LC, Asakura L, Sachs A, Erbert Y, Novaes CRL, Gimeno SGA. Sistema de Vigilância Alimentar e Nutricional/SISVAN: conhecendo as práticas alimentares de crianças menores de 24 meses. Ciênc Saúde Colet. 2015; 20 (3): 727-38.
13. Ministério da Saúde (BR). Secretaria de Atenção Primária à Saúde. Sistema de Vigilância Alimentar e Nutricional: relatórios públicos. Brasília (DF): Ministério da Saúde; 2022; [access in 2022 Jun 7]. Available from:
http://sisaps.saude.gov.br/sisvan/relatoriopublico14. Ministério da Saúde (BR). Orientações para a coleta e análise de dados antropométricos em serviços de saúde. Norma técnica do Sistema de Vigilância Alimentar e Nutricional - SISVAN. Brasília (DF): Ministério da Saúde; 2011. [access in 2022 Jun 9]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/orientacoes_coleta_analise_dados_antropometricos.pdf15. Antunes JLF, Cardoso MRA. Uso da análise de séries temporais em estudos epidemiológicos. Epidemiol Serv Saúde. 2015; 24 (3): 565-76.
16. Melo KM, Cruz, ACP, Brito MFSF, Pinho L.
Influência do comportamento dos pais durante a refeição e no excesso de peso na infância. Esc Anna Nery. 2017; 21 (4): 1-2.
17. Moreira MSF,Oliveira FM, Rodrigues W, Oliveira LCN, Mitidiero J, Fabrizzi F,
et al. Doenças associadas à obesidade infantil. Rev Odontol Araçatuba. 2014; 35 (1): 60-6.
18. Onis M. Prevenção do sobrepeso e da obesidade infantis. J Pediatr (Rio J. ). 2015; 91 (2): 105-7.
19. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Saúde da criança: nutrição infantil: aleitamento materno e alimentação complementar. Brasília (DF): Ministério da Saúde; 2009. (Série A. Normas e Manuais Técnicos) (Cadernos de Atenção Básica, nº 23) [access in 2021 Jun 9]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/saude_crianca_nutricao_aleitamento_alimentacao.pdf. 20. Ferreira APS, Szwarcwald CL, Damacena GN. Prevalência e fatores associados da obesidade na população brasileira: estudo com dados aferidos da Pesquisa Nacional de Saúde, 2013. Rev Bras Epidemiol. 2019; 22: e190024.
21. Universidade Federal do Rio de Janeiro (UFRJ). Estado Nutricional Antropométrico da Criança e da Mãe: Prevalência de indicadores antropométrico de crianças brasileiras menores de 5 anos de idade e suas mães biológicas: ENANI 2019. [Internet]. Rio de Janeiro (RJ): UFRJ; 2022. [access in 2021 Jun 9]. Available from:
https://enani.nutricao.ufrj.br/wp-content/uploads/2022/02/Relatorio_Estado_Nutricional-5.pdf22. Irigoyen M, Glassman ME, Chen S, Findley SE. Early onset of overweight and obesity among low-income 1- to 5-year olds in New York City. J Urban Health. 2008; 85 (4): 545-54.
23. Fryar CD, Carroll MD, Afful J. Prevalence of overweight, obesity, and severe obesity among children and adolescents aged 2-19 years: United States, 1963-1965 through 2017-2018. NCHS Health E-Stats. 2020; (1): 1-7
24. Simon VGN, Souza JMP, Souza SB. Aleitamento materno, alimentação complementar, sobrepeso e obesidade em pré-escolares. Rev Saúde Pública. 2009; 43 (1): 60-9.
25. Effect of breastfeeding on infant and child mortality due to infectious diseases in less developed countries: a pooled analysis. WHO Collaborative Study Team on the Role of Breastfeeding on the Prevention of Infant Mortality. Lancet. 2000; 355 (9202): 451-5.
26. Ministério da Saúde (BR). Secretaria de Política de Saúde. Organização Pan Americana da Saúde. Guia alimentar para crianças menores de dois anos. Brasília (DF): Ministério da Saúde; 2005. [access in 2022 jul 24]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/guia_alimentar_criancas_menores_2anos.pdf27. Ministério da Saúde (BR). Atlas da Obesidade Infantil no Brasil. Brasília (DF): Ministério da Saúde; 2019. [access in 2022 Set 11]. Available from:
http://189.28.128.100/dab/docs/portaldab/publicacoes/dados_atlas_obesidade.pdf28. Costa MFL, Barreto SM. Tipos de estudos epidemiológicos: conceitos básicos e aplicações na área do envelhecimento. Epidemiol Serv Saúde. 2003; 12 (4): 189-201.
Received on June 22, 2021
Final version presented on March 8, 2023
Approved on March 15, 202
Associated Editor: Lygia Vanderlei
Authors' contribution: Sousa AKS: elaboration of the study design, data collection and analysis, and manuscript review. Lima CEB: review of the manuscript content. Mascarenhas MDM: conception and planning, data analysis and interpretation. Rodrigues MTP: conception and planning, critical analysis of the manuscript writing.
The authors approved the final version of the article and declare no conflict of interest.


 ; Carlos Eduardo Batista de Lima2
; Carlos Eduardo Batista de Lima2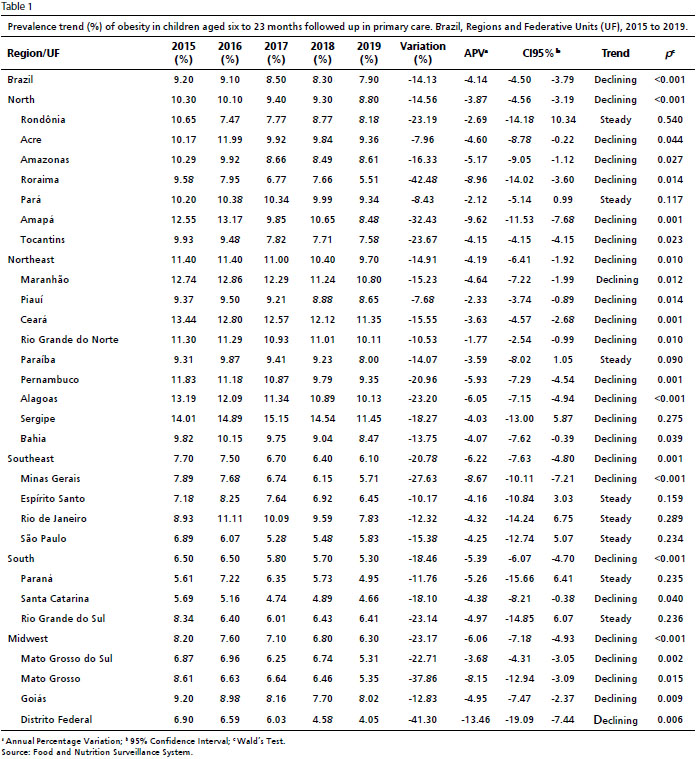







 Ler em português
Ler em português